Article Text

Abstract
Diagnosis is one of the most important tasks performed by primary care physicians. The World Health Organization (WHO) recently prioritized patient safety areas in primary care, and included diagnostic errors as a high-priority problem. In addition, a recent report from the Institute of Medicine in the USA, ‘Improving Diagnosis in Health Care’, concluded that most people will likely experience a diagnostic error in their lifetime. In this narrative review, we discuss the global significance, burden and contributory factors related to diagnostic errors in primary care. We synthesize available literature to discuss the types of presenting symptoms and conditions most commonly affected. We then summarize interventions based on available data and suggest next steps to reduce the global burden of diagnostic errors. Research suggests that we are unlikely to find a ‘magic bullet’ and confirms the need for a multifaceted approach to understand and address the many systems and cognitive issues involved in diagnostic error. Because errors involve many common conditions and are prevalent across all countries, the WHO’s leadership at a global level will be instrumental to address the problem. Based on our review, we recommend that the WHO consider bringing together primary care leaders, practicing frontline clinicians, safety experts, policymakers, the health IT community, medical education and accreditation organizations, researchers from multiple disciplines, patient advocates, and funding bodies among others, to address the many common challenges and opportunities to reduce diagnostic error. This could lead to prioritization of practice changes needed to improve primary care as well as setting research priorities for intervention development to reduce diagnostic error.
- Diagnostic errors
- Patient safety
- Primary care
- Health policy
- Information technology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Diagnosis is one of the most important tasks performed by primary care physicians (PCPs). The World Health Organization (WHO) recently prioritised safety areas in primary care and recognised the importance of errors in diagnosis.1 Recognising the paucity of literature,2–4 WHO set up a Safer Primary Care Expert Working Group to compile key lessons and topics for further research. This initiative led to the development of the 2016 Technical Series on Safer Primary Care, a series of 9 monographs to promote good practices and to implement systems changes to improve safety. This narrative review informed the development of the monograph focused on diagnostic errors, expected to be released by WHO in late 2016.
For multiple reasons, diagnosis in primary care (ie, first-contact, accessible, continued, comprehensive and coordinated care)5 represents a high-risk area for errors. PCPs typically face high patient volumes and make decisions amid uncertainty.6 Undifferentiated presenting features are the norm for diseases common in primary care, which tend to be benign and self-limiting, as well as uncommon diseases, which tend to be serious and life threatening. Diagnosis typically unfolds over time and across several episodes of care.7 ,8 PCPs need to carefully balance the risk of missing serious illness with the wise use of often scarce and costly referral and testing resources. Thus, diagnostic errors leading to patient harm from wrong or delayed testing or treatment have emerged as a global safety priority.9
Defining diagnostic errors
A diagnostic error occurs when a patient's diagnosis is missed altogether, inappropriately delayed and/or wrong, as judged by the eventual appreciation of definitive information10 but these categories of missed, delayed and wrong overlap extensively. For example, the following scenarios could involve an error in colorectal cancer diagnosis. The diagnoses can be considered ‘missed’ (cancer missed at three different primary care visits despite alarming symptoms), ‘wrong’ (patient told they have haemorrhoids at these visits but actually have cancer) or ‘delayed’ (patient had an abnormal laboratory test result, such as iron deficiency anaemia, suggestive of cancer but no one reviewed the results or notified the patient). But it is often hard to distinguish between the three; for example, in both missed and wrong scenarios, diagnosis was also delayed. Thus, these concepts have to be applied in concert to gain situational understanding. The evolution of diagnoses over time often makes it challenging to pinpoint a diagnostic error and operationalise diagnostic error definitions and measurements. The diagnostic process can also extend across multiple providers and in different locations. Moreover, there are no clear guidelines for ‘timely’ diagnosis for majority of conditions.11
Recent work has framed the diagnostic process along five process dimensions all of which must be considered in understanding diagnostic error.12 These dimensions include (1) the patient-provider encounter (history, exam, ordering tests/referrals based on appropriate assessment); (2) performance and interpretation of diagnostic tests; (3) follow-up and tracking of diagnostic information (such as abnormal tests) over time; (4) subspecialty and referral-related communication and coordination issues; and (5) patient behaviours, adherence and engagement. All five process dimensions are vulnerable to breakdowns in primary care, and sometimes more than one dimension is involved in an error.13–16
A recent Institute of Medicine (IOM) report ‘Improving Diagnosis in Health Care’ defines a diagnostic error as a “failure to establish an accurate and timely explanation of the patient's health problem or communicate that explanation to the patient.”14 Other formal definitions of diagnostic error have also been previously proposed.10 ,17 ,18 However, in this paper, we contextualise errors as missed opportunities that could be used to promote learning and improvement versus assigning blame or responsibility to a single clinician.18 The concept of missed opportunities also implies that something different could be done to prevent the error.
Three criteria should be considered when defining preventable diagnostic errors.12 ,19–22 First, an error should only be designated when case analysis reveals evidence of a missed opportunity to make a correct or timely diagnosis, that is, something different could have been done to make the correct diagnosis earlier.18 Such missed opportunities may result from individual cognitive or system-related factors, or more commonly interplay of both, or infrequently from more blatant factors such as lapses in accountability. Second, the missed opportunity is framed within the context of an ‘evolving’ diagnostic process such that error determination depends on the temporal or sequential context of events. This would imply that there is evidence of omission (failure to do the right thing) or commission (doing something wrong) at the particular point in time at which the ‘error’ occurred. Third, the opportunity could be missed by the provider, care team, system and/or patient.
A preventable error or delay in diagnosis may occur due to factors outside a single clinician's immediate control.3 Studies of diagnostic errors often involve some degree of hindsight bias—a type of bias in judgement about a diagnosis coloured by retrospective knowledge where earlier warning symptoms and signs are later found to be either overlooked or not considered seriously yet were less obvious when at the time of the actual encounter.23 Not all delayed/wrong diagnoses are accompanied by evidence of missed opportunities (areas C and D in conceptual model, figure 1) and not all missed opportunities are harmful (area A). Although the goal is to focus on preventable diagnostic harm (area B), this will require learning from all types of diagnostic error.
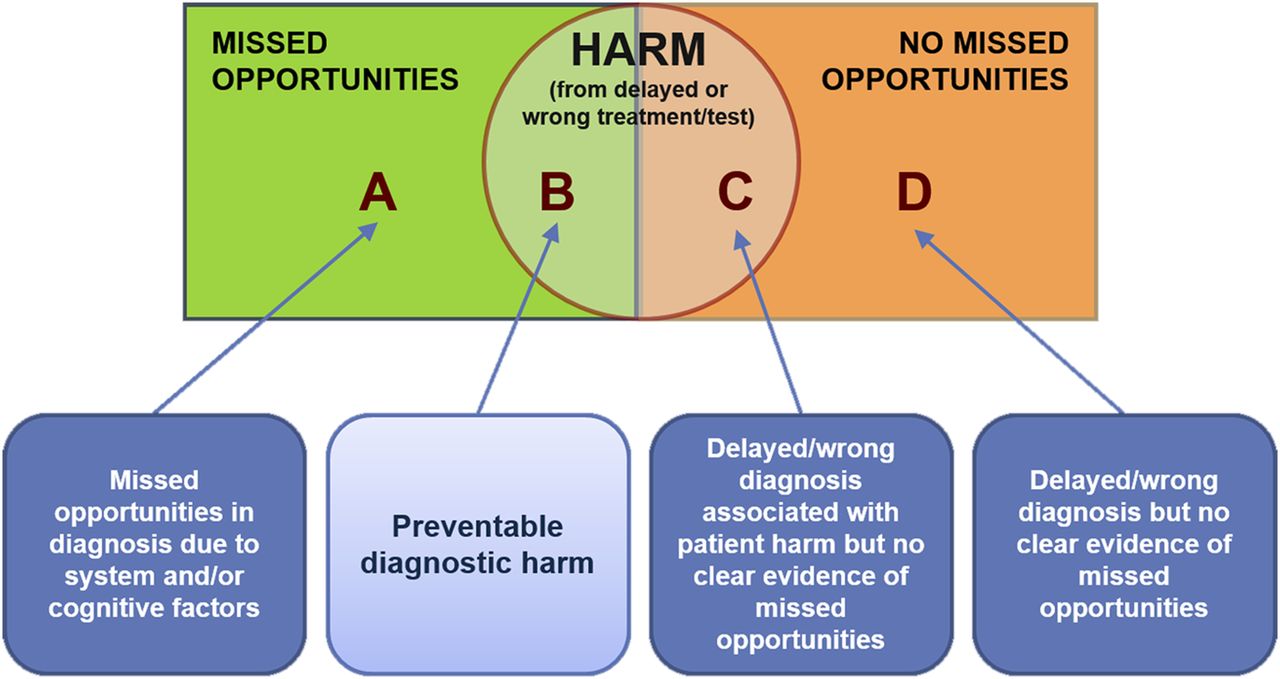
Relationships between diagnostic errors, missed opportunities and patient harm (adapted from Singh H).18
Epidemiology of diagnostic errors
A recent study estimated that about 5% of US adult patients experience diagnostic errors (defined as missed opportunities to make a correct or timely diagnosis or area A in Figure 1) in outpatient settings every year.24 Over half of these included the possibility of harm (area B). This was likely an underestimate, and it is unclear whether this rate would be similar in primary care in other countries, where data are generally lacking. Current US estimates are based on studies from integrated health systems using electronic health records that facilitate access to diagnostic data. A cross-sectional study of 12 primary care clinics in Malaysia reported a prevalence of errors of 3.6% (95% CI 2.2 to 5.0).25 While not representative of prevalence, in large studies of outpatient malpractice claims, diagnostic errors emerge as the most common category.26 ,27 Additional literature demonstrates evidence of diagnostic errors in primary care.28 ,29 The frequency of diagnostic error in paediatrics is unknown. However, a survey of US paediatricians found that more than half reported making a diagnostic error at least once or twice a month, and that they made harmful errors at least once or twice a year.30 Based on the available data, the IOM report ‘Improving Diagnosis in Health Care’ concluded that most people will likely have a diagnostic error in their lifetime.14
Diagnostic errors often reflect healthcare system complexities and vulnerabilities. In low-and-middle-income countries (LMICs; gross national income per capita below US$12 736),31 ,32 diagnosis poses even greater challenges as the process is further complicated by limited access to care and diagnostic testing resources, a paucity of qualified primary care providers and sometimes of specialists, and pre-electronic record-keeping systems. These factors likely suggest a higher rate of diagnostic errors in such settings compared with high-resource settings, though evidence for this is scarce (table 1).33 ,34 While access to primary care or specialists and limited availability of health professionals and diagnostic tests might lead to underdiagnosis in LMICs, high-resource settings might also be more prone to overdiagnosis because sophisticated imaging and laboratory testing, and subspecialty consultation, are all more accessible and there is greater concern about malpractice liability if a diagnosis is missed.
Factors that predispose to diagnostic errors in primary care settings
Typically, there are multiple ‘root causes’ in each error case. These include both cognitive errors such as failing to synthesise the available evidence correctly or failure to use the physical exam or test data appropriately. System flaws such as problems with communication or coordinating care, problems with the availability of medical record data and insufficient access to specialists are also contributory factors.10 ,12 ,35–38 A survey of 600 US PCPs identified typical concerns, such as settling too rapidly on a diagnosis, failing to consider an appropriately broad differential diagnosis or failing to order appropriate tests or consultations.39
High-risk situations
Studies on the relative frequency of conditions involved are largely from high-income countries. Reviews of diagnostic errors encountered in ambulatory care settings suggest that diagnostic errors may derive from routine as well as infrequent/rare conditions. Some of the conditions described in a systematic review included malignancies, myocardial infarction, meningitis, dementia, iron deficiency anaemia, asthma, tremor in the elderly and HIV.6 The observational study of 190 cases of diagnostic errors12 described earlier found that the most commonly encountered conditions involved pneumonia (6.7%), decompensated congestive heart failure (5.7%), acute renal failure (5.3%), cancer (5.3%) and urinary tract infection or pyelonephritis (4.8%).
Common diagnostic errors reported in a survey of PCPs included cancer, pulmonary embolism and coronary artery disease.39 Another survey of US internal medicine physicians reported both outpatient and inpatient errors related to pulmonary embolism (4.5%), drug reactions (4.5%), lung, colorectal and breast cancers (3.9%, 3.3% and 3.1%, respectively), acute coronary syndrome (3.1%) and stroke (2.6%).17 In a US study of 181 malpractice claims, cancer was the most common diagnosis involved.37 An analysis of 1000 negligent claims against the UK general practitioners identified diagnostic errors most commonly involving infections, trauma and cancer.40 Malpractice claims, however, tend to involve diagnoses that are more serious or most harmful if not diagnosed correctly in a timely fashion and do not necessarily represent error frequency. Nevertheless, infections, cardiovascular disease and cancer consistently emerge as the most significant categories of harmful diagnostic errors in the outpatient setting (table 2). Because children are frequently seen in primary care and are vulnerable to errors, we include them as a population at risk.
At-risk categories of harmful diagnostic errors
Interventions to reduce diagnostic errors
Physicians are often unaware of outcomes of their care, including their own diagnostic errors. Furthermore, both autopsy studies and vignette reviews show that physicians' diagnostic accuracy and the confidence they have in that accuracy are not always aligned.60 ,61 The marked decline of autopsies in recent years and absence of effective feedback mechanisms are factors that can lead to overconfidence and lack of appropriate calibration.33 ,62 Beyond raising awareness and developing effective strategies to deal with diagnostic uncertainty, a host of interventions targeting both cognitive-related and systems-related elements have been proposed, although few have been empirically tested.63 Systems-based interventions target all five dimensions mentioned earlier, whereas cognitive interventions seek to expand clinicians' knowledge and experience (eg, using simulation), improve clinical reasoning and decision-making skills or provide cognitive ‘help’ (decision support and second opinions).
While some interventions we consider here should logically improve diagnosis,2 current evidence of their effectiveness is limited.64 ,65 There is likely a need for multifaceted or multiple interventions.66 Recognising the lack of robust evidence of error reduction, we identify areas where interventions could be designed and tested (figure 2). We propose eight themes for interventions, all of which are grounded in ‘the Safer Dx framework’ to measure and reduce diagnostic error.13 The framework follows Donabedian's Structure-Process-Outcome model where the structural component is the ‘sociotechnical work system’ composed of various dimensions including people, technologies (particularly health information technologies), organisational policies and practices and external rules and regulations. Because errors arise from interactions among the various dimensions of the sociotechnical healthcare system, multiple components need to be simultaneously addressed by interventions. The ‘process’ aspects of the Safer Dx framework are defined by the five process dimensions described earlier in the Introduction. The ‘outcome’ is safe and efficient diagnosis (correct and timely, as opposed to missed, delayed, wrong) as well as long-term outcomes (eg, value, patient outcomes) related to healthcare delivery.

{kind=link}
{kind=link}
Potential interventions to reduce global burden of diagnostic errors. IT, information technology; POCT, point-of-care testing.
Improving diagnostic reasoning
Studies of PCPs who recounted diagnostic errors highlight failures in all stages of the diagnostic process.6 ,17 ,67–69 Several experimental studies have highlighted reasoning biases, in relation to both hypothesis generation and information interpretation in PCPs. Certain aspects of diagnostic reasoning67 might be more important, more common or more amenable to interventions. Interventions that could potentially improve clinical reasoning include advice to practice reflectively,70–72 use of tools such as mnemonics and checklists,73 and web-based decision support products that assist with differential diagnosis.74–76 ‘Debiasing’ has been proposed as an approach to eliminate subconscious biases that contribute to error.77 ,78 While many find the idea of focusing on cognitive biases and heuristics to improve clinical reasoning appealing, physicians find it difficult to characterise specific biases with any reliability and identify twice as many biases when outcome implies incorrect versus correct diagnosis.79 ,80 Knowledge is still key to diagnostic accuracy and efforts to promote it essential.81
Improving reliability of diagnosis requires reforming training and medical education for PCPs and including concepts related to the ‘basic science’ of diagnostic error.82 PCPs would also benefit from working in blame-free and improvement-focused systems that focus on feedback and error analysis as tools to improve performance. They need an environment that transforms errors into learning opportunities.
Encouraging government policies that support primary care
Robust government policies focusing on strengthening primary care systems and making it safe and effective while seem logical83 ,84 are often not well implemented. Specific strategies, some of which are more challenging for LMICs,85 include enhancing access to care and appropriate expertise, ensuring the competency of PCPs and primary care teams,86 making available high-quality diagnostic testing services (radiology/laboratory), providing a suitable work environment with safe and effective health information technology (IT) and improving access to reference information resources.87
In areas where access to primary care is limited, non-physician healthcare workers provide primary care, and in some cases have made considerable impact on health indicators,88 often using simple clinical algorithms such as the WHO's Integrated Management of Child Illness.89 However, adequate access to trained PCPs and specialists needs to be ensured for more challenging cases or when specialised diagnostic procedures are required. Short-term policies should prioritise conditions that can be improved with relatively minor investments, such as cancer or infection diagnoses or improved follow-up of patients seen for emergency care.
Improving information technology
Assuming internet access is available, an attractive option for improving access to appropriate expertise is the use of new technology that enables remote consultation and diagnosis. Remote reading of radiology imaging was a pioneering area,50 and the applications of remote diagnosis have expanded to include cardiology, ophthalmology, pathology, dermatology and even mental health. These resources enhance access to subspecialty expertise, often in real-time and can be particularly valuable for remote or dispersed clinical settings. Moreover, health IT can support diagnostic reasoning90 and promote detection of errors and follow-up and tracking.91 ,92 Deploying health IT-based interventions requires a coordinated plan to provide safe and effective hardware and software that support processes, users and workflow, as well as organisational support.93 Health IT approaches, tools and algorithms could be used in several steps of the diagnostic process in order to reduce diagnostic errors.87 These steps could include traditional steps of data gathering and broadening differential diagnosis but also novel ways to improve patient follow-up,94 detecting diagnostic errors via novel use of ‘triggers’22 ,95 ,96 and enabling diagnostic feedback to clinicians.97
Involving patients
Engaging and empowering patients is another low-cost investment with large potential to leverage improvement.98 Patients can act as a safety net by educating them what symptoms to look for, on the expected time course of their illness and how to re-access care if their condition does not improve or new symptoms emerge. In addition, patients can be proactive in ensuring diagnostic test results are reviewed. They can prompt providers to think comprehensively of a differential diagnosis (such as asking ‘what else do you think this could be?’), access medical knowledge on their own through reliable web sources and help prevent diagnostic errors by participating in follow-up and feedback.99–101 Ensuring longitudinal patient follow-up beyond the consultation is particularly important in primary care, given the non-specific presentation and evolution of many serious diseases over time.102 Patient empowerment includes dispelling misconceptions such as ‘no news is good news’ from the doctor (which could contribute to failures in follow-up of abnormal test results) and encouraging them to raise their diagnostic concerns or fears without feeling intimidated by the physician. However, this can be challenging in passive or paternalistic cultures, requiring a cultural reacclimation of both patients and providers. Allowing patients access to their medical records has substantial potential to improve diagnostic reliability.
Improving access to diagnostic tests
In addition to improving access to appropriate diagnostic tools for common infectious conditions such as pneumonia and diarrhoea,103 more focus is needed on non-communicable diseases (NCDs), which require laboratory or imaging tests for accurate diagnosis and monitoring.104 A recent WHO report points to a global cancer epidemic by 2025, which should be a high-priority area for future interventions given high rates of delayed cancer diagnosis and the difficulties with making diagnoses based on clinical features alone.19 ,20 ,105 Pathology and imaging services to support diagnostic testing are often limited in LMICs. Although plain radiography is available in many first-contact settings, access to more sophisticated imaging, including ultrasound, can be limited.
In many LMICs where centralised/referral laboratories are unavailable, point-of-care testing (POCT) may offer improved access to diagnostic and monitoring laboratory tests. A recent survey of PCPs in five countries highlighted the variation in POCT adoption and prioritised them for further development and implementation, but we need to demonstrate their effectiveness, including cost-effectiveness.106 In addition to developing, evaluating and implementing cost-effective POCT techniques for common conditions, healthcare personnel need to be trained on how to use them, and the testing, interpretation and reporting processes need appropriate oversight.
Developing methods to identify and learn from diagnostic errors
Current measures of quality of care in primary care are not focused on diagnostic error.107–109 To routinely assess the quality of diagnostic care, we need methods to better identify and define diagnostic errors. Promising approaches include designing triggers to identify patient records that may contain diagnostic errors,110 assigning ‘clinical champions’ to encourage physician reporting and learning from errors,111 and identifying and fixing process breakdowns in the follow-up of abnormal findings.3 ,96
Finding and analysing individual cases of diagnostic error through non-punitive and non-defensive discussions provide a unique opportunity to understand the problem and explore solutions.112 To minimise hindsight bias that arises when events are reviewed retrospectively, it is helpful to play forward rather than backward to see if a different set of appropriate actions/judgement emerge. The goal is to understand why the actions (or inactions) made sense at the time, and what could be improved in the future.113 Actions that worked well should also be highlighted.
Optimising diagnostic strategies in primary care
Research is needed to define how best to manage uncertainty, delineating the diagnostic value and time course of emergence of individual and combinations of clinical features. More evidence is also needed for the validation, best uses and impact of clinical prediction rules in primary care—many of which remain untested in this setting.114 Research on optimising knowledge access in frontline care is needed. Many knowledge-related diagnostic questions during practice go unanswered as busy physicians move on to the next patient.113 For many reasons, diagnostic decision support programmes are underused, with physicians mainly citing lack of time and concerns about their efficiency and utility.115
Providing systematic feedback to clinicians about their diagnoses
In addition to learning from their own (and others') errors, physicians need to continuously refine and recalibrate their diagnostic skills. Improving feedback to PCPs is consistent with good engineering principles, but is generally minimal or absent in primary care.62 One fertile area for investigation is the potential impact of feedback on competency in diagnostic reasoning62 and what roles patients could play here. Research is also needed to identify the most practical and effective methods of providing feedback to PCPs, and how to implement systems that encourage practitioners and systems to learn from diagnostic errors (and diagnostic successes). One model is the Confidential Enquiry approach used in several countries,116 ,117 which can explore reasons for underlying catastrophic diagnostic errors and help identify priority actions. This approach uses expert panels and local clinicians to perform detailed case reviews of a series of patients who suffered poor outcomes (usual fatalities) in a non-judgemental multiperspective process.
Next steps for policy, practice and science
While there are plenty of intervention opportunities discussed above, most work in this area is retrospective and conducted in high-income settings and might not represent multiple types of primary care settings globally. Much more robust data are needed from LMICs. Rigorous research is needed to establish the incidence and epidemiology of diagnostic error, to understand the role of contributory factors and to evaluate potential cognitive and/or system-related interventions.118 Evidence suggests that there is no single ‘magic bullet’ intervention for diagnostic error, and solutions need to be rigorously evaluated for benefits and unintended consequences.66 Moreover, we need research to define and evaluate the quality of diagnostic performance. Funding is required for all of this research.
The IOM recently also made several concrete recommendations to reduce diagnostic error, focusing on individual clinicians and also on patients, diagnostic services such as laboratory, pathology and radiology, and healthcare delivery systems.14 Many of these recommendations are applicable globally, such as better teamwork among all parties involved in diagnosis, adequate time and reimbursement for ‘cognitive’ work of PCPs, health IT that supports diagnosis, engaging patients, learning from errors and research funding climate conducive to accelerating our understanding of both problems and solutions. However, most will take sustained action and what is needed now are steps to outline a multifaceted approach that takes into account the local context where solutions are to be implemented.119 Based on the review, we suggest that the WHO consider bringing together primary care leaders, practicing frontline clinicians, safety experts, policymakers, health IT community, medical education and accreditation organisations, researchers from multiple disciplines, patient advocates and funding bodies among others, to address the many common challenges and opportunities to reduce diagnostic error.
Conclusions
Diagnostic errors are relatively frequent and harmful in primary care. While much remains to be learned, it is evident that errors involve diagnosis of common conditions. Diagnostic errors in primary care affect all countries, strategies to address them involve many stakeholders, and there is no other global agency addressing the problem. Thus, WHO's leadership and actions on a global level will be instrumental for prioritisation of practice changes needed to improve primary care as well as setting research priorities for intervention development to reduce diagnostic error.
References
Footnotes
Twitter Follow Hardeep Singh at @HardeepSinghMD
Funding Dr. Singh's research is supported by the VA Health Services Research and Development Service (CRE 12–033; Presidential Early Career Award for Scientists and Engineers USA 14–274), the VA National Center for Patient Safety, the Agency for Health Care Research and Quality (R01HS022087 and R21 HS 023602) and in part by the Houston VA HSR&D Center for Innovations in Quality, Effectiveness and Safety (CIN 13–413).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.