Article Text

Abstract
Background Patient participation in care is a fundamental element of safe and high-quality healthcare with the potential to enhance health outcomes and improve patient satisfaction.
Objectives To test the efficacy of a clinician-facilitated, bedside multimedia (MyStay) intervention designed to support patient participation in their recovery after total knee replacement surgery. The primary outcome was patients’ reported worst pain intensity on postoperative day 3. Secondary outcomes were patient activation, length of hospital stay, knee function and satisfaction with care.
Methods Unmasked, cluster randomised, four-period cross-over trial with a simultaneous process evaluation within in a large private, not-for-profit, metropolitan teaching hospital. Statistical analyses used linear mixed models with random effects for wards, cohorts within wards and patients within cohorts and fixed effects for treatment and period.
Results 241 patients were recruited between March 2014 and June 2015. Patients were admitted to intervention (104) or control (137) clusters. Intervention group patients reported significantly lower mean pain intensity scores on postoperative day 3 (6.1 vs 7.1, 95% CI −1.94 to −0.08, p=0.04). The percentages of patients who reported severe pain (score ≥7) were 43.7% and 64.2% in the intervention and control groups, respectively (χ2 9.89, p=0.002; generalised linear mixed model Wald test, p=0.05). Intervention group patients on average stayed in hospital one less day (5.3 vs 6.3, 95% CI 0.05 to 1.94, p=0.04), reported higher activation (45.1% vs 27.1% at level 4 activation) (p=0.04) and higher overall satisfaction with care (9.3 vs 8.6, 95% CI 1.09 to 0.219, p=0.01), and were more likely to refer family or friends to the health service (9.3 vs 8.7, 95% CI 1.07 to 0.13, p=0.02).
Conclusion The clinician-facilitated, MyStay bedside multimedia intervention enhanced patients’ activation and participation in their care after surgery; pain intensity and length of stay in hospital were reduced and patients were more satisfied with their care.
Trial registration ACTRN12614000340639 (http://www.anzctr.org.au/default.aspx).
- patient-centred care
- information technology
- health services research
- cluster trials
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Patient participation is recognised worldwide as a key element of quality healthcare.1–3 It is associated with positive outcomes for patients with chronic illness,4–6 but benefits of patient participation in acute care contexts remain less well described. In high acuity environments, barriers to participation include the brevity of interactions7 with multiple clinicians,8 9 patients’ symptom burden,9–11 acuity,9 11 perceived knowledge related to their condition,8 12 13 level of confidence14–16 and preference for participation.17–19 Yet overcoming these barriers will likely enhance recovery and patient experience overall.14 20
The early postoperative period after total knee replacement surgery (TKR) involves a complex balance between recovery, rehabilitation and prevention of complications. TKR is performed to treat end-stage arthritis when other treatment methods have not improved patient symptoms.21 Achieving maximum benefit from this surgery is dependent on correct insertion and fixation of the prosthesis, restoration of alignment of the knee22 and early mobilisation of the knee joint to maximise range of movement.23 24 Although a relatively common and successful procedure, TKR is considered one of the most painful,25 particularly in the early postoperative period.26 Patient participation in pain management, mobilisation and exercises may enhance recovery and prevent complications; however, activating patients to participate and work with the multidisciplinary team in order to benefit from the healthcare available to them16 27 is complex in acute environments. Simply equipping patients with information about ideal recovery without structured facilitation by clinicians is not sufficient.28 Innovative strategies are needed to assist patients to participate effectively in their care to the extent that is possible and preferred. Multimedia technology offers a potential platform for facilitating patient–clinician interactions because of its low burden, continuous availability and ease of use. There is evidence that multimedia plays an important role in preoperative delivery of information for patients undergoing surgery,29–31 but not for their postoperative recovery.
The study aimed to test whether the MyStay intervention, a clinician-facilitated multimedia programme designed to inform and assist patients to participate daily in their acute postoperative recovery, improved their recovery in terms of reduced pain intensity, reduced length of hospital stay, improved activation and function, and satisfaction with care received.
Methods
Trial design and participants
The Multimedia Intervention for Managing patient Experience (MIME) study was an unmasked, cluster randomised, four-period cross-over trial and simultaneous process evaluation conducted in three acute, inpatient orthopaedic wards of a large private, not-for-profit, metropolitan teaching hospital in Melbourne, Australia. Wards rather than patients were randomised to minimise ‘contamination’ through any exchange of information between patients. Because the intervention was clinician-facilitated and delivered on portable devices, blinding was not feasible. The duration of each period ranged from 12 to 16 weeks and was determined by the number of participants required in each cohort. Patient-level data were collected to measure outcomes (figure 1). For pragmatic reasons, namely to minimise the resources required to coordinate the study simultaneously over several sites, a cluster randomised cross-over trial, with ‘washout’ intervals between the periods and cohorts, was favoured in contrast to a cluster randomised trial run simultaneously at several sites or a stepped-wedge design. The cross-over design also allowed for adjustment, if required, for any trend in pain management over the life of the trial. The full trial protocol, including sample size calculation, has been published previously.32
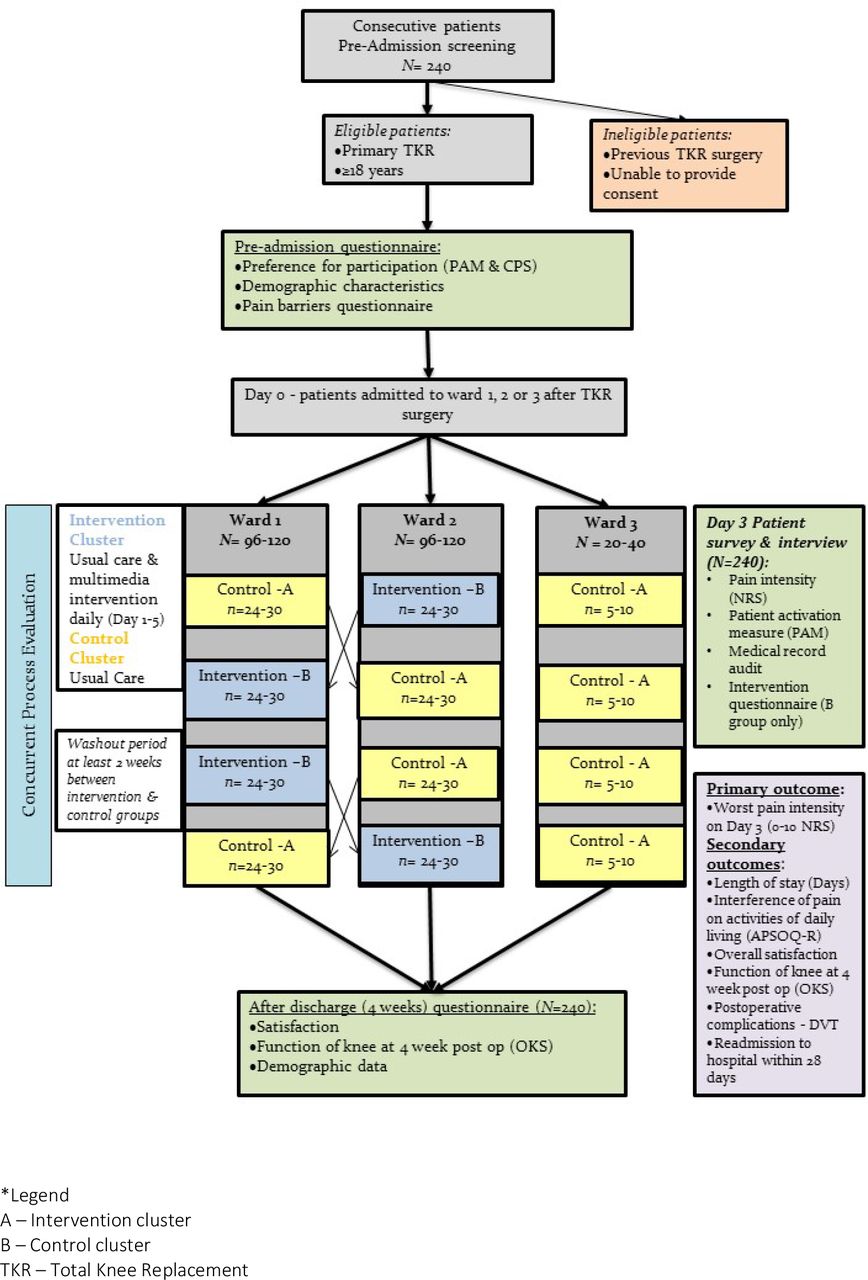
Study design. APSOQ-R, American Pain Society Patient Outcome Questionnaire—Revised; CPS, Control Preference Scale; DVT, deep vein thrombosis; NRS, Numerical Rating Scale; OKS, Oxford Knee Score.
Patients were included if they were adults (aged >18 years) and had an elective admission for primary, unilateral, TKR surgery and excluded if they were cognitively impaired or lacked proficiency in English language such that it would interfere with informed consent or ability to complete questionnaires. Most patients (79.6%) attended a standardised preoperative education session at the hospital 1 to 2 weeks prior to surgery and received information on how a TKR was performed, the possible risks and what to expect in the postoperative period.
Primary outcome
The primary outcome was patients’ reported worst (dynamic) pain intensity score measured using the 11-point Numerical Rating Scale33 (NRS) on day 3 after surgery (where day 0 refers to the day of surgery). Patients were asked to choose a whole number between 0 and 10 that best described their worst pain in the previous 24 hours where 0 equated to ‘no pain’ and 10 equated to ‘worst possible pain’. With two wards and 30 patients in each period within a ward, the trial was powered32 to detect a difference of 1.65 or more in mean pain intensity scores (a third ward was included to retain all consented patients).
A multimodal analgesic regime that included paracetamol, non-steroidal anti-inflammatory drugs (NSAIDs), long-acting opioids and short-acting opioids (for breakthrough pain) was recommended for all patients.
Secondary outcomes
Secondary outcomes were interference of pain on activities of daily living measured by items in the American Pain Society Patient Outcome Questionnaire—Revised (APSOQ-R)34 on day 3, length of hospital stay (days), function and pain following TKR surgery measured using the Oxford Knee Score (OKS)35 36 4 weeks after discharge from acute care, overall satisfaction and NET promoter score37 measured 4 weeks after discharge from acute care, incidence of deep vein thrombosis (DVT) within 28 days and incidence of readmission to study hospital within 28 days.
Concurrent process evaluation
Process evaluation was used to assess the conduct of the trial and explore whether the intervention had the intended effect of providing patients with the capability and opportunity to participate in care related to their goals of recovery. The overall objectives of the process evaluation were to determine if there were any differences in patient activation (Patient Activation Measure,38 PAM) between intervention and control group patients and, whether patient outcomes related to pain intensity may have been attributed to differences in available (prescribed) and/or administered analgesics between groups.
Randomisation
Two wards (clusters) were randomly assigned (by the trial statistician) to a sequence of control (A) and intervention (B) periods prior to recruitment of patients and commencement of the trial. A third ward, used as an ‘overflow ward’ for consented patients who could not be accommodated in the first two wards, received the control condition in each period. At the time of patient recruitment, it was not known to which cluster or period individual patients would be allocated. Allocation of patients to clusters occurred via usual hospital processes of ward allocation post-surgery and was largely dependent on bed availability at the time of surgery. Patient allocation to wards is undertaken centrally by a discrete hospital service and was in no way related to this research project or any persons involved or aware of this research.
Multimedia intervention
The bedside multimedia intervention known as ‘MyStay Total Knee Replacement’ (referred to as MyStay) was developed through consultation with patients, surgeons, physiotherapists and nurses and review of best available evidence and existing clinical pathways (detailed description of MyStay development—online supplementary material 1). MyStay was presented in a chapter-based format that combined text, sound, graphics and animation and packaged for iPad presentation. It was designed to be both clinician-facilitated and patient self-directed, that is, to be facilitated by clinicians during patient–clinician interactions but also used independently by patients as a stand-alone programme. MyStay had two interacting components: (1) information tailored to each day of recovery to enhance patients’ understanding of the goals of recovery and their role in their own recovery, and (2) opportunity for patients to achieve their recovery goals through clinician facilitation.
Supplemental material
It was expected that MyStay would facilitate interactions between patients and clinicians about daily goals and plans of care for each day of recovery and provide an opening for patients to discuss their pain management. Nurses in particular were asked to incorporate the intervention at the beginning-of-shift patient assessments by assisting their patients to navigate through the programme, clarify any uncertainties and plan their management together. Physiotherapists were asked to incorporate the exercise animations into physiotherapy sessions. Application of MyStay commenced on day 1 after TKR surgery.
Comparator
During control periods, throughout and following a wash-out period of 2 weeks, iPads containing MyStay were removed and patients received usual care based on the hospital standard care pathway (online supplementary material 2).
Supplemental material
Data collection
Data were collected at three time points: pre-admission, day 3 postoperatively and 4 weeks following discharge from acute care (table 1).
Measurements and tools used according to data collection periods
On day 3, all patients (intervention and control) completed a self-reported questionnaire and participated in a semistructured interview. Concurrent medication chart and medical record audits elicited the type and quantity of analgesics prescribed and administered in the previous 24 hours corresponding to the primary outcome measure of worst (dynamic) pain intensity.
Analgesics were prescribed either as fixed or pro re nata (PRN). Fixed analgesics were administered at set intervals and were not modifiable unless there was a contraindication to their administration; PRN analgesics were administered in response to ‘breakthrough’ pain (ie, pain that breaks through a fixed analgesic regimen) or in preparation for activities that may exacerbate pain such as physiotherapy or mobilisation.
According to the existing clinical care pathway in all wards, patients were deemed ‘eligible for discharge’ from acute care when assessed as medically stable, tolerating diet and fluids, walking independently, could safely ascend and descend stairs with the use of a walking aid, demonstrated confidence in attending home exercise programmes and were comfortable with a pain medication regime.
Follow-up questionnaires were administered 4 weeks after discharge via mail.
Statistical analyses
Quantitative data were analysed using GenStat (V.17) and analyses were independently validated using SPSS V.23. Statistical significance was claimed at p value <0.05. Descriptive statistics were used to characterise the study population and any differences between treatment groups and environmental characteristics. For the primary endpoint of pain intensity, a linear mixed model analysis, using the restricted maximum likelihood (REML) method,39 was used to calculate the F-test to enable comparison of the means of the groups (intervention vs usual care). The model included random effects for wards, cohorts within wards and patients within cohorts, and fixed effects for period and treatment (control vs intervention). If the period effect was not significant, it was deleted from the mixed model. Other outcome measures such as length of stay (LOS), pain and function following TKR, overall satisfaction, NET promoter, patient activation, incidence of DVTs and readmission to study hospital were compared between the groups and analyses used a linear mixed model approach and analogous methods developed for binary and categorical data. Analysis was according to intention to treat.
Results
Patient recruitment
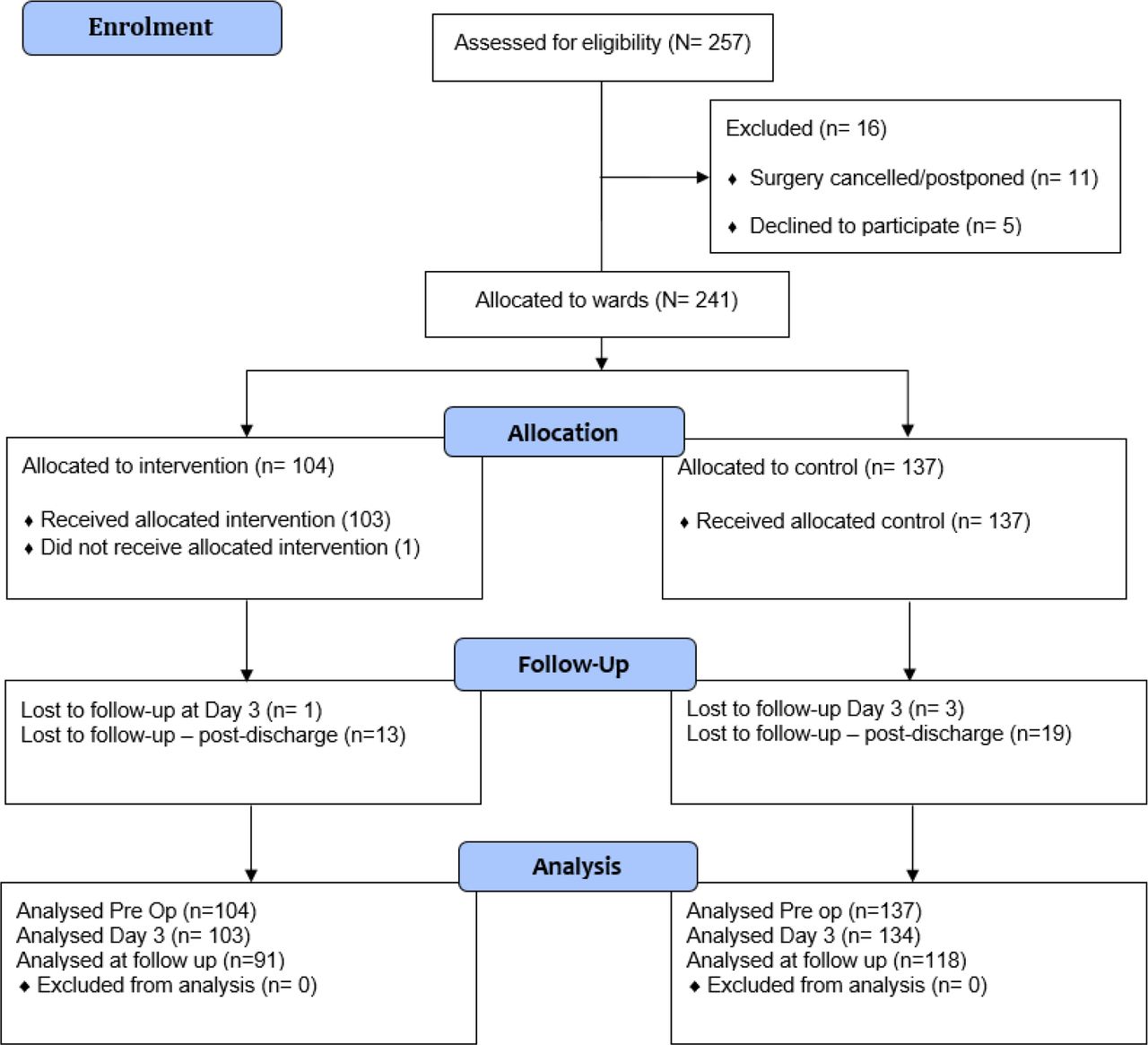
Between 12 March 2014 and 10 June 2015, of the 257 eligible patients, 241 were recruited (figure 2) either via the hospital pre-admission clinic (79.6%) or via mail-out invitations (20.4%). There was no significant difference in allocation to intervention or control cohorts for patients recruited via either method.
{kind=link}
{kind=link}
Trial profile.
Recruitment ended when the number of participants required for statistical power was reached. Follow-up data collection was completed in September 2015. Data validation and cleaning was conducted by the trial statistician, blinded to groups.
Loss to follow-up
Figure 2 outlines the flow of patients through the trial. One patient, allocated to an intervention period, did not receive the intervention because of a cerebrovascular accident in the early postoperative period. After discharge, 86.7% patients returned follow-up questionnaires.
Baseline data
The baseline characteristics of patients are presented in table 2. The mean age of participants was 65.3 (SD 9.8) years in the intervention group and 67.4 (SD 8.7) years in the control group (p=0.20). There were slightly more women (55.2%) than men (44.8%) in the sample overall, and the proportion of men was lower in the intervention group (38.5%) than the control group (49.6%), but this difference was not significant (p=0.09). Key demographic characteristics were balanced between study periods.
Baseline characteristics of the intention-to-treat population
Baseline assessments
The Pain Barriers Questionnaire (BQ)40 and PAM41 were completed prior to admission by all patients. There were no significant differences in the mean scores for the BQ between groups (intervention group M=16.1 vs control group M=15.6, t=0.71, p=0.48). Pre-admission, patients in both groups were found to have a high level of activation (levels 3 and 4) according to the PAM, indicating an understanding of their role in maintaining their health and perceived capability to fulfil that role (intervention group 79% vs control group 74%, p=0.09).
Primary outcome
The mean worst pain scores, measured on day 3 using the NRS, were 6.05 (SEM 0.33) (intervention group) and 7.05 (SEM 0.28) (control group) (mean difference (I-C)=−1.01, 95% CI −1.94 to −0.08, p=0.04). The period effect was not significant (p=0.61) and the estimated components of variance were 0.05, 0.14 and 5.56 for wards, cohorts within wards and patients within cohorts, respectively. The percentages of patients with severe pain (score≥7) were 43.7% intervention group versus 64.2% control group (p=0.002; generalised linear mixed model Wald test, p=0.049). In an unplanned, supplementary analysis that excluded all 41 patients in the overflow ward, the mean worst pain scores were 6.03 (SEM 0.38) (intervention group) and 6.96 (SEM 0.39) (control group) (mean difference 95% CI –2.13 to 0.27, p=0.10).
In an additional unplanned analysis adjusted for administered PRN oxycodone (Endone), inclusion of the oxycodone covariate in the REML analysis was almost statistically significant (p=0.05) and a 1 mg increase in dose was associated with a 0.03 increase in day-3 reported pain (NRS). The difference in the adjusted means of the treatment arms remained significant: mean difference (95% CI −2.06 to −0.25, p=0.02). There was no evidence of an interaction between the oxycodone covariate and the treatment (p=0.41).
Secondary outcomes
Secondary outcome analyses (APSOQ-R) are presented in online supplementary material 3. Patients in the intervention group perceived that they had received more pain relief in the previous 24 hours (M=7.67 vs M=7.07, 95% CI −0.003 to 1.194, p=0.05). Significantly more patients in the intervention group than the control group reported using deep breathing as a method to relieve pain (82.2% vs 68%, χ2=5.53, p=0.02).
Supplemental material
There was a significant reduction in LOS for the intervention group; intervention group 5.29 days vs control group 6.29 days (95% CI −0.05 to −1.94, p=0.04). One patient in the intervention group was discharged prior to day 3; this patient was sent to in-hospital rehabilitation on day 2 following surgery. None of the control group patients were discharged from acute care prior to day 3.
There was no difference between groups in terms of those discharged directly home compared with a rehabilitation facility. Most patients (86.3%) were discharged to in-patient rehabilitation. In addition, there was no difference between patients discharged home versus rehabilitation in terms of acute care length of stay.
Patient activation
There was no significant difference in activation between groups when measured at baseline (χ2=6.41, p=0.09). On day 3, a significantly higher proportion of patients in the intervention group reported level 4 activation (45.1% vs 27.1%, χ2=8.47, p=0.04). The number of control group patients with activation scores at level 3 or 4 reduced from 74% at baseline to 53% on day 3. Activation in the intervention group patients also declined but not to the same degree; from 79% patients at level 3 or 4 at baseline to 64% on day 3.
Four weeks after discharge from acute care, patients’ activation levels returned to those at pre-admission. For the intervention group, 82% indicated level 3 or 4 activation versus 74% control group patients on follow-up. There was no significant difference between groups in patient activation measured at follow-up (p=0.56).
Analgesic management
In relation to processes of care, the prescription and administration of both fixed and PRN analgesics for the 24 hours preceding the day 3 pain score were extracted from all patients’ charts. There was no significant difference between groups in terms of prescribed regular and PRN analgesics. Tables 3 and 4 outline prescribed and administered fixed and PRN analgesics by treatment group, respectively. There were no differences in prescriptions for paracetamol, NSAIDs, adjuvant medicines or opioids between groups. Overall, 5.8% of patients indicated an allergy to NSAIDs and were excluded from these analyses.
Prescribed fixed and PRN analgesics by group
Administered fixed and PRN analgesics by group
The most commonly prescribed and administered PRN strong opioid was oxycodone (Endone) with most patients (96.3%) receiving at least one dose during the 24-hour audit period (table 4). Endone was administered as an oral tablet and the total administered dose over 24 hours ranged from 2.5 to 30 mg. There was a difference between treatment groups in the mean daily amount (mg) of oxycodone administered PRN (intervention group M=16.1 vs control group 10.8, t=3.23, p=0.001) (table 4). While the interaction between treatment groups and subgroups of patients categorised by pain score (0–3, 4–6 and 7–10) was not significant (p=0.29), there was a trend (p=0.002) for oxycodone administered PRN to increase across the pain groups and a significant difference between the treatments was noticed in the highest (7–10) pain group: intervention (M=21.2, SD=13.5 mg) and control (M=11.9, SD=12.9 mg) groups (p=0.004).
Patient follow-up
Intervention group patients had a mean OKS of 19.9 and control group patients 21.3 four weeks post-surgery; this difference was not significant (95% CI −5.78 to 2.80, p=0.44).
Intervention group patients reported higher mean satisfaction with care received of 9.26 versus 8.58 control group patients (95% CI 1.09 to 0.219, p=0.01). Intervention group patients were also more likely to ‘recommend the health service to a family or friend’ (NET promoter score) with a mean score of 9.27 versus 8.67 (95% CI 0.13 to 1.07, p=0.02). The intervention group also had a higher percentage of promoters (81.3%) compared with the control group (66.9%) (χ2[2, N=209]=8.80, p=0.01).
Eight (3.3%) patients developed a DVT while inpatients or presented to the study hospital within 28 days of discharge. Of these, six patients were in the intervention group and two were in the control group (p=0.06). Six (2.5%) patients were readmitted to hospital within 28 days of discharge from hospital for any reason; three in the intervention and three in the control group (p=0.73).
Discussion
Our results show that the MyStay intervention, designed to enhance patient participation, was effective in reducing patients’ reported pain intensity on day 3 after TKR surgery when compared with standard care. Although patients in both groups reported high levels of dynamic pain on day 3 following surgery (suggesting that pain management overall was suboptimal),42 intervention group patients reported lower worst pain scores indicating that they experienced lower levels of dynamic pain. Patients who received the intervention also had a lower length of stay in acute care, higher overall satisfaction with the care they had received, and were more likely to recommend the health service for similar surgery to family and friends. There were no observed differences in interference of pain on activities of daily living (APSOQ-R), knee pain and functioning (OKS) 4 weeks after discharge, incidence of DVTs or readmission to the study hospital.
The clinical significance of these results is the evidence of the impact of patient participation on patient-reported and organisational outcomes in acute care environments. Prior to this study, interventions designed to facilitate patient participation in acute care had failed to show effects other than higher patient satisfaction.43–46
While the significant reduction (1.01) in mean pain scores may seem small, it corresponds to a ‘medium’ effect size (Cohen’s d) of 0.42 and it is approximately one-third of the IQR of the observed scores and is therefore of clinical relevance. Furthermore, whereas 64% of control patients had a day-3 score ≥7, with MyStay 44% of patients had a day-3 score ≥7. In some patient populations, ‘7’ is regarded as the cut-off for severe pain47 so the MyStay intervention produced a non-trivial reduction in the percentage of patients experiencing severe pain. Patients in the intervention group received significantly higher amounts of PRN oxycodone. While that may explain the lower reported worse pain intensity scores, unplanned post hoc analyses failed to show a significant interaction between PRN oxycodone dose and treatment group. Patients receiving MyStay were also more likely to use non-pharmacological methods to manage pain. We need a better understanding of the ways in which patient participation affects pain experience and patients’ influence on the care they receive. We can conclude, however, that the MyStay intervention as a treatment policy has a clinically important effect on the occurrence of severe pain.
Reasons for differences in acute LOS can be multidimensional and may depend on the age and demographic characteristics of the patient population, readiness of the patient for discharge and the availability of beds in rehabilitation facilities.48 The observed reduction in LOS may not be reproducible in the future where the LOS in acute care is continually decreasing through enhanced recovery pathways.49 50 Although enhanced recovery pathways are commonly used internationally, they are not widely used in Australia to date.51 52 On average, data from 2016 to 2017 indicate that patients following TKR in Australia spend 4.7 days (range, 3.6–8.3 days) in hospital.53 There were no changes to the Care Pathways or TKR practice by the surgeons during the study period. The reduction in hospital LOS observed in this study suggests that a relatively low-cost, clinician-facilitated MyStay multimedia intervention at the bedside that provided patients with the necessary information and the opportunity to engage with clinicians increased patients’ engagement in mobility and exercise to maximise function and knee flexion, and hence ‘readiness for discharge’. The findings provide ‘proof of concept’ that patient participation can improve outcomes other than patient satisfaction alone and the benefits of patient participation may extend to rehabilitation or home if patients are discharged early.
Further evidence suggesting that MyStay was effective in engaging patients in their recovery were findings relating to the activation scores and satisfaction with care. Prior to admission, the majority of patients had relatively high activation scores indicating that they felt they had the necessary skills and knowledge to care for themselves. There was no difference between intervention (79% at level 3 or 4) and control groups (74% at level 3 or 4) prior to admission to hospital. On day 3 after surgery, although there was a reduction in the proportion of patients at level 3 and 4 activation in both groups, this reduction was most marked in control group patients. There was a 20% decrease in the number of control group patients with level 3 or 4 activation compared with baseline, and the difference between intervention and control group patients at this level was significant. Patient activation measures returned to baseline measures for both groups 4 weeks after surgery. These findings highlight the impact of acute illness and acute care environments on patients’ perceived ability to manage their healthcare needs and the need for, and potential effectiveness of, interventions to moderate these impacts.
Patients exposed to the intervention had a significantly higher overall satisfaction with their acute care experience and a higher NET promoter score. Although there are well-known limitations in the measurement of patient satisfaction,25–27 the consistency of higher satisfaction with other patient-reported outcomes such as the NET promoter score37 and lower reported pain intensity supports an interpretation of an intervention effect on satisfaction.
Failure to obtain an OKS preoperatively meant that we could not evaluate differences in changes in knee function at follow-up. Further limitations may include the lack of blinding of the intervention among ward nurses, patients and data collectors and could have introduced bias. Blinding in this type of intervention was not possible because the iPads were visible and patients would often refer to the MyStay. To mitigate the risk of bias, validated outcome questionnaires were used. Data collectors extracting medical record audit data and the statistician who conducted the analysis were blinded to group. A robust research methodology was used to overcome the limitations associated with conducting a single-site study54; however, the generalisability of our findings to other health service settings needs further investigation. The inclusion in the analyses of data gathered from consented patients allocated to the overflow ward, which itself received a fixed sequence consisting of the control condition in all four periods, could be criticised for being susceptible to an unknown allocation bias; however, in a supplementary analysis of the primary endpoint, which excluded these patients, the observed effect was similar in magnitude, but given the 17% reduction in the total sample size, it was no longer statistically significant at the conventional 5% level.
Creating an opportunity for patient participation without placing additional burden on clinicians and patients in this context was considered critical because implementing a shared tool has the risk of adding to the burden of care rather than facilitating it. Time spent orientating patients to the technology was approximately 5 to 10 min initially (day 1), then 2 to 5 min per day with individual patients. It is concluded, therefore, that the MyStay intervention can be incorporated into everyday routine care despite the acuity of the environment, and the time required for clinicians to apply (not facilitate) the programme is low and feasible. The MyStay programme provides patients with an alternative and complementary source of information related to their recovery that is usually highly reliant on clinicians and often limited to ‘what is important now’ rather than what the patient wants or needs to know.
Our findings contribute to the evolving understanding of the role of patient participation in acute care environments and the use of multimedia technology as a tool for facilitating patient–clinician interactions. We have shown that a simple and easily implementable intervention such as MyStay facilitated patient participation in their care after surgery and improved outcomes. These findings would be strengthened by replication in other acute healthcare settings; however, our findings support the use of facilitated patient engagement interventions in postoperative recovery after TKR.
Acknowledgments
The authors acknowledge and thank the associate editors and reviewers for their helpful comments.
References
Footnotes
Contributors JM, RdS, BR, AFH, PML, JR and MB conceived the study and designed the trial. MB supervised the conduct of the trial and data collection. JM collected, analysed the data and drafted the manuscript. JR was responsible for secondary analysis of the data. All authors contributed substantially to manuscript revision. JM completed the final draft, submitted the manuscript and takes responsibility for the paper as a whole.
Funding The Norman Beischer Medical Research Foundation provided funding for the MyStay development.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval Approval to conduct this research was received from the University Human Research and Ethics Committee (approval no. 2013-195) and the hospital where the data were collected (approval no. 598-13).
Provenance and peer review Not commissioned; externally peer reviewed.