Article Text

Statistics from Altmetric.com
Introduction
The use of research evidence to facilitate improvements in healthcare quality continues to be a topic widely debated by scholars and practitioners.1 ,2 The concept of ‘knowledge mobilisation’ has been developed, with strategies to help bridge this gap.3 These strategies include the development of “a culture of partnership between academic researchers and decision-makers to assist in strengthening the development of policy, practice and social innovation, or the co-production of knowledge”.3 ,4 It is based on the premise that knowledge that is collected and created ‘on the ground’, through daily interaction and negotiation with practitioners, managers and service users,4 will provide better insight into the issues affecting these stakeholders, be more relevant to the local context and will, therefore, be more easily incorporated into changes in practice.5–11
Different strategies have been used internationally to promote knowledge coproduction.12 Several of these strategies entail the creation of partnerships between academic and healthcare organisations.13–19 In some cases, these partnerships use ‘boundary spanners’,19 ,20 ‘knowledge brokers’21 or other intermediary roles,5 where individuals work to link practitioners with knowledge and develop organisational capacity to carry out and incorporate research into practice.18 ,22 One type of intermediary role is the embedded researcher. There are multiple definitions of embedded research and one of the goals of this review is to explore the wide range of meanings associated with this term. However, as a starting point, we used the definition proposed by McGinity and Salokangas,23 where embedded researchers are defined as those who work inside host organisations as members of staff, while also maintaining an affiliation with an academic institution. Their task is seen as collaborating with teams within the organisation to identify, design and conduct research studies and share findings which respond to the needs of the organisation, and accord with the organisation's unique context and culture.23 The role of embedded researchers differs from that of knowledge brokers and boundary spanners. Embedded researchers may use techniques used by knowledge brokers such as knowledge management, linkage and exchange and capacity building (based on the definition of knowledge broker used by5 ,6 ,21). Furthermore, they might operate as ‘boundary spanners’ in the sense that they work across organisational boundaries.5 However, their main purpose is to carry out research, to coproduce knowledge. The research is therefore produced through a collaborative and participative process, and it is jointly ‘owned’.23
The use of embedded researchers within and outside of healthcare appears to be a growing practice,14 but, to our knowledge, there are no published reviews of the characteristics of this approach, its potential role and the challenges it might face. Therefore, this review addresses the following questions. What are the characteristics of embedded research? What is the potential role for embedded researchers to facilitate improvement research that makes a difference? What are the challenges of such models? How can the lessons learned by embedded researchers in other sectors be applied to embedded research in healthcare? Our review synthesises the available literature on the experiences of researchers using the embedded research approach and presents a series of lessons learned for its application to research aimed at quality improvement in healthcare.
Methods
We carried out a narrative review24–26 to explore the role that embedded researchers could play in improvement efforts in healthcare. We conducted a two-stage bibliographic search of publications in English from 1937 to November 2015 using MEDLINE, Web of Science, PsychInfo, ProQuest Social Science and CINAHL Plus. In the first stage, we used the following search terms: ‘embedded research’ OR ‘embedded researcher’ OR ‘embedded researchers’ OR ‘researcher-in-residence’ OR ‘researcher in residence’ OR ‘boundary spanners’ OR ‘boundary spanner’. We included ‘boundary spanner’ as a search term to account for the work of researchers working across multiple organisations as this was an important aspect of the definition of embedded research we used as a starting point.23 Due to the contested nature of the definition of embedded research, we carried out a second stage of the search based on the identification of terms used in the articles that we included in the first stage of the review. These terms were: ‘intermediaries’ OR ‘transient government officials’ OR ‘embedded scientist’ OR ‘engaged scholar’ OR ‘knowledge broker’. In the same way, we iterated our search terms in this two-stage process, we also applied the working definition of embedded research outlined above flexibly in order to capture the wide range of approaches being employed in this emerging field (see under ‘Defining embedded research’ in Results section).
We conducted a review of bibliographies to identify further relevant publications and hand-searched the following journals: BMJ, BMJ Quality and Safety, Anthropology in Action, BMC Health Services Research and Implementation Science. These journals were selected based on our findings of the initial searches. Results were combined into RefWorks, and duplicates were removed.
The inclusion criteria were peer-reviewed journal articles focused on the embedded research approach both within and outside healthcare. The latter was included because the reflections on the process of carrying out research as part of an organisation in other sectors may be valuable for healthcare research. We excluded publications that were published in languages other than English.
The exclusion criteria are presented in figure 1. The included articles were analysed using a data extraction form developed in RedCap (Research Electronic Data Capture), which was created after the initial screening of full-text27 articles (see online supplementary appendix 1). We analysed the content of the articles in relation to the questions set out above. In addition, we captured themes emerging from the articles to include relevant issues not covered by our initial research questions.
{kind=link}
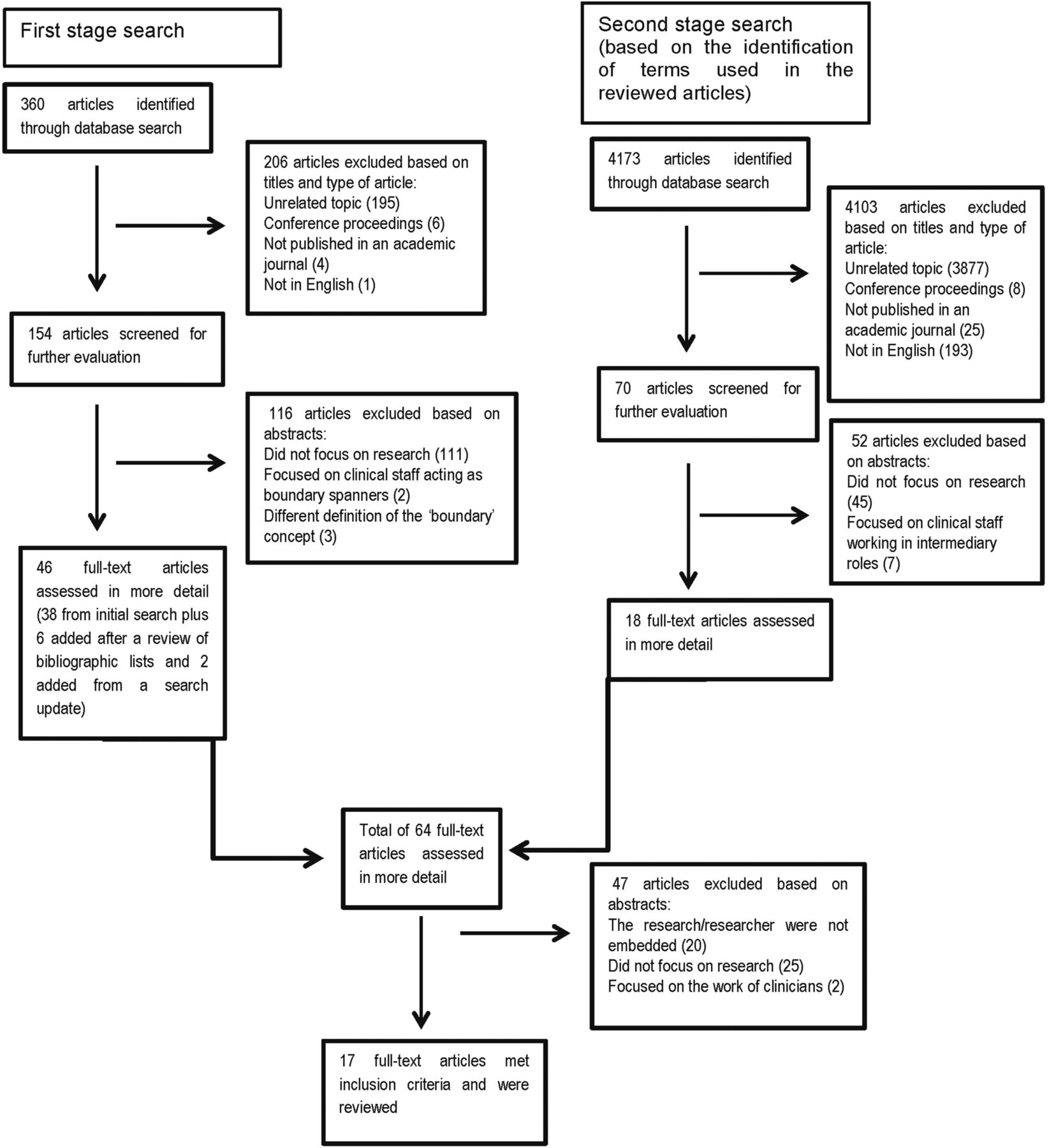
Flow diagram of publication selection process.
Supplementary appendix
Results
The first search yielded 360 published articles (see figure 1). The articles were screened in RefWorks by two of the authors (CV-P and TP) based on title, language, general topic, and type of publication, resulting in a total of 154 articles. Screening based on abstracts resulted in 38 articles for full-text review. The review of bibliographies yielded six more articles. The second search yielded 4173 articles; initial screening based on title led to 70 articles. Screening based on abstracts resulted in 20 articles for full-text review (see figure 1). The number of articles included for full-text review from both search stages was 64. After the full-text review, 47 articles were excluded. Seventeen articles were included in the final selection.
Our review of the literature indicates that the embedded research approach is an emerging trend within and beyond healthcare. Table 1 contains a description of the publications included in the review. The review contains eight healthcare-related publications and nine non-healthcare-related publications.
Characteristics of the articles included in the review and definition of embedded research/researcher
Defining embedded research
There is currently a wide spectrum of research activities that share characteristics that embody ‘embedded research’. While our working definition included a requirement that embedded researchers need to have dual affiliation (to an academic institution and the host organisation),23 we found that five of the articles included in the review did not discuss issues of dual affiliation. These articles, however, satisfied all of the other characteristics outlined in our working definition. One additional article clearly stated that the researchers were not affiliated to an academic institution while they were embedded. We included this article because the authors reflect on the positive and negative aspects of not having this dual affiliation. The approach we envision as embedded research is still in early stages of development, but despite variations in the affiliation of researchers, a series of common features can be identified (see box 1).
Characteristic features of embedded research
Researcher is usually affiliated to an academic institution as well as an organisation outside of academia, thus working in a state of ‘in-between-ness’.
Researcher develops relationships with staff and is seen as part of the team.
Researcher generates knowledge in conjunction with local teams (coproduced) which responds to the needs of the host organisation.
Researcher builds research capacity in the host organisation.
Becoming part of the organisation
Lewis and Russell37 regard it as essential that the researcher undergoes a process of immersion within his or her host organisation. By ‘being there,’ the researcher is able to grasp the challenges faced by the organisation, its goals and interests and the contexts where these play out.23 ,36 ,37
One of the main challenges of improving the quality of healthcare is the development of an organisational culture that is supportive and committed to improvement.1 As Dixon-Woods et al1 have argued, “problems can occur when improvement efforts run counter to centrally driven national pushes and pressures or are introduced into environments already suffering organisational stress from mandated requirements”. By being immersed in the organisation, the embedded researcher can gain greater understanding of the pressures and problems faced at different levels of the organisation and tailor improvement strategies accordingly.14 ,23
Developing relationships with staff
Physical presence alone is not enough to become an embedded researcher. As Wong34 highlights, an important component of ‘embeddedness’ lies in the quality and types of relationships the researchers foster with staff. Through these relationships, the researchers gain trust and are seen as members of the team.29 ,34 ,39 Their positionality, or the way researchers see themselves and are seen by others in the organisation, varies in relation to the people involved and the context.37 In his embedded work, Duggan39 established different collaborative relationships, such as: ‘critical friendship’ (working in equal relation to the project manager), ‘critical nephewship’ (working in a junior position) and ‘critical orphanship’ (unattached to the project team). These relationships allowed him to reach out and capture the views of staff at different levels of management, acting as an equal with some staff and in a more subordinate position with others. When acting as an ‘unattached’ researcher, he had more flexibility to participate in new activities within the organisation.
Establishing collaborative relationships with local teams is important for uncovering the different viewpoints of staff members regarding the issues faced by the organisation and how they could be addressed. This insight into the wide range of perspectives coexisting in the organisation can allow the researcher to make research findings more relevant to local end users, promote ownership of these findings and anticipate potential sources of tension produced by competing views.38 Improvement initiatives in healthcare frequently (but by no means always) emerge from the interests of senior groups within organisations who have particular ideas about the problems faced by the organisation, their causes and the best ways to solve them. These initiatives are often developed without the involvement of those who will experience changes in their daily practice and are imposed as a top-down measure.42 As a consequence, they often fail.1 The spread of innovations can also encounter similar obstacles when it is meant to intersect different groups and cross professional boundaries.43
Embedded researchers seek to tackle this issue of top-down approaches by considering the fact that each organisation has multiple subgroups with their own views of how the organisation works and how services should be organised.36 ,37 By working with these groups on an ongoing basis, embedded researchers are able to understand the complexity of the situations faced by the organisation and propose strategies that respond to the interests of a wider range of stakeholders.38
Critical reflection by the researcher and local team
Some authors argue that the creation of these collaborative relationships can be enriched when the researcher employs a reflexive approach.23 ,37 ,38 Reflexivity entails a conscious exercise of thinking about the position the researcher occupies as an individual, and as part of the organisational context.37 Reflexivity helps the researcher maintain a clearer idea of their role and capacity to intervene.38 It also supports a continuous reassessment and adjustment of the researcher's practice.34 When researchers are able to foster individual reflexivity, they become aware of potential barriers to the research process, and can thus adapt research activities to address the needs and interests of all involved parties, and create stronger relationships with the people participating in the research project.37 ,34 Furthermore, when shared with other members of the team in the form of collective reflexivity, this exercise provides a way of fostering critical thinking within the team even after the researcher leaves the organisation—a form of capacity building.34
Informing practice
Some have argued that in the traditional model of research, there is a disconnection between ‘producers’ and ‘consumers’ of research evidence.3 ,44 ,45 As a consequence, organisational decision-making is not always informed by health service research evidence.3 One of the goals of embedded research is the rapid delivery of research findings and their quicker incorporation into improvements in practice.14 Due to their immersion within the organisation, embedded researchers can produce research that is more relevant to the ‘end user’ and can give advice and flag issues in formal and informal ways.37 ,34
Having regular meetings with clinical teams and management groups to discuss progress of their work is proposed as a useful mechanism for the provision of iterative feedback.34 Such meetings are about discussing the research progress and maintaining relationships, and also about ensuring that all relevant members of the host organisation still feel they ‘own’ the problem, and will be willing to own the solution, too. The process of engaging staff to own the problem and support service improvement has been widely discussed in the healthcare quality improvement literature. Dixon-Woods and colleagues have argued that ‘soft’ and ‘hard’ tools might be needed to persuade staff to change current practices in healthcare organisations.1 ,46 Gollop et al47 have indicated that individualised and tailored influencing techniques, such as finding the right ‘hook’ when making the case for change, might be required to reduce some healthcare professionals' scepticism and resistance to service improvement.
Embedded researchers can use their presence and daily working relationships to implement some of these ‘soft persuasive tools’. The researcher might facilitate meetings, provide technical assistance to solve problems and share their knowledge of the research evidence. They might tailor feedback by weaving in the host organisation's own words or letting actors from the host organisation take the lead.
Due to their knowledge of the organisation's context and culture, the researcher is able to share the findings in relation to the wider issues at stake in the organisation, such as the need to scale-up interventions or combine the study with wider improvement initiatives taking place across the organisation.34 ,37 Furthermore, the researcher identifies and describes problems, and also cases of good practice,34 thereby helping to empower teams to continue with work that is producing positive outcomes.
Capacity building
In many cases, embedded researchers help build research capacity so that the benefits of embedded research extend beyond the researcher's direct involvement. Capacity building might include promoting a reflexive culture before launching new initiatives, creating awareness of less well-known ways to approach problems, establishing a research culture, teaching evaluation skills or assisting in applications for external funding.14 ,34 ,35 In contrast to other research approaches that tend to be based on the development of individual partnerships between researchers and staff, the embedded approach centres on the incorporation of research into the organisation's systems, processes and practices, thus promoting its sustainability over time.32 ,35
It is argued that embedded research also develops capacity at universities. It provides researchers with the opportunity to test methods and theories in practice—thus enhancing their applicability to real-life circumstances.14 ,23 ,39 Furthermore, the experience of working alongside healthcare professionals will help researchers later in their academic careers to design studies that generate insights helpful for healthcare organisations.23 ,33 ,36
The challenges of carrying out embedded research
Carrying out rigorous research within healthcare organisations is challenging. For instance, some authors mention their hesitation when contemplating designing research that could potentially lead to negative results or highlight undesirable qualities of the host organisation.34 When attempting to disseminate findings, researchers might be bound by internal regulations that prevent them from publishing information considered harmful by the host organisation.36 The dual affiliation of many embedded researchers places them in a state of ‘in-between-ness,’ where they have to show their commitment to the organisation's goals and to the academic standards established for conducting publishable research in their fields.37 ,38 This resembles the issues discussed in the literature on intermediary and boundary roles and the presence of role tensions or ‘role strain,’ a situation created when individuals have to deal with competing demands generated by members of the organisations they are affiliated to.48 ,49
One way to deal with the challenges connected with dual affiliation is to agree on clear guidelines from the beginning to manage expectations.50 The guidelines might define the role of the researcher, types of studies they will be able to undertake, study timeframes and feedback processes.14 ,34 Other embedded researchers have indicated that even if the researcher does not have an affiliation with an academic institution, it is important for him or her to maintain regular dialogue with academics about his or her research.29 ,37 A connection with academia allows embedded researchers to keep up to date on new trends, preserve a critical perspective and make sure their research is rigorous.37 It has also been recommended that embedded researchers should foster relationships with other researchers doing similar work and share lessons of how to manage day-to-day issues.29
This review has highlighted a number of lessons that may be useful for embedded researchers, and these are summarised in box 2.
Lessons learned from the use of embedded researchers within and outside of the healthcare sector
The embedded researcher needs to consider the experiences and points of view of the different subgroups within the organisation.
The creation of collaborative relationships with staff in the local organisation and the coproduction of knowledge can be enriched by practicing ‘reflexivity’ (reflecting on own position as an individual and as part of the organisational context).
Clear guidelines should be agreed between the embedded researcher and the local organisation from the beginning to manage expectations.
The researcher should schedule regular meeting with clinical teams and management groups to provide iterative feedback.
It is important for embedded researchers to maintain links with academic institutions to preserve a critical perspective.
Limitations of this review
This review has a number of limitations. There is a lack of consensus around the terminology used to refer to embedded research. Our search terms and screening process might not have captured all of the relevant articles.
Conclusion
Embedded research has the potential to address some of the main challenges in using research to improve quality in healthcare: understanding organisational culture to focus research appropriately, securing engagement from staff at different levels of the organisation to ensure the findings of research are translated into changes in practice and promoting the sustainability of improvement interventions.1 As Gold has argued, “in organisations, take up of ideas often occurs through informal processes”.51 The continuous presence of embedded researchers in healthcare organisations allows for the creation of these informal processes. The coproduction of knowledge between embedded researchers and local teams can lead to greater ‘ownership’ of the research findings by the healthcare organisation, and consequently, could lead to a smoother incorporation into changes in practice. The development of the research skills of local teams can help ensure research is viewed favourably and used within the organisation even after the embedded researchers have left.
Embedded research involves its own challenges in terms of dual affiliation, relationship building and sharing of results. Given our focus on the embedded research model as a method of coproducing research knowledge, we believe that maintaining a dual affiliation with health and academic organisations will represent a core component of embedded research. Learning from the experience of embedded researchers in different organisational contexts, and from the organisations they work with, could contribute further to our understanding of this approach. Rigorous evaluation of embedded research initiatives is required, which includes assessing the costs and benefits of embedded research for healthcare organisations.
References
Footnotes
Contributors CV-P, TP, MU and NJF conceived the idea for the review and participated in the design. CV-P and TP carried out the literature search, review and analysis of the selected publications. CV-P and NJF led on the drafting. All authors contributed substantially to writing the paper and all reviewed and approved the final draft.
Funding This paper presents independent research and was funded by the University College London Hospitals (UCLH) NHS Foundation Trust through matched funding to the National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care (NIHR CLAHRC) North Thames at Bart's Health NHS Trust.
Competing interests CV-P, NJF, MU and TP report grants from the University College London Hospitals (UCLH) NHS Foundation Trust through match funding to the National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care (NIHR CLAHRC) North Thames during the conduct of the study.
Provenance and peer review Not commissioned; externally peer reviewed.