Article Text

Abstract
Background Benzodiazepines and sedative hypnotics (BSH) have numerous adverse effects that can lead to negative outcomes, particularly in vulnerable hospitalised older adults. At our institution, over 15% of hospitalised older adults are prescribed sedative-hypnotics inappropriately. Of these prescriptions, 87% occurred at night to treat insomnia and almost 20% came from standard admission order sets.
Methods We conducted a time-series study from January 2015 to August 2016 among medical and cardiology inpatients following the implementation in August 2015 of a sedative reduction bundle (education, removal of BSH from available admission order sets and non-pharmacological strategies to improve sleep). Preintervention period was January–July 2015 and postintervention period was August 2015–August 2016. A surgical ward served as control. Primary outcome was the proportion of BSH-naive (not on BSH prior to admission) patients 65 years or older discharged from medical and cardiology wards who were prescribed any new BSH for sleep in hospital. Data were analysed on statistical process control (SPC) p-charts with upper and lower limits set at 3δ using standard rules. Secondary measures included Patient-reported Median Sleep Quality scores and rates of fall and sedating drug prescriptions that may be used for sleep (dimenhydrinate).
Results During the study period, there were 5805 and 1115 discharges from the intervention and control units, respectively. From the mean baseline BSH prescription rate of 15.8%, the postintervention period saw an absolute reduction of 8.0% (95% CI 5.6% to 10.3%; p<0.001). Adjusted for temporal trends, the intervention produced a 5.3% absolute reduction in the proportion of patients newly prescribed BSH (95% CI 5.6% to 10.3%; p=0.002). BSH prescription rates remained stable on the control ward. Patient-reported measure of sleep quality, falls and use of other sedating medications remained unchanged throughout the study duration.
Conclusion A comprehensive intervention bundle was associated with a reduction in inappropriate BSH prescriptions among older inpatients.
- quality improvement
- medication safety
- hospital medicine
Statistics from Altmetric.com
Introduction
Problem description
Benzodiazepine sedative-hypnotics (BSH) are high-risk drugs associated with numerous adverse effects, including daytime sedation, ataxia, delirium, anterograde amnesia and cognitive impairment.1–4 They are often started during an acute care hospitalisation and continued following discharge.5–7 In a long-term population-based cohort study of older adults in Ontario, Canada, who were discharged after an acute care hospitalisation, 3.1% of patients were on newly prescribed benzodiazepines within 1 week of their hospital discharge and 1.5% of the study cohort went on to become chronic benzodiazepine users.6 A Swiss observational study also highlighted the issue of new BSH exposure during hospitalisation which was associated with subsequent ambulatory BSH prescribing.8 The authors identified that BSH were newly prescribed for 37% of patients hospitalised in a general internal medicine ward. At discharge, the proportion of patients who received a BSH had increased by 10%. In-hospital BSH prescriptions may increase the long-term use of BSH and expose patients to drug-related problems.
Available knowledge
Hospital-acquired insomnia is a common reason for BSH initiation. Inpatients commonly experience sleep disturbances due to acute illness, pain, anxiety, a change in living environment or external night-time interruptions such as frequent clinical monitoring, excessive lighting, activity and noise.2 3 Studies demonstrate BSH can improve sleep latency and sleep time and decrease night time awakenings; however, the effect size is small.9 In contrast, there is an overwhelming risk of adverse events, including delirium, falls, hip fractures, motor vehicle accidents, physical dependence and cognitive impairment.10–13 The number needed to treat for BSH to achieve a small incremental improvement in sleep is 13, whereas the number needed to harm is six.9
Successful interventions aimed at reducing BSH use include implementation of non-pharmacological sleep protocols to provide a safe alternative to promoting sleep in hospitalised older patients.14 15 Examples include relaxation techniques and interventions aimed at improving the sleep environment (eg, reducing interruptions and bright light exposure).
Rationale
We previously published a retrospective observational study conducted at Mount Sinai Hospital (MSH) that found 15.9% of the older patient cohort who were BSH naive (patients not prescribed BSH prior to hospital admission) were newly prescribed a BSH during their hospitalisation. The majority of the BSH orders were used as needed for insomnia. The contributing factors to new BSH initiation were the presence of BSH on an admission order set, junior level physician trainees and patient-reported poor sleep quality in hospital.16 These findings helped us define the problem of prevalent inappropriate BSH use and its root causes. This work led to the development of a quality improvement (QI) project to reduce exposing older patients to unnecessary harm from BSH and informed the basis of our theory of change.
Specific aim
We aimed to reduce the proportion of BSH-naive inpatients on medicine and cardiology wards who were prescribed a new BSH in hospital for sleep by 20% in 1 year.
Methods
Context
MSH is a 443-bed academic hospital affiliated with the University of Toronto and is home to over 2400 medical learners annually. Rotations on general internal medicine (GIM) and cardiology serve as clinical teaching units for medical students and residents. There are 84 patient beds designated to GIM and 14 to cardiology services. The majority of patients under the care of GIM are located on three wards, with one ward shared with cardiology.
These contextual factors helped to generate a number of change ideas which we tested by completing five plan, do, study, act (PDSA) cycles across the study period. We selected the GIM and cardiology wards to implement our QI initiative based on the education opportunities for those involved. A surgical ward served as our control unit, as these clinicians, trainees and patients were cohorted to the control ward and not exposed to the intervention.
Intervention
We formed a multidisciplinary QI team consisting of a physician champion, nurses, pharmacists, trainees and unit administrators. The team aligned the project with the hospital priority of fall reduction and was endorsed by the Falls Prevention Steering Committee. Through root cause analyses, we identified several strategies and utilised them based on a balance of their effectiveness and feasibility of implementation. Removal of BSH from the electronic admission order sets was our system-focused approach to simplify and standardise care of GIM and cardiology patients. The BSH options were removed from the admission order sets where they appeared as ‘routine’ orders and these were only available on the cardiology order sets. Routine BSH orders were not options in the GIM admission order sets. We also leveraged team-based pharmacists to remind prescribers to avoid BSH use for sleep.
Although interventions aimed at human behaviour are usually rated as less effective compared with forced functions and system-focused interventions, there is value in person-focused interventions. In our experience, interventions that fail to engage staff or provide an educational basis for change can produce workarounds or unsustainable results. Because healthcare providers are still needed to make judgments throughout a patient’s care journey, we anticipated curtailing BSH orders at admission would not be sufficient as they can still be ordered ad hoc. The educational aspect of the intervention (through case-based vignettes and engagement of front-line staff and patients/families) served to also engage staff on non-pharmacological sleep approach which required their buy-in. While not effective as a sole intervention, educational strategies can complement multifactorial interventions that have scientific basis in targeting different problem contributors (such as the belief that zopiclone is safer than benzodiazepines). Finally, front-line staff implemented non-pharmacological sleep hygiene including reducing daytime napping, disruptions (eg, medication administration, vital sign monitoring) and noise and offering ear plugs or eye masks.
Study of the interventions
The interventions were trialled and refined through iterative PDSA cycles. The QI implementation team met monthly during the baseline data collection phase. Follow-up meetings occurred every 2–3 months during the cycles to monitor and refine the interventions.
Measures
The primary outcome was the proportion of BSH-naive patients 65 years or older discharged from medical and cardiology wards that were prescribed any new BSH for sleep. We collected data from January 2015 to August 2016, using a similar methodology to our prior prevalence study.16 Preintervention period was from 1 January 2015 to 31 July 2015 and the postintervention period was from 1 August 2015 to 31 August 2016. The primary outcome on the control ward was available from 1 January 2015 to 31 July 2016. The control ward was a medical–surgical ward and included all patients admitted to the unit. The largest admitting services were gastroenterology (ie, inflammatory bowel disease service) and general surgery. Target BSH included all benzodiazepines, trazodone, quetiapine and zopiclone, the only available z-drug on formulary at the time of the study. The pharmacy’s electronic prescription database and the electronic patient medical records provided the outcome measure. An unblinded study team member performed comprehensive chart reviews to determine the indication of BSH prescriptions. Inappropriate BSH prescriptions among this naive population included: (1) any orders for zopiclone; (2) any night-time orders (between 20:00 and 06:00) and (3) indication of ‘sleep’ or ‘insomnia’ identified in the indication field for as-needed medications through chart review of electronic prescription orders. A second research assistant independently verified the data with 100% agreement.
Process outcomes collected on the intervention wards consisted of the proportion of clinical care providers who received the educational intervention to reduce BSH prescribing and proportion of patients and/or their caregivers receiving educational material.
We measured self-reported sleep quality through patient and caregiver surveys as a balancing measure as well as a patient-reported experience measure (PREM). Patients quantified their in-hospital sleep quality using a Likert scale (score 1=very poor and 5=excellent). We administered PREMs at two time points: prior to intervention bundle implementation and 2 months postintervention. As balancing measures, we included aggregate fall rates and rates of other sedating drugs that may be used for sleep such as dimenhydrinate. Falls are corporately collected using hospital administrative data and included injurious falls. Data is validated by the Performance Measurement Office using chart review. Rates of balancing drugs were determined as follows: patients discharged from study wards by month with ANY prescriptions of balancing drugs divided by total number of patients discharged from the study wards.
Analysis
Descriptive analyses were used to summarise demographic results. Continuous variables were compared using two-tailed t-test and categorical variables using χ2 test. Median hospital length of stay and sleep quality scores were compared using Mann-Whitney test. We used SPC charts to compare the baseline period (January 2015–July 2015) and the intervention period (August 2015–August 2016) for the primary outcome and balancing measures. SPC charts were analysed using standard rules to detect any signal of special cause variation in the charted data points.17 The unadjusted difference in proportions for the preintervention and postintervention periods was computed using the Wilson method. Generalised linear models (binomial likelihood with identity link function) were used to estimate an adjusted intervention effect. The Akaike Information Criterion (AIC) was used to select from several prespecified candidate models, allowing for both additive and interaction effects among group (treatment vs control wards), intervention period (effecting the treatment ward only, or as a shared effect) and time (as biweekly period); for each model, we compute the Box-Pierce Test p-value by ward to assess for correlation residuals (online supplementary file 1). For the lowest AIC model, we report parameter estimates, 95% CIs and Wald p-values. We use alpha=0.05 as the threshold for statistical significance. The primary reason for using an identity link was the desire to assess and report a linear time trend on the probability (percent) scale for ease of interpretability. The analysis was performed using R V.3.4.4. (Free Software Foundation, Boston, Massachusetts, USA). SPC charts were created using QI Macros SPC software for Excel V. 2012.07 (KnowWare International, Denver, Colorado, USA).
Supplemental material
This study follows the SQUIRE V.2.0 publication guidelines for reporting.18
Results
Between January 2015 and August 2016, 5805 patients were discharged from the intervention units. Of these, 82.3% were under the GIM service and 52.2% were female. The mean age was 67 (SD 19.9) years and median length of stay was 5.0 (IQR 3.0–8.0) days. Intervention and control group demographics are displayed in table 1.
Characteristics of patients discharged from study wards
PDSA cycle #1
In August 2015, one of the QI physician team members provided medical students and residents with clinical teaching sessions about the hazards of using BSH as sleep aids and discussed alternative strategies to use when paged overnight (such as non-pharmacological sleep hygiene), during GIM monthly teaching rounds. More than 70% of learners attended at least one of the three sessions (education, data review and feedback) held during the rotation. In addition, we provided emailed performance feedback in the form of a run chart of the primary outcome to all trainees 2 weeks after the education sessions which allowed for reflection on prescribing patterns. Following the initial education, ongoing emails and reminders from the chief resident occurred at the start and mid-way through each 4-week rotation.
PDSA cycle #2
Because our previous BSH prevalence study identified over 20% of BSH prescriptions originated from cardiology admission order sets, we removed BSH options (diagnoses specific and postprocedural order sets) in consultation with the cardiology division.3 The order set change requests were approved by the relevant hospital committees and implemented in November 2015.
PDSA cycle #3
Pharmacists conducted structured medication reviews and alerted physicians when new BSH were ordered for a BSH-naive inpatient on their team. This provided just-in-time teachable moments for trainees. Pharmacists worked with nurses on their wards to minimise interruptions to patients’ sleep at night through rescheduling medication administration times to outside the hours of 22:00–06:00, when possible.
PDSA cycle #4
We conducted patient interviews to monitor sleep quality in hospital as a balancing measure. During this patient engagement process, we identified barriers to sleeping in hospital that included disruptions and noise. This information served as feedback to front-line staff and resulted in the implementation of published non-pharmacological sleep protocols to address the main contributor of disruptive sleep in hospital.17 19 This included dimmed hallway lighting between 22:00 and 06:00, noise minimisation in nursing stations, television volumes reduced and offering of ear plugs to patients. Minimising interruptions to sleep included avoidance of waking patients for routine vital signs and blood sampling during sleep hours and identification of medications that could be reassessed for rescheduling.
Strong nurse leadership and organisational support helped to enable a culture change to promote sleep and minimise interruptions. A physician champion delivered sleep hygiene in-service education on intervention wards and targeted all nurses during day and night shifts. Advanced nurse practitioners engaged their colleagues in regular staff huddles, with emphasis on promoting sleep hygiene and reducing unnecessary BSH requests. Unit-based sleep hygiene rollout occurred in April–May 2016.
PDSA cycle #5
We implemented an educational sleep hygiene campaign aimed at patients and caregivers. Volunteers provided patients with handouts containing tips to sleep better in hospital without pharmaceutical aids (such as ear plugs which we made available on the wards, eye masks and sound/light reductions). Posters and educational materials aimed at empowering patients and caregivers to advocate for sleep hygiene practices were placed in visible patient care areas. These infographics contained descriptions of non-pharmacological strategies to improve sleep and descriptions of associated harms of sedatives (such as falls, hip fracture and confusion).
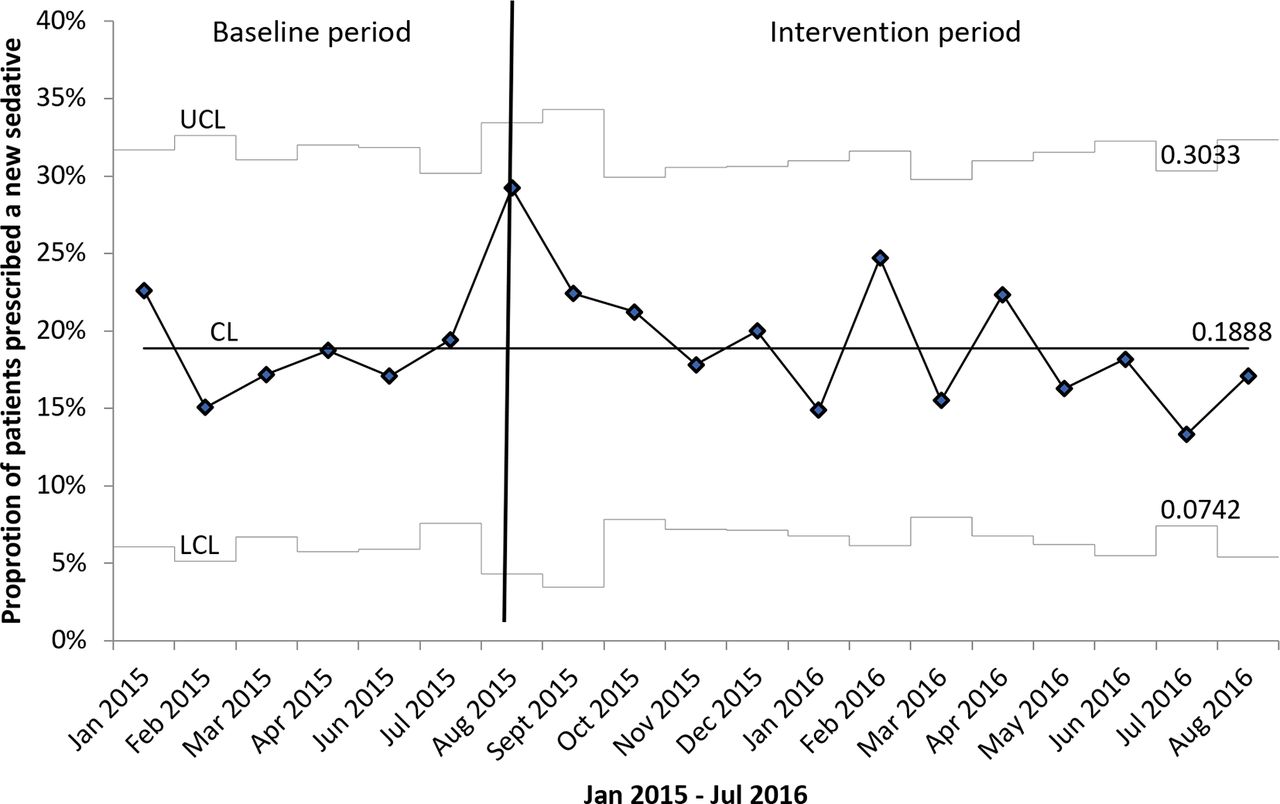
The figure 1 uses the Institute for Safe Medication Practices framework and summarises the intervention components in order from systems-oriented (top of pyramid) to person-oriented (bottom of pyramid) interventions to address all the contributing factors to potential BSH overuse.20 Unadjusted mean BSH prescription rate during baseline is 15.8% with an absolute reduction in the postintervention period of 8.0% (95% CI 5.6% to 10.3%; p<0.001). Prior to the intervention phase, there was a small declining trend of 0.1% per 2 weeks. The estimated intervention effect, adjusted for temporal trend, is a 5.3% absolute reduction in the proportion of new sedatives (95% CI 2.0% to 8.6%; p=0.002) (online supplementary file 1). The figure 2 demonstrates a shift pattern after the intervention was implemented, with a sustained reduction in the proportion of inappropriate BSH prescriptions. Improvement in the primary outcome was stable with 11 months of postintervention data. The mean outcome measure on the control ward was 20.2% and 18.3% in the preintervention and postintervention periods, respectively, with a stable process (figure 3).

Hierarchy of effective interventions* to reduce new benzodiazepine and sedative-hypnotic use for insomnia in naive older inpatients.

Proportion of new benzodiazepine and sedative-hypnotic prescriptions in naive older inpatients on intervention units by discharge date. PDSA, plan, do, study, act.

Proportion of discharged patients prescribed new benzodiazepine and sedative-hypnotics in control unit by discharge month.
More than 80% of nursing staff and physicians attended educational sessions and/or received materials. Educational materials were reviewed with patients and/or caregivers at regular intervals. Preintervention and postintervention patients reported similar hospital sleep quality (median score 3 (IQR 1.5–4.5) vs 2 (IQR 0–4.0), respectively, p=0.21).
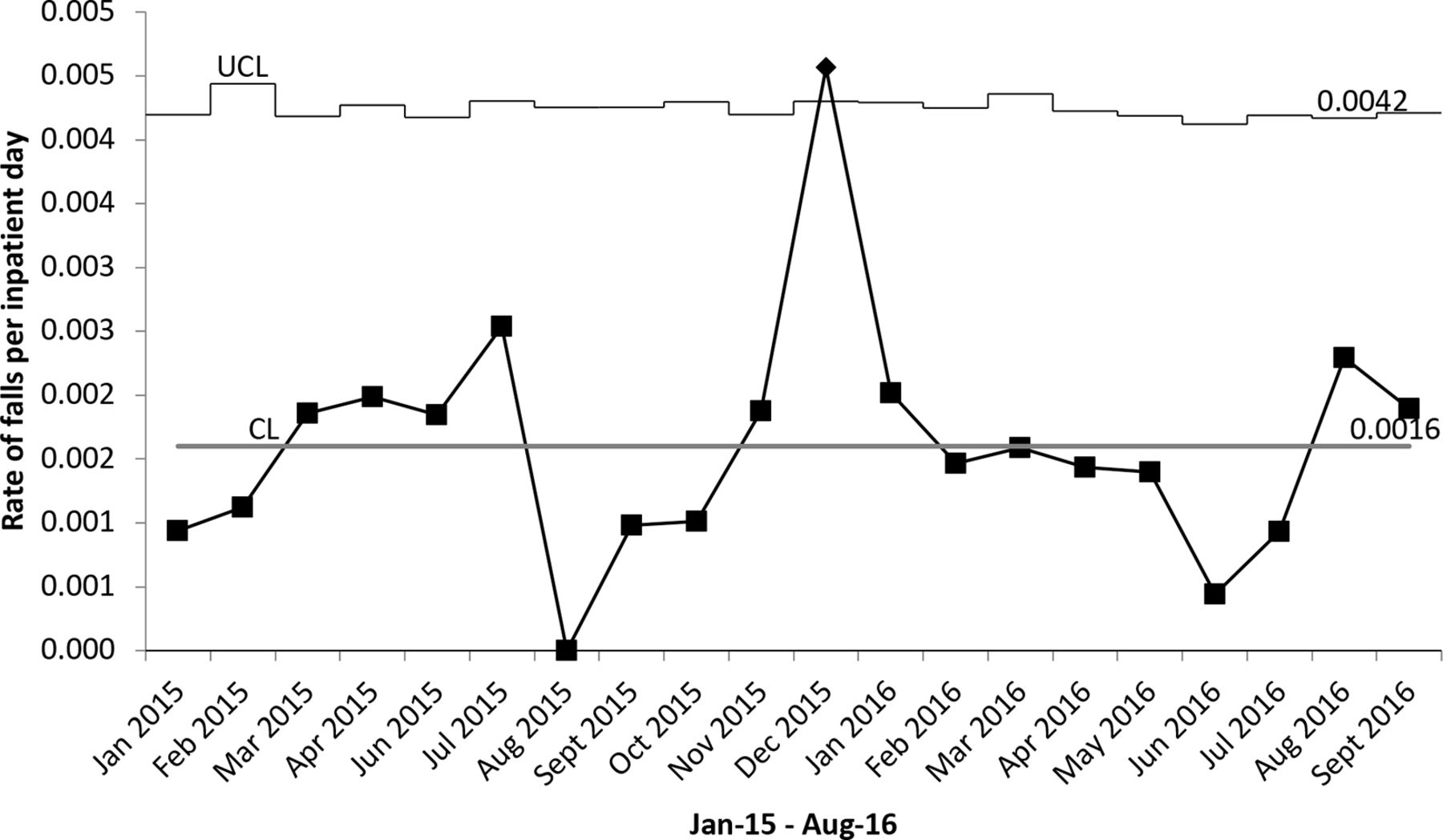
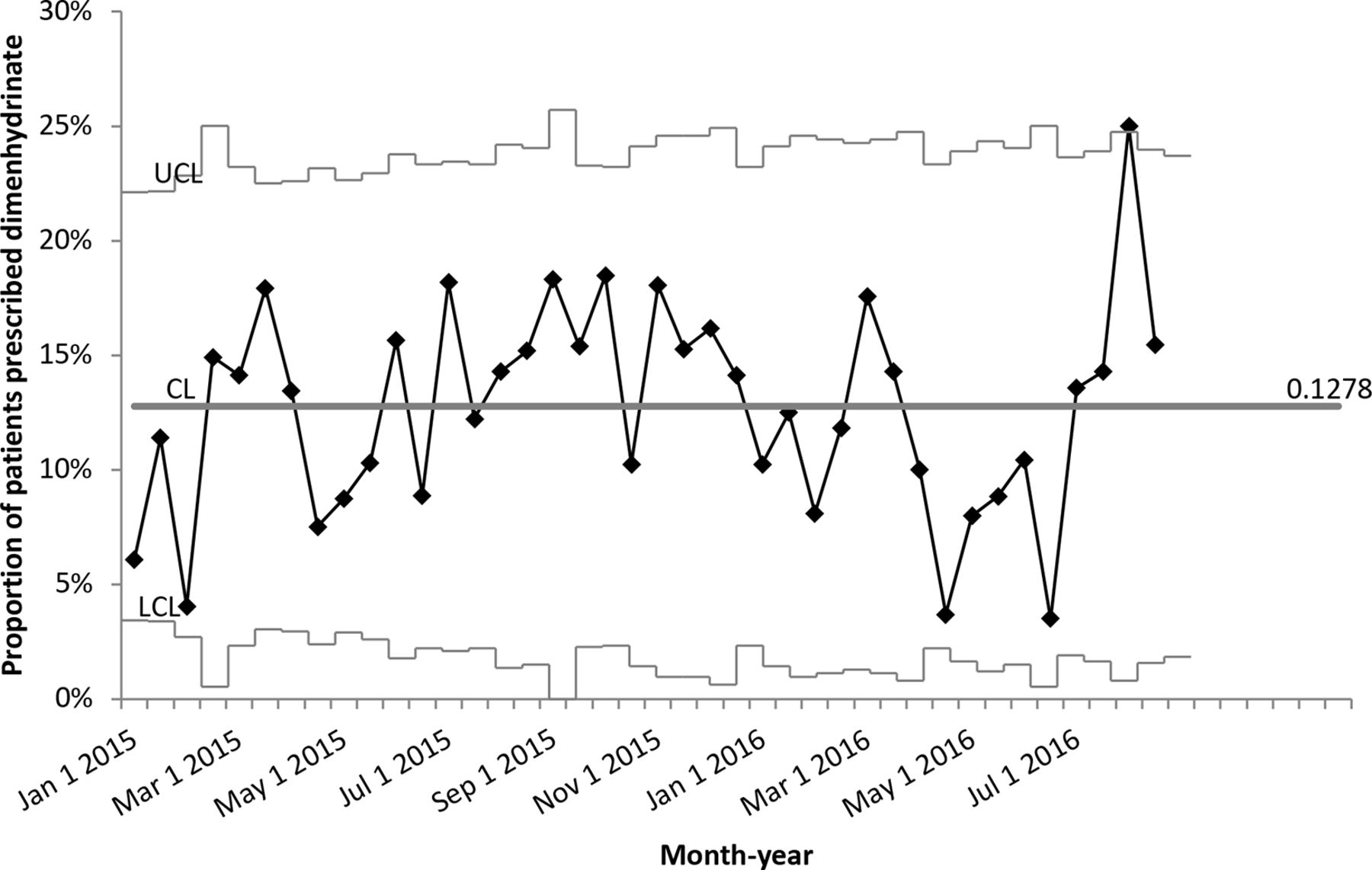
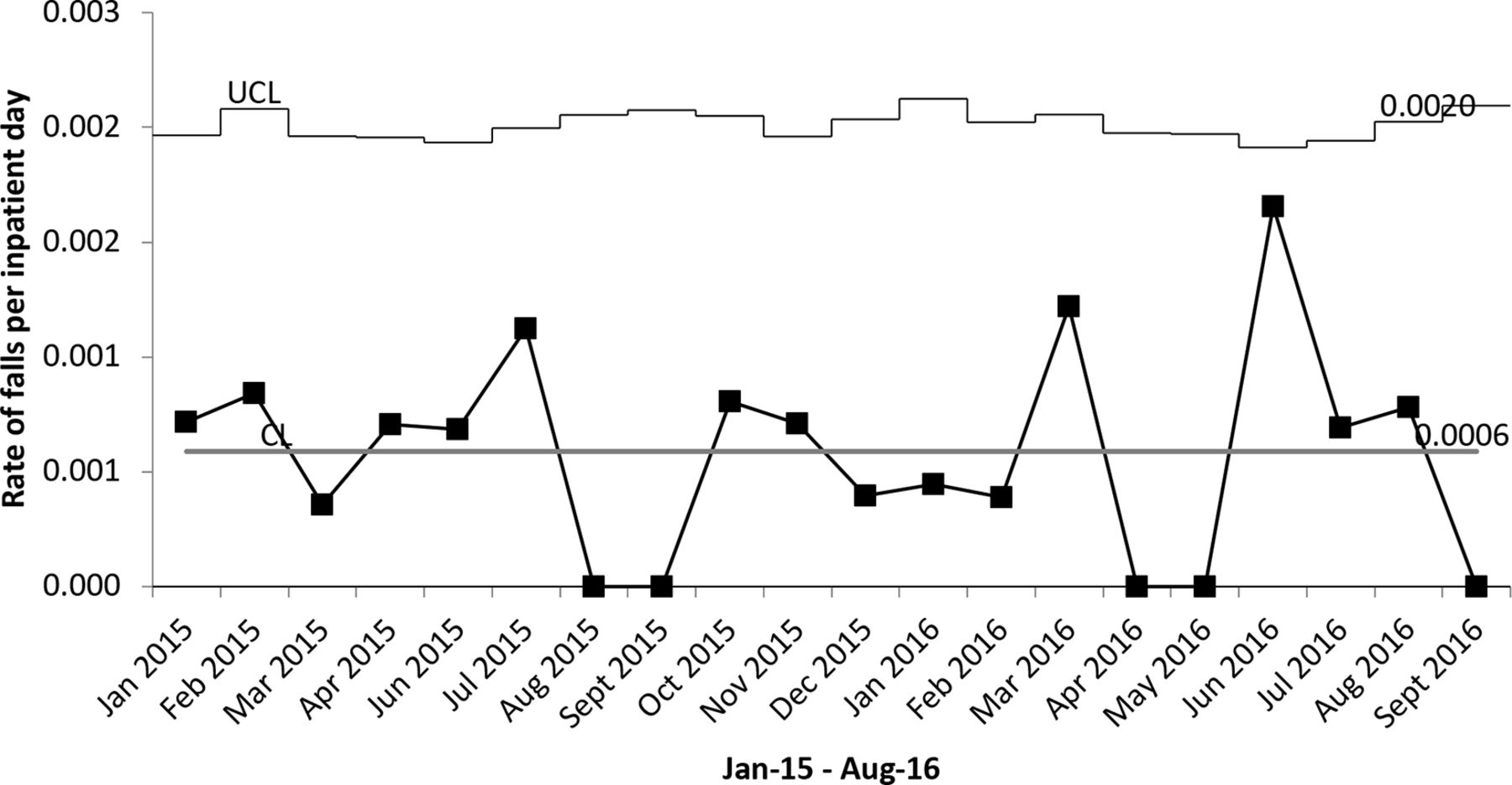
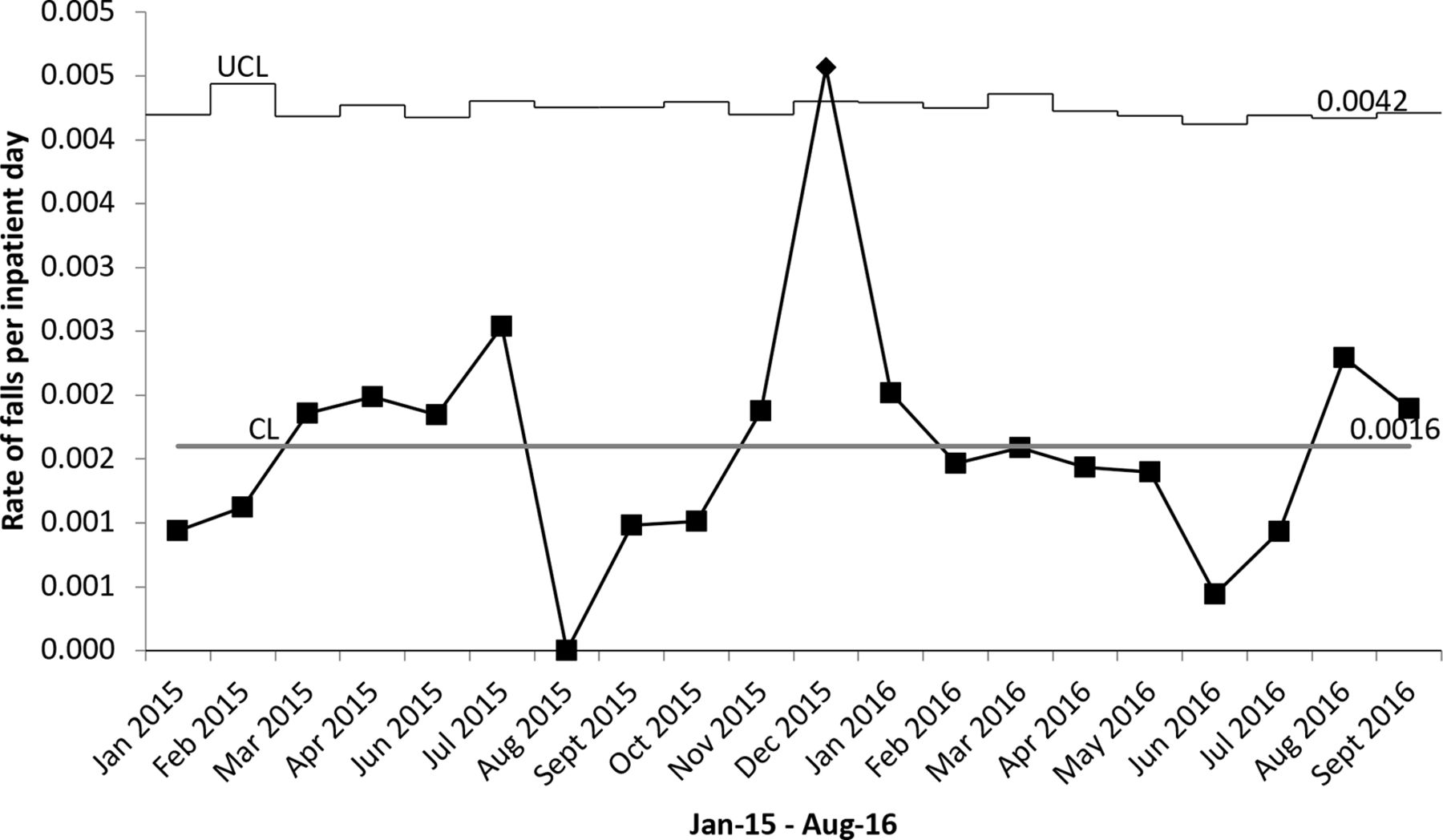
SPCs of aggregate measures of fall and prescriptions of dimenhydrinate remained stable in the intervention group during the study period without evidence of special cause variation (figures 4–6).

Monthly statistical process control p-chart of injurious falls per inpatient day on General Internal Medicine intervention units.
Monthly statistical process control p-chart of injurious falls per inpatient day on Cardiology intervention unit.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Biweekly statistical process control p-chart of proportion of patients prescribed dimenhydrinate on General internal medicine intervention units by discharge date.
Discussion
We found that a sedative reduction bundle was associated with an absolute reduction of 5.3% and a relative adjusted 33% reduction compared to the baseline rate of 15.8% in the proportion of new BSH initiation for insomnia among older hospitalised adults. We believe several factors contributed to the observed results. First, we achieved strong engagement of staff and hospital leadership support by aligning our project aim with hospital initiatives to reduce falls. Aligning the project goals with the corporate falls and delirium prevention strategy resulted in senior-level support to move the project forward. As a result, front-line staff used daily huddles to discuss sleep and sedative issues in the context of fall prevention and identified environmental and clinical monitoring opportunities to reduce sedatives.
A key project enabler was uncovered during patient engagement interviews to monitor for unintended consequences of removing sedatives from order sets such as worsening sleep quality. Patients identified the disruptive sleep environment as a driver for BSH prescriptions. This provided the impetus to implement sleep hygiene that contributed to the reduction in BSH prescriptions in the final PDSA cycle. Hearing the feedback from patients motivated nursing staff to minimise interruptions to sleep.
Our findings are novel in the effect size of BSH prescription reductions and in the comprehensiveness of the intervention where we incorporated PREMs. A single-centred Korean study implemented a sleep programme that included education to healthcare professionals and patients and promotion of non-pharmacological sleep hygiene.19 Study investigators found no change in new starts of BSH (RR=1.02, 95% CI 0.96 to 1.07). However, they noted a relative risk reduction of 0.82 (95% CI 0.79 to 0.86) in the proportion of inpatients discharged on a BSH. A controlled pre–post Australian study conducted in long-term care facilities examined the impact of education, staff training on non-pharmacological approaches to insomnia and symptoms of dementia, academic detailing and sedatives review conducted by pharmacists on overall antipsychotic and benzodiazepine prescribing patterns. Benzodiazepine prescription prevalence decreased from 31.8% to 26.9% (p<0.005).21 The intervention is similar to that described in our study; however, it was delivered in a different setting (long-term care), in conjunction with targeting antipsychotics use, and did not include PREMs.
Limitations
Several limitations of this study merit discussion. First, single-centre studies may require further evaluation to determine generalisability. However, other studies have demonstrated similar outcomes. Second, we were unable to demonstrate improvements in clinical outcomes such as falls. Yet, we were able to reduce risk of harm without negatively impacting on PREM (sleep quality). Third, we only measured BSH prescription rates rather than actual administration. However, the aim of this study was to reduce avoidable harm and exposure access to BSH-naive patients. We believe it is critical to influence prescribing patterns to impact administration of BSHs. Fourth, data collectors were unblinded; however, they were unaware of intervention start dates. Fifth, while we tracked attendance during GIM educational sessions, we did not quantify knowledge or attitude change. Clinician teams provided informal feedback to study teams indicating overwhelming support of the initiative. Sixth, sustainability data beyond 2016 was out of scope for this study. However, in March 2018, our QI team carried out a point-prevalence sustainability audit on the GIM units (comprising of nearly 90% of patients in our study cohort) and found a rate of 9% for our outcome measure of new sedative prescription initiation in hospital among naive inpatients. We were reassured that the intervention appears to have translated into sustained practice changes. Seventh, the control group differed in several ways from the intervention group such as age which may have contributed to observed differences in the results. However, the rationale of the control group was to allow trending of BSH prescribing rates over time within each group, which we found remained stable among controls. Finally, observational studies can only provide associations without proven causality and require further study with a rigorous evaluation strategy. It is possible that factors external to our intervention contributed to the observed results; however, the lack of similar reductions in BSH prescriptions on the control ward suggests that our intervention may be responsible for the observed improvements on the intervention wards.
Conclusions
Unnecessary BSH use in hospital continues to expose patients to preventable harm and can lead to long-term dependency. A multifaceted, patient-centred intervention bundle was associated with decreased BSH initiation among older medical inpatients. Further study and evaluation are warranted.
Acknowledgments
We would like to thank John Matelski MSc, Biostatistics Research Unit, University Health Network; and Dalia Othman, Sinai Health System, for their valuable contributions to data analysis and collection, respectively, related to this project. We also extend our gratitude to the medical and cardiology inpatient teams at Mount Sinai Hospital who made this project possible.
References
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available.