Article Text

Abstract
Objective To set priorities to improve consultations, care structures and the healthcare system from the perspective of patients with chronic conditions, care professionals, hospital administrators and health policy makers.
Methods Adult patients with chronic conditions recruited from the ComPaRe e-cohort in France ranked their 15 most important areas of improvement among 147 previously defined by patients. Priorities at a population level were obtained by using logit models for sets of ranked items in a data set calibrated to represent the French population of patients with chronic conditions. Care professionals, hospital managers and health policy makers rated the complexity involved in improving the areas identified. We calculated the number of patients who considered as a priority at least one of the areas considered easy to implement.
Results Between September 2018 and May 2019, 3002 patients (84% women, 47% with multimorbidity) and 149 professionals (including 50 care professionals, 79 hospital directors, 11 health policy decision makers) were recruited. Patients’ top priorities were (1) Transforming care to be holistic and personalised, at a consultation level; (2) Smoothing patients' journey in the care system, increasing their knowledge of their own health and improving care coordination, at a care structure level (3) Training clinicians in better interpersonal skills and knowledge of specific conditions/treatments, reducing stigma and making care more affordable, at a healthcare system level. In total, 48%, 71% and 57% patients ranked in their top priorities one area considered easy to improve by professionals at consultation, care structure and health system levels, respectively.
Conclusion This is the first comprehensive map of patients’ priorities to improve the management of chronic conditions. Implementing simple actions could benefit a large number of patients.
- health services research
- healthcare quality improvement
- patient-centred care
Data availability statement
Data are available upon reasonable request. All data are available under the rules of the ComPaRe e-cohort.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
In modern Western countries, 40% of adults have at least one chronic condition and 23% have multiple conditions and are therefore considered multimorbid.1 2 From the healthcare system perspective, the management of chronic conditions and multimorbidity is a jigsaw puzzle: increasing numbers of patients seek care over extended periods of time,2 and each patient requires coordinated inputs from a wide range of health professionals and institutions that have traditionally been separate.3
Yet, most Western care systems remain structured around disease-by-disease episodic care processes that are ill-equipped to meet the requirements of people with chronic conditions and multimorbidity.4–7 As a result, in addition to their diseases and symptoms, patients must adapt to the structural and interactional limitations of the care system in which they seek care, including inequalities in care access, poor organisation of care structures, time-limited consultations, disease-centred reimbursements.8 9 The burden imposed on patients by their care is such that 40% of patients with chronic conditions, independent of their diseases and context, consider that they would not be able to continue the same investment of time, energy and money in healthcare lifelong.10 11
Improving care for patients with chronic conditions and multimorbidity is a daunting process. Possibly, no other sector has equivalent intricate funding models, multiple moving parts, complicated ‘clients’ with diverse needs, and so many potential options and interventions to answer these needs.12 Surprisingly, to our knowledge, the simple question of ‘where to start’ has never been asked and we have no evidence available for prioritising interventions (among the hundreds that have been developed and tested at the organisation level or patient level) and for whom.13 14
To answer this question, we adopted a citizen science approach and leveraged the collective intelligence and collaboration of large groups of non-professional people.15 In a previous study, we involved a large number of patients with chronic conditions in France to elicit their perspectives on how to improve the care of patients with chronic conditions.16 A sample of 1636 patients with chronic conditions was asked ‘If you had a magic wand, what would you change in your healthcare?’, with an open-ended response. Their answers enabled the inductive identification of 147 areas of improvement to transform consultations, care structures and the healthcare system. However, because the study was based on questions with open-ended responses, how propositions from patients would be prioritised or valued by different groups remained unclear. Areas of improvement frequently mentioned were not necessarily those most ‘desired’ by participants but those that were the most evident to them.
In the present research, we aimed at (1) prioritising, from patients’ perspectives, the areas of improvement previously identified and, (2) determining how complex these priority improvements would be to implement.
Methods
This study involved two complementary parts. First, we involved a large number of patients with chronic conditions in setting patients’ priorities for improving the management of chronic conditions in France. Second, we asked a group of professionals in care, care quality improvement and health policy to determine how complex these priority improvements would be to implement.
Setting patients’ priorities for improving the management of chronic conditions
We surveyed patients with chronic conditions to understand how they prioritised and valued 147 areas of improvement, identified by patients in a previous research.16 During that study, a working group of researchers and patients classified each area of improvement by their ‘level’, that is, the people and structures involved, and ‘overarching category’, that is, the topic. For example: the area of improvement ‘Develop online training programmes for patients’ was classified as an improvement at the ‘care structure’ level, in the overarching category ‘Increase patients’ knowledge of their own health’, and the area ‘Avoid giving patients false hopes’ was classified as an improvement at ‘consultation’ level in the overarching category ‘Create the context for real discussions with patients’. A detailed description of areas of improvement, overarching categories and levels is published elsewhere.16
Adult patients with chronic conditions were recruited from the ‘Community of Patients for Research’ (ComPaRe, http://compare.aphp.fr), an ongoing citizen science project based on an e-cohort of patients with chronic conditions in France. Participants of ComPaRe are adults (>18 years old) who report having at least one chronic condition (defined as a condition requiring healthcare for at least 6 months) and who join the project to donate time to accelerate research of their conditions by answering regular patient-reported outcomes and patient-reported experience measurements online.17 18 Recruitment in ComPaRe entails direct outreach to potential participants by widespread advertising in general and social media and partner patient associations. As a result, the population in ComPaRe is not representative of the French population of patients with chronic conditions. Yet, it covers diverse sociodemographic backgrounds, including socioeconomically disadvantaged individuals.19 All participants provide electronic consent before participating in the e-cohort.
Patients were invited by email to participate. Three reminders were sent to increase participation rate. Those agreeing to participate were randomised to three groups, each assessing the importance of areas of improvement at consultation, care structure or healthcare system level (ie, a given participant only assesses areas of improvement from the level assigned at random).16 Within each group, patients identified their priorities for improvement by using a novel two-step method inspired by Q methodology. First, each patient selected the 15 areas for improvement he/she felt were the most important (step 1). Second, the patient sorted these 15 areas of improvement within a constrained template in which only 1 area could be considered ‘most important’, 2 areas could be considered ‘very important’, 3 areas could be considered ‘moderately important’ and 9 areas could be considered of ‘minor importance’ (step 2) (online supplementary appendix 1). This method reduced the number of items to be ranked, thereby easing the participants’ tasks and increasing the reliability of the ranking process.20 Therefore, for each patient, output of the ranking process involves a ranking of these 15 top priorities, with ties.
Supplemental material
Assessments of the complexity involved in implementing actions to improve areas identified by patients
We surveyed care professionals, experts in quality improvement, hospital administrators and health policy makers about their perception of the complexity involved in implementing actions to improve the 147 areas of improvement identified previously.16 These professionals were recruited (1) During a national meeting of the federation of regional organisations responsible for the improvement of hospital care in France (Lyon, 2019); (2) By inviting hospital carers, directors and managers from the Assistance Publique−Hôpitaux de Paris hospitals; (3) By contacting alumni from the ‘Ecole des Hautes Etudes en Santé Publique’, which trains hospital directors and managers in France (4) By inviting all members of the French Parliament and Senate part of commissions for Health and Social Affairs.
Each professional connected on a secured website (http://clinicalepidemio.fr/VAM) and was presented with 15 areas for improvement selected at random from one of the three sets of areas for improvement (consultation, care structure or healthcare system levels). Areas of improvement presented were tailored to the professional’s field: care professionals were invited to evaluate areas of improvement at the consultation level; hospital managers were invited to evaluate areas of improvement at the care structure level; and health policy makers were invited to evaluate areas of improvement at the healthcare system level.
Professionals were asked to rate the difficulty in implementing actions according to the area of improvement, taking into account costs, potential resistance to change, difficulties to motivate the people involved and time needed to achieve results. Ratings ranged from 1 (extremely easy to implement) to 10 (extremely difficult to implement) or could be ‘I am not qualified to assess the complexity to implement actions to improve this area’.
Statistical analyses
Setting patients’ priorities for improving the management of chronic conditions
In each level (consultation, care structure, healthcare system), we fitted logit models to the ranking data (step 2) to prioritise areas of improvement by importance. The logit models calculate the odds, for an area of improvement, to be ranked better than a reference area of improvement (here chosen as the area with the lowest importance). Therefore, models generate a general ranking for all areas of improvement, at a population level.21 To summarise results, we presented, for each overarching category, the median odds to be ranked better than the reference area of improvement.
We complemented our analyses by using a weighted data set obtained by calibration on margins of our data with weights for age categories (<24, 25–34, 35–44, 45–54, 55–64, 65–74, >75 years old), gender and educational level (low, middle school or equivalent, high school or equivalent, associate’s degree, higher education). Weights were derived from national census data describing the French population reporting chronic conditions.22 23
Analyses were conducted both globally and in subgroups defined by multimorbidity (patients’ reported number of conditions ≥2 or not) and duration since the diagnosis of the first chronic condition (<8 or ≥8 years; threshold was the median duration since diagnosis).
Assessments of the complexity involved in implementing actions for patients’ propositions
For each area of improvement, we summarised the difficulty in implementing actions by the median and IQR. Data for ‘I am not qualified to assess the complexity to implement actions to improve this area’ were left out of analyses. We then calculated the number (proportion) of patients who would benefit from the implementation of all actions with a median difficulty ≤3. We considered those who selected at least 1 of these areas of improvement among their 15 most important actions (for all patients who participated) or among their top 6 actions (for patients who participated in step 2 and who provided the ranking of their selection).
Results
Between September 2018 and May 2019, 3002 patients (2534 (84%) women) were recruited in the study (participation rate: 93%) (online supplementary appendix 2). The mean age was 43 years (SD=14) and 1440 (47%) participants had multimorbidity (mean number of conditions 2·2 (SD=2·1)) (table 1). Patients’ conditions included diabetes (n=171), high blood pressure (n=225), thyroid disorders (n=221), rheumatological conditions (n=649), neurological disorders (n=416), dermatological conditions (n=321), digestive conditions (n=306) and cancer (n=179). Characteristics of patients in the weighted data set are presented in online supplementary appendix 3.
Patients’ characteristics (n=3002) by evaluation of propositions to improve consultations, care structures and the healthcare system
Between December 2019 and January 2020, 149 professionals (106 (71%) women) provided 2196 evaluations of the complexity involved in implementing actions for areas of improvement. These professionals were care professionals (n=50), health quality managers (n=19), hospital directors and managers (n=60), and health policy decision makers (n=11, including 6 members of the French Parliament or Senate). Their mean age was 44 years (SD=11).
Setting patients’ priorities for improving the management of chronic conditions
Priorities for improvement at consultation level
At the consultation level, 1021 patients selected their 15 most important areas for improvement and 840 (82%) ranked them. Patients’ top priorities to improve consultations are presented in table 2. Overall, patients’ highest rankings were for areas of improvement in overarching categories related to holistic care (median odds to be ranked better than the reference area ‘allow flexibility in drug intakes’: 38·8 (IQR 18·4–40·9)) and personalised care and care goals (median odds: 20·4 (IQR 14·3–25·8)). Lowest rankings were for improvements in patients’ treatment and home care (median odds: 2·7 (IQR 1·4–6·6)) (figure 1). Results were unchanged in the calibrated data set reflecting the characteristics of the French population of patients with chronic conditions (weighted data set) (online supplementary appendix 4a).

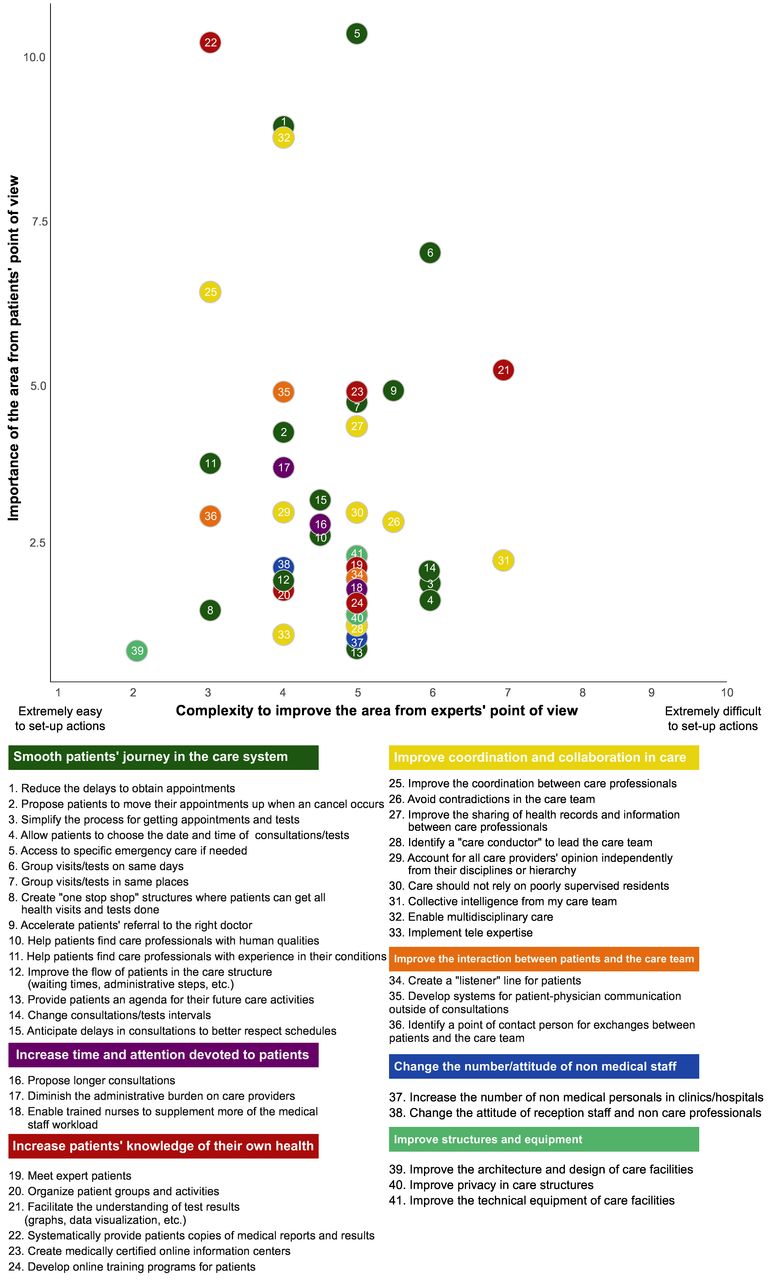
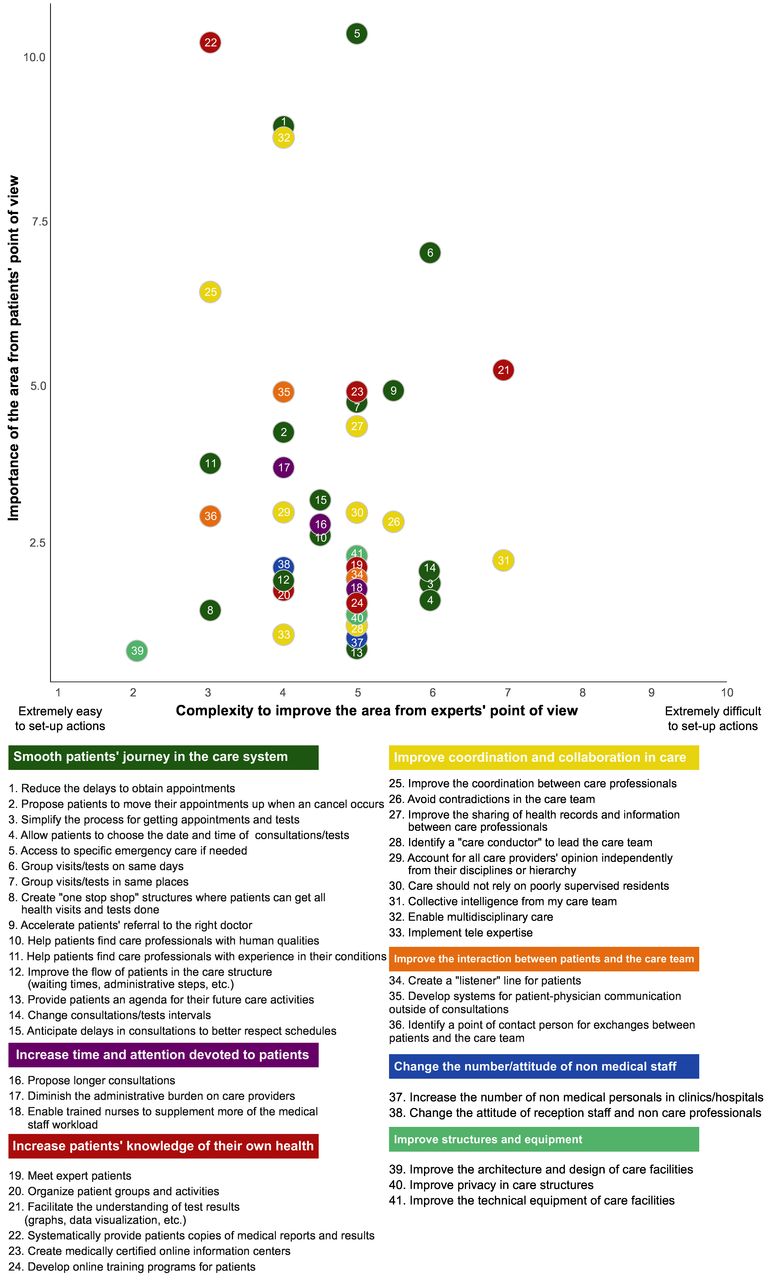
Comparative importance of areas of improvement at the consultation level, from patients’ point of view (n=840) and their complexity for implementation from professionals’ point of view (n=38). Importance of each area of improvement is represented by its odds to be ranked better than the reference area of improvement ‘allow flexibility in drug intakes’. Complexity was assessed by care professionals, hospital managers and health policy decision makers, with ratings ranging from 1 (extremely easy to set up actions) to 10 (extremely difficult to set up actions). Areas of improvement are organised in overarching categories (colours).
Top six priorities for improvement at the consultation, care structure and health system levels and the complexity for their implementation
Presence/absence of multimorbidity and duration since the diagnosis of the first chronic condition did not change the ranking of priority areas of improvement for consultations (online supplementary appendix 4b,4c).
Priorities for improvement at care structure level
At the care structure level, 1013 patients selected their 15 most important areas for improvement and 802 (79%) ranked them. Patients’ top priorities to improve care structures are presented in table 2. Overall, patients provided high rankings for areas in all overarching categories. Top priorities involved overarching categories related to improvements to smooth patients’ journey in the care system (median odds to be ranked better than the reference area ‘Improve the architecture and design of care facilities’: 3·9 (IQR 2·1–5·0)), increasing patients' knowledge of their own health (median odds 3·6 (IQR 2·1–5·2)) and improving coordination and collaboration in care (median odds 3·1 (IQR 2·7–5·4)). Lowest priorities were to improve structures and equipment (median odds 1·7 (IQR 1·3–2·0)) (figure 2). Results were overall similar in the weighted data set but top priorities were to develop access to specific emergency care for patients with chronic disease and to group visits and tests on the same days if possible (online supplementary appendix 5a).
Comparative importance of areas of improvement at the care structure level, from patients’ point of view (n=802) and their complexity for implementation from professionals' point of view (n=78). Importance of each area of improvement is represented by its odds to be ranked better than the reference area of improvement ‘improve the architecture and design of care facilities’. Complexity was assessed by care professionals, hospital managers and health policy decision makers, with ratings ranging from 1 (extremely easy to set up actions) to 10 (extremely difficult to set up actions). Areas of improvement are organised in overarching categories (colours).
Presence/absence of multimorbidity and time since the diagnosis of the first chronic condition did not change the ranking of priority areas of improvement for care structures (online supplementary appendix 5b,5c).
Priorities for improvement at the healthcare system level
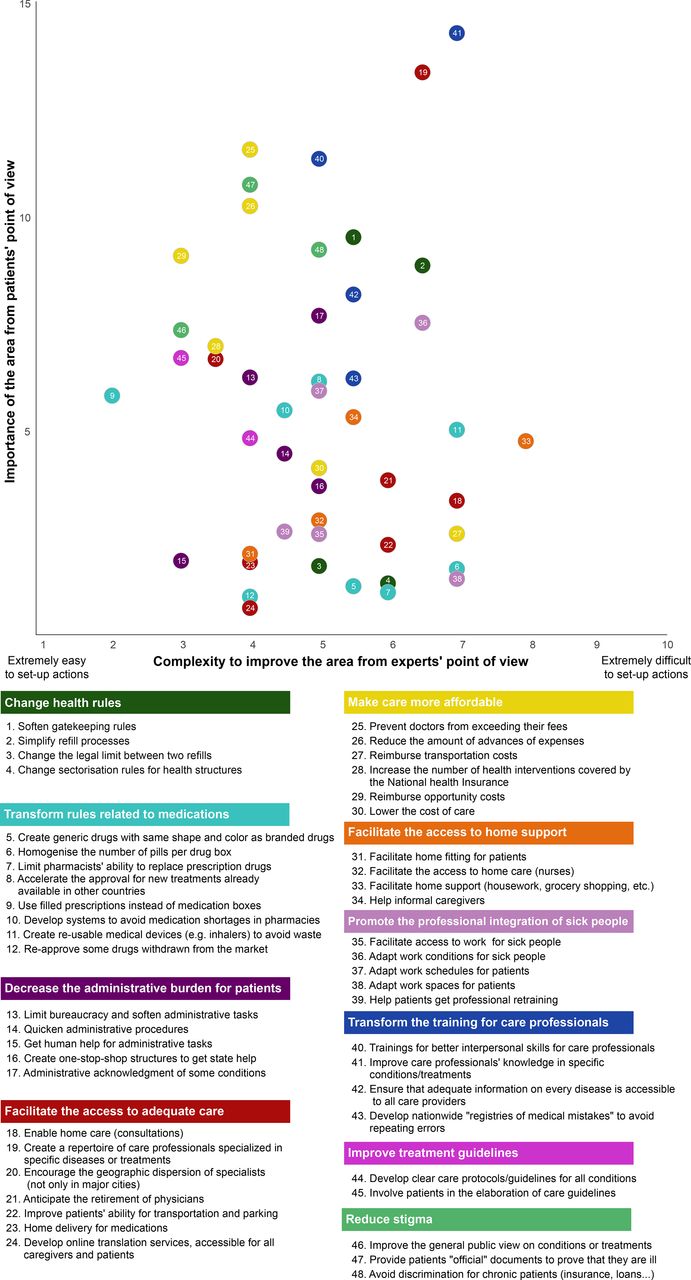
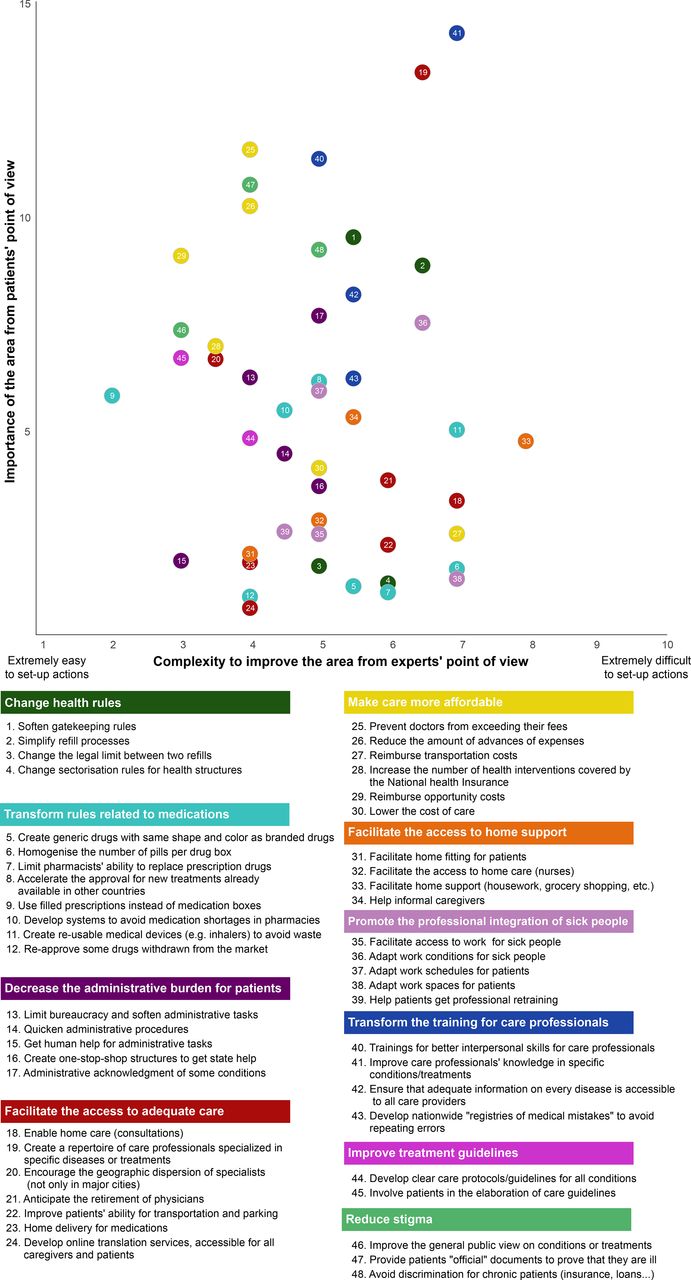
At the healthcare system level, 968 patients selected their 15 most important areas for improvement and 745 (77%) ranked them. Patients’ top priorities to improve the healthcare system are presented in table 2. Overall, patients’ highest rankings were for areas of improvement in overarching categories related to improving the training of care professionals for better interpersonal skills or knowledge in specific conditions/treatments (median odds to be ranked better than the reference area ‘Develop online translation services, accessible for all care professionals and patients’: 9·9 (IQR 7·8–12·2)), reducing stigma for patients with chronic conditions (eg, via actions to improve the public’s views on conditions) (median odds: 9·3 (IQR 8·4–10·1)) and making care more affordable (median odds: 8·1 (IQR 4·9–10·0)). Lowest priorities were to promote the professional integration of sick people (median odds: 2·7 (IQR 2·7–6·0)) (figure 3). Results were slightly changed in the weighted data set where the top priority was to soften gatekeeping rules (ie, having to consult a general practitioner before seeing a specialist) (online supplementary appendix 5a).
{kind=link}
{kind=link}
{kind=link}
Comparative importance of areas of improvement at healthcare system level, from patients’ point of view (n=745) and their complexity for implementation from professionals' point of view (n=33). Importance of each area of improvement is represented by its odds to be ranked better than the reference area of improvement ‘develop online translation services, accessible for all care professionals and patients‘. Complexity was assessed by care professionals, hospital managers and health policy decision makers, with ratings ranging from 1 (extremely easy to set up actions) to 10 (extremely difficult to set up actions). Areas of improvement are organised in overarching categories (colours).
Presence/absence of multimorbidity and duration since the diagnosis of the first chronic condition did not change the ranking of priority areas of improvement for care structures (online supplementary appendix 6b,6c).
Assessments of the complexity involved in implementing actions to improve areas identified by patients
Assessments of the complexity involved in implementing actions to improve consultations
In total, 38 professionals (76% care professionals) provided 462 evaluations of the complexity in implementing actions to improve consultations (average of 8 evaluations per area of improvement). Median complexity to implement actions for consultations ranged from 3/10 (to introduce patients to patients' associations) to 7/10 (to enable drug holidays if possible and to prevent exacerbations rather than wait for them) (figure 1). Their opinions showed high agreement, with an average IQR of 2·2 (min: 0·2, max: 4·2) in their ratings (online supplementary appendix 4d). In total, 87% and 48% of patients selected at least one area of improvement considered easy to implement (median complexity ≤3) among their top 15 and top 6 priorities, respectively, at the consultation level.
Assessments of the complexity involved in implementing actions to improve care structures
In total, 78 professionals (69% health quality managers and hospital directors) provided 1251 evaluations of the complexity in implementing actions to improve consultations (average of 30 evaluations per area of improvement). Median complexity to implement actions for consultations ranged from 2/10 (to improve the architecture and design of care facilities) to 7/10 (to develop ways to facilitate the understanding of test results for patients and develop methods to encourage collective intelligence from my care team) (figure 2). Their opinions showed high agreement, with an average IQR of 2·9 (min: 1·8, max: 6) in their opinions (online supplementary appendix 5d). In total, 98% and 71% of patients selected at least one area of improvement considered easy to implement (median complexity ≤3) among their top 15 and top 6 priorities, respectively, at the care structure level.
Assessments of the complexity involved in implementing actions to improve the healthcare system
In total, 33 professionals (33% decision makers) provided 483 evaluations of the complexity in implementing actions to improve the healthcare system (average of 10 evaluations per area of improvement). Median complexity in implementing actions for consultations ranged from 2/10 (propose filled prescriptions instead of medication boxes) to 8/10 (propose home support (housework, grocery shopping, etc) for patients with chronic conditions) (figure 2). Their opinions showed high agreement, with an average IQR of 2·7 (min: 0·8, max: 5·8) in their opinions (online supplementary appendix 5d). In total, 91% and 57% of patients selected at least one area of improvement considered easy to implement (median complexity ≤3) among their top 15 and top 6 priorities, respectively, at the healthcare system level.
Discussion
In this study, we involved 3002 patients with chronic conditions and multimorbidity in France in the process of prioritising patient-defined areas of improvement at consultation, care structure and healthcare system levels. We completed the priority setting by asking 149 care professionals, hospital administrators and health policy makers to determine how complex actions would be to implement for the identified areas of improvement. In total, 48%, 71% and 57% of patients ranked in their top six priorities for improvement at least one area considered easy to improve by professionals at consultation, care structure and health system levels, respectively.
Overall, the overarching principles for improvement identified by patients are consistent with chronic care models advocated in the medical literature,24 but further comparison is limited by the breadth of our findings because previous priority surveys covered specific contexts or diseases.25–27 To our knowledge, this is the first comprehensive map of all unmet needs in the management of chronic conditions and multimorbidity in France. This map may help stakeholders (clinicians, hospital managers, health policy decision makers) make informed choices on where to allocate time, effort and resources in healthcare and define objectives for improvement at both the macro level (ie, by considering the priorities of patients with chronic conditions, as a single and large group) and micro level (ie, by considering the priorities of patients with certain conditions, of a certain age, with multimorbidity etc).28 In particular, our results are strengthened by the calibration of our data set to represent the French population reporting chronic conditions in terms of age, gender and educational level. This enabled the extrapolation of our results at a national level.
Methods used in our study contrast with the literature on how care for chronic patients should be transformed. Indeed, new care models and programmes for patients with chronic conditions have been devised by (1) Experts’ opinions, without or with minimal involvement from patients.24 29 (2) Experiences limited to specific settings, contexts or diseases.30 In complement with our previous article, we present the proof of concept of a scientific method to capture patients’ voices, on a large scale, to guide the design of care by (1) Identifying patients’ needs and ideas to improve healthcare.16 (2) Ranking the identified needs. Our methods leverage large online surveys and novel ranking methods that can reduce the cognitive burden for participants (although not evaluated in this study), which can be easily reproduced in different contexts, populations or countries. Our methods also differ from usual priority settings that use consensus methods such as the Delphi method, because we clearly separated the collection of patients’ views (presented in this study) from the potential decisions that may be taken based on findings.
Our study had several limitations. First, we considered patients with chronic conditions as a single large entity. Despite the analysis of some subgroups, our results are a general overview of patients’ preferences at a population level. This situation may mask values and priorities of specific groups of patients. Future work could involve the re-analysis of our data to better understand the fine-grained topology of patients’ perspectives to define care improvement programmes and targets for specific populations. Second, professionals’ judgements on the complexity to implement actions were based on subjective assessments that were not related to a single ‘measurement unit’ (eg, monetary costs). This methodological choice aimed at easing data collection makes the comparison of ratings and the evaluation of the investments required difficult. Third, the number of professionals evaluating each proposition was relatively low but was still consistent with numbers recommended in the literature, from empirical experience, to obtain acceptable estimates.31 32 Fourth, despite the use of methods to enhance the representativeness of estimates that have been found effective in e-cohorts, a generalisation of our findings is cautioned because primary data were based on volunteers who were younger, more educated and more often female than the French population of patients with chronic conditions.19 Finally, transferability of our findings at an international level is cautioned. Patients’ priorities reflect their unmet needs within the organisations and systems in which they sought care. Thus, specificities of the French healthcare model (eg, universal health coverage, institutional polycentrism) directly affected both patients’ ideas to improve the system and their importance from patients’ views.
Our study showed that actions to improve patients’ experience are not necessarily difficult or costly. It may even be the contrary. Actions considered easy to implement, by experts, were considered as priorities for large numbers of patients with chronic conditions and multimorbidity. In complement with our previous study, our approach thus allows for the identification of priority areas of improvement. Further steps will require finding actionable solutions. This may be achieved with the help of patients with methods such as co-design.16 33 Of course, improvement should target all priorities from patients and not only those considered easily ‘actionable’.
Our work stands as a new model to engage large numbers of patients in care improvement that can be replicated in other populations, contexts and countries. Methods presented in this paper can be easily scaled up to complement current systems to assess the quality of care. Repetition could then inform the dynamics of gaps in care management. As such, our study sets the foundation for methods supporting evidence-based health policy, whereby decisions from stakeholders to transform the system are guided by data on patients’ needs, collected during scientific and replicable processes, rather than the opinions, anecdotes and aspirations of a few people.34
Future challenges will be to act on our results. A large cluster of priorities for improvement involved the need for clinicians to reconsider the patient-clinician relationship and to improve their human skills. Patients feel unheard and judged. Pain is still undiagnosed and underestimated by carers.35 Changing the mindset of care professionals, at scale, would entail rethinking medical studies and education. Such transformation will require the development of new methods of knowledge transmission, development of reflective practice, and providing medical students with a supportive environment. However, results will not be immediate.36 At the care structure and health system levels, kind and careful care for patients will not be achieved without re-designing care processes to slow down and give care professionals time to care for their patients. Implications are daunting because this would require modifying how care structures and professionals make money. We depict here a colossal work. To achieve it, one promising way could be to enlist patients in enacting change, in a Patient Revolution.37
Conclusion
This study generated the first comprehensive map of patients’ priorities to improve consultations, care structures and the healthcare system in France. About 70% of patients would benefit from the implementing actions that professionals considered easy to implement.
Data availability statement
Data are available upon reasonable request. All data are available under the rules of the ComPaRe e-cohort.
Ethics statements
Ethics approval
ComPaRe was approved by the Comité de Protection des Personnes Ile de France 1 (IRB: 0008367).
Acknowledgments
The authors thank Laura Smales (BioMedEditing, Toronto, Canada) for editing and Elise Diard for help in drafting figures.
References
Footnotes
Twitter @thitran3
Contributors Generated the idea: V-TT and PR; Conceived and designed the experiments: V-TT, ED and PR; Collected data: V-TT and ED; Analysed data: V-TT; Wrote the first draft of the manuscript: V-TT; Contributed to the writing of the manuscript: V-TT, ED and PR; Agree with manuscript results and conclusions: V-TT, ED and PR; V-TT is the guarantor, had full access to the data in the study, and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.