Article Text

Abstract
Background For over a decade, the preoperative timeout procedure has been implemented in most paediatric surgery units. However, the impact of this intervention has not been systematically studied. This study evaluates whether purposefully introduced errors during the timeout routine are detected and reported by the operating team members.
Methods After ethics board approval and informed consent, deliberate errors were randomly and clandestinely introduced into the timeout routine for elective surgical procedures by a paediatric surgery attending. Errors were randomly selected among wrong name, site, side, allergy, intervention, birthdate and gender items. The main outcome measure was how frequent an error was reported by the team and by whom.
Results Over the course of 16 months, 1800 operations and timeouts were performed. Errors were randomly introduced in 120 cases (6.7%). Overall, 54% of the errors were reported; the remainder went unnoticed. Errors were pointed out most frequently by anaesthesiologists (64%), followed by nursing staff (28%), residents-in-training (6%) and medical students (1%).
Conclusion Errors in the timeout routine go unnoticed by the team in almost half of cases. Therefore, even if preoperative timeout routines are strictly implemented, mistakes may be overlooked. Hence, the timeout procedure in its current form appears unreliable. Future developments may be useful to improve the quality of the surgical timeout and should be studied in detail.
- human error
- medical error
- measurement/epidemiology
- Paediatrics
- safety culture
- surgery
Data availability statement
The anonymised, non-identifiable data this study is based on are available upon request. Requests should be directed to the corresponding author. Reuse is permitted for scientific purposes and quality initiatives.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
In 2008, the WHO launched the Surgical Safety Checklist as part of the Global Patient Safety Challenge in an effort to reduce surgical morbidity and mortality worldwide.1 Since then, the preoperative timeout procedure has been implemented in most operating rooms and most paediatric surgery units. In our hospital, a standardised team-timeout routine, based on the WHO checklist, is performed before every operation.
Checklists are lists of crucial tasks to be addressed in a specific order so that no important steps are forgotten. They are often used in aerospace environments, where they have been extensively studied and have shown to improve aviation safety.2 On this basis, surgical safety checklists were created to improve team communication, create a systematic and comprehensive review of critical datapoints, ensure the execution of important tasks and flatten the hierarchy that often characterises the culture of surgical teams,3 with an ultimate goal to improve patient safety. Checklists may be implemented in the form of mnemonics, printed lists, posters or electronic means. The adaptability of checklists to the healthcare environment has been critically appraised, particularly because of the complexity of the individual items and their narrative, unreproducible measures of compliance and variability in outcome.4 A systematic review of 20 published studies found that implementation of a surgical checklist had the potential of decreasing mortality by 47%–62% and morbidity by around one-third.5 Another review confirmed decreases in complications, mortality and surgical site infections by ORs of 0.59, 0.77 and 0.57, respectively.6 Similarly, a large epidemiological study demonstrated a reduction in mortality by an OR of 0.6.7 In contemporary practice, over three-quarters of hospitals worldwide use surgical checklist timeouts.8
On the other hand, a well-performed meta-analysis found mixed, less encouraging impact of surgical checklists on mortality and complications.9 This report found substantial heterogeneity of the available studies on the topic, particularly regarding study design, setting and surgical specialty. In a recent observational study, the interaction between the timeout participants was found to be complete in only half of 200 observed elective surgeries,10 indicating that important items may be missed. This was confirmed in a study using snapshot audits that found team-timeout errors in 40%–60% of cases.11
Consequently, there remains considerable uncertainty regarding the quality and performance of the surgical checklist timeout procedure, including its true efficacy for picking up critical mistakes.12 For checklists to be effective, however, it is important not only that the listed items be mentioned but also that potential errors be pointed out by the team. To date, there are practically no data on how often errors in the timeout procedure are effectively identified or overlooked. Therefore, this study evaluates whether purposefully introduced random errors during the timeout routine are reported by the team. This study was designed compliant with the Consolidated Standards of Reporting Trials (CONSORT) 2010 criteria.13
Methods
Study design
Deliberate errors were randomly, intermittently and clandestinely introduced into the surgical checklist timeout routine for elective paediatric surgical procedures by two attending paediatric surgeons. Errors were randomly selected among predefined categories including wrong name, intervention, site, side, allergy, birthdate or gender using random lists and block sizes of 100 patients each. Randomisation was performed by one of the authors. In order not to raise any suspicion by team members, fewer than 1 in 10 cases was selected for deliberate error placement, and cases were randomly selected from medical record numbers to avoid noticeable inclusion patterns.
Team members included the surgical resident or fellow, the anaesthesiologist, anaesthesia nursing, scrub nurse, as well as nursing and medical students. None of these team members were aware of the study.
Error reporting rates were assessed for the cases in which errors were deliberately introduced. No data were collected on the other cases performed during the study period. Since these were the vast majority of cases performed in the study, their purpose was to conceal cases with deliberate errors so that they would not be anticipated by members of the team.
The study did not measure departmental adherence with the standardised timeout procedure, since all cases included in the analysis were performed by the investigators.
Timeout procedure
The standardised timeout strictly followed the format of the WHO Surgical Safety Checklist.1 In brief, in our department, the attending paediatric surgical attending commences the timeout procedure after positioning the patient and before the prep and drape by loudly verbalising ‘timeout’ in the operating room. A paper guide is available and can be viewed by the surgeon. At this time, all other non-essential activities must cease and the team’s attention focuses only on the timeout procedure. Using the written consent form of the patient, the surgeon verifies the patient’s name, birthdate and the procedure to be performed, as well as the laterality if applicable. In interventions with laterality, the site is marked in the presurgical checklist before entering the operating suite. Special or potentially complicating issues are then mentioned. The surgeon checks that all imaging is displayed for the procedure, if applicable. Finally, the surgeon states whether preoperative antibiotic prophylaxis is necessary, whether there are allergies, or any critical steps anticipated, and if blood should be available for the operation. Subsequently, the anaesthesiologist takes over by describing the type of anaesthesia given, the patient’s weight, as well as any recorded allergies. The anaesthesiologist confirms if antibiotic prophylaxis was given, describes the number and types of intravascular access routes present, and whether blood products have been typed and crossed or are available in the operating room. Finally, the nursing staff confirms that the appropriate instrumentation for the procedure is available, sterile and complete. They ask about the estimated time of the procedure and when the next patient should be called for, which is answered by the surgeon. The surgeon then asks if all team members agree with the issues noted during the timeout. Team members are instructed to verbalise any discrepancies. Unknown team members are asked to introduce themselves and their function. If all agree, the operation commences. Until that point, there is a written policy in our department that no scalpels or cautery instruments are handed over, unless in emergency situations. The timeout is recorded on a standard surgical safety checklist paper form by the surgical resident.
Error generation
Cases and type of error (name, intervention, site/side, allergy, gender and age) were selected for error introduction by random lists on the morning of the particular case. The type of error to be introduced was randomly assigned and verbally communicated to the surgeon investigator before the case according to the list. The actual error was generated at the discretion of the attending surgeon according to a prescripted set of rules. When applicable, typical first and surnames were substituted in lieu of the actual name; interventions were used that affected the same body region (eg, an orchidopexy instead of an inguinal hernia); sides were switched (right for left); allergies were declared when none were actually present, or vice versa. Gender was switched, and age was falsely modified within a 50% margin (a 10 year old was falsely declared a child within a range of 5–15 years).
Outcome parameters
The study’s main outcome measure focused on how frequent an error was reported by the team and by whom, as well as the type of error. Error detection was defined as someone in the operating room reacting to the error by verbal interjection by the end of the physician’s timeout. This was documented by a senior medical student or designee.
Inclusion and exclusion criteria
Patients were included if they underwent elective, non-emergent surgery in our paediatric surgery operating room on our campus and the parents or legal guardian gave written consent for study participation. Exclusion criteria included refusal to participate by the parents, legal guardian or the patients themselves. Also, for safety reasons, patients were not included if they were operated in other operating rooms, facilities or institutions.
If the error was not positively identified by the end of the physician’s portion of the surgical safety checklist procedure, the ethics comittee requested that the attending paediatric surgeons verbalise a correction before proceeding, as illustrated in the following example:
Attending surgeon: ‘This is patient X, born on Y, who is a Z year old boy who is here for a right inguinal hernia repair. The site is marked and the consent has been signed by the parents. We are anticipating minor, negligible blood loss’ (correct).
Attending surgeon: ‘The patient is otherwise healthy and has no allergies’ (incorrect—the patient has a documented allergy to amoxicillin).
Anaesthesia attending: ‘The patient is ASA class 1, we have an intravenous catheter in place in the right antecubital fossa, there is no blood crossed for this patient. Do you want any preoperative antibiotics?’
Attending surgeon: ‘Preoperative antibiotics are not required in this clean case, thank you. But I just realised that the Mom told me that the patient does indeed have an allergy to amoxicillin. Please confirm’. (error corrected—entire team now knows about the amoxicillin allergy).
Procedure continues as per protocol.
Informed consent by the parents or legal guardian of the patient was obtained. Patients 14 years of age or older were also asked to give their informed written consent for participation.
The only individuals informed about the study were the investigative team, the chief of anaesthesia, as well as the director of operative services of the hospital. All agreed to observe absolute secrecy until study completion.
The study was registered online (https://researchregistry.com, study number 2890).
Statistics
From empirical evidence in our department, we assumed an error detection rate of over 90%. Our null hypothesis was that less than 90% of errors would be discovered. Sample size was therefore calculated so that the lower end of the 95% Pearson CI attained 90%. Actual error detection rate was estimated at 95% of errors. Clopper-Pearson CIs were calculated for the detection rate. A prehoc analysis according to these presumptions calculated a minimum of 120 errors necessary for adequate statistical power. Detection rates were compared using the test of equal or given proportions. Post hoc paired comparisons were calculated using the Benjamini-Hochberg procedure for multiple tests. The comparisons between team member roles were performed as a post hoc analysis.
Results
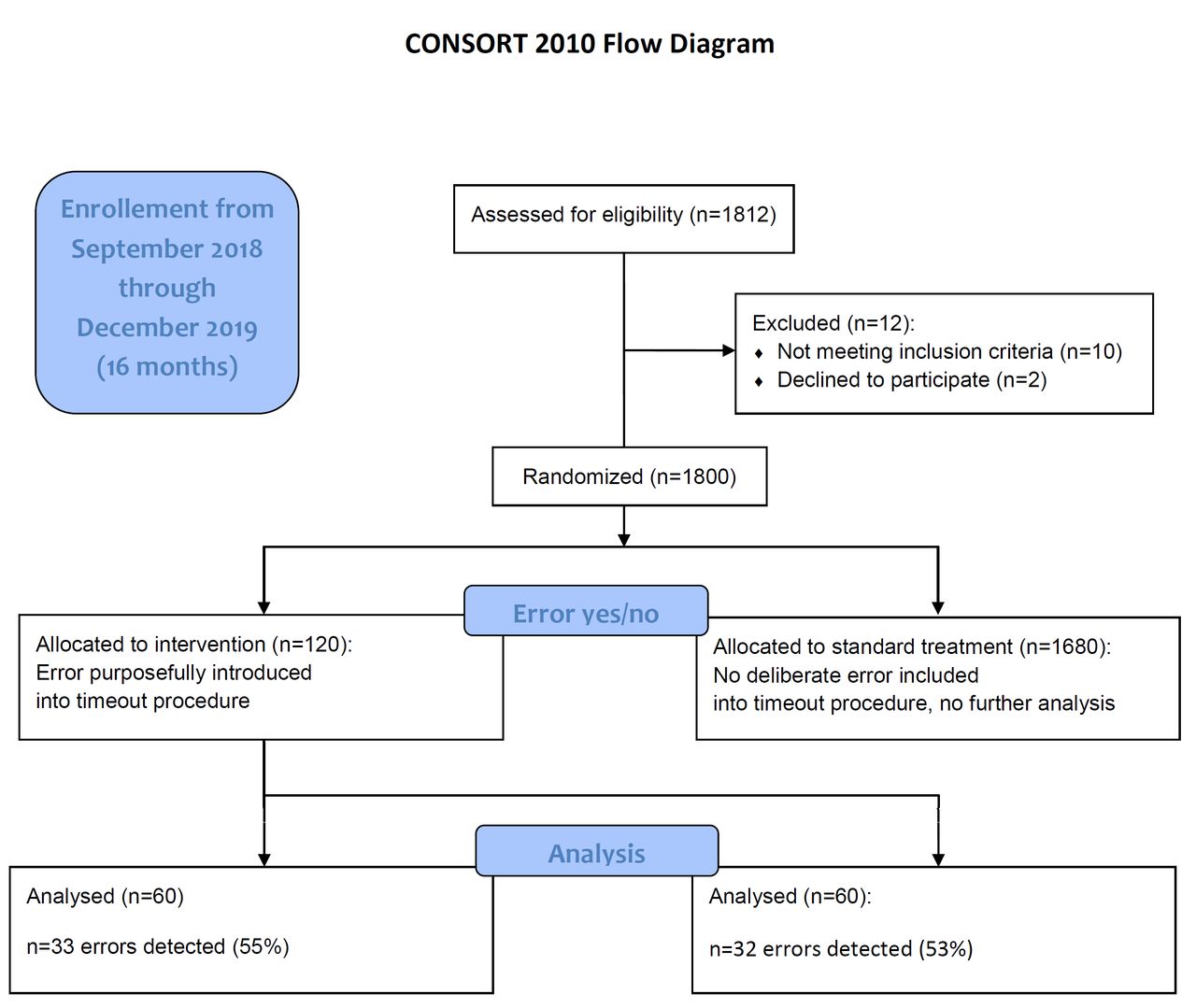
Over the course of 16 months, a total of 1800 operations and timeouts were performed. Errors were randomly introduced in 120 of these cases (6.7%). In the 120 observed cases, in which errors were introduced, compliance with all elements of the timeout procedure was 100%. There were no instances in which a team member falsely corrected an unwarranted item. Also, no real, actual undetected errors were recorded during the study.
Overall, 54% of the errors were verbally challenged; the remainder went unnoticed. The total detection rate was 65 out of a total of 120 errors (54%; see CONSORT flowchart in figure 1). The detailed detection rates by types of error are found in table 1.
Error detection rates by type of error

CONSORT 2010 flowchart of the study participants. CONSORT, Consolidated Standards of Reporting Trials.
The operative team was much more likely to identify a wrong gender mistake at a rate of 77% (95% CI 58% to 90%), compared with wrong age at a rate of 30% (95% CI 15% to 49%) (p<0.001).
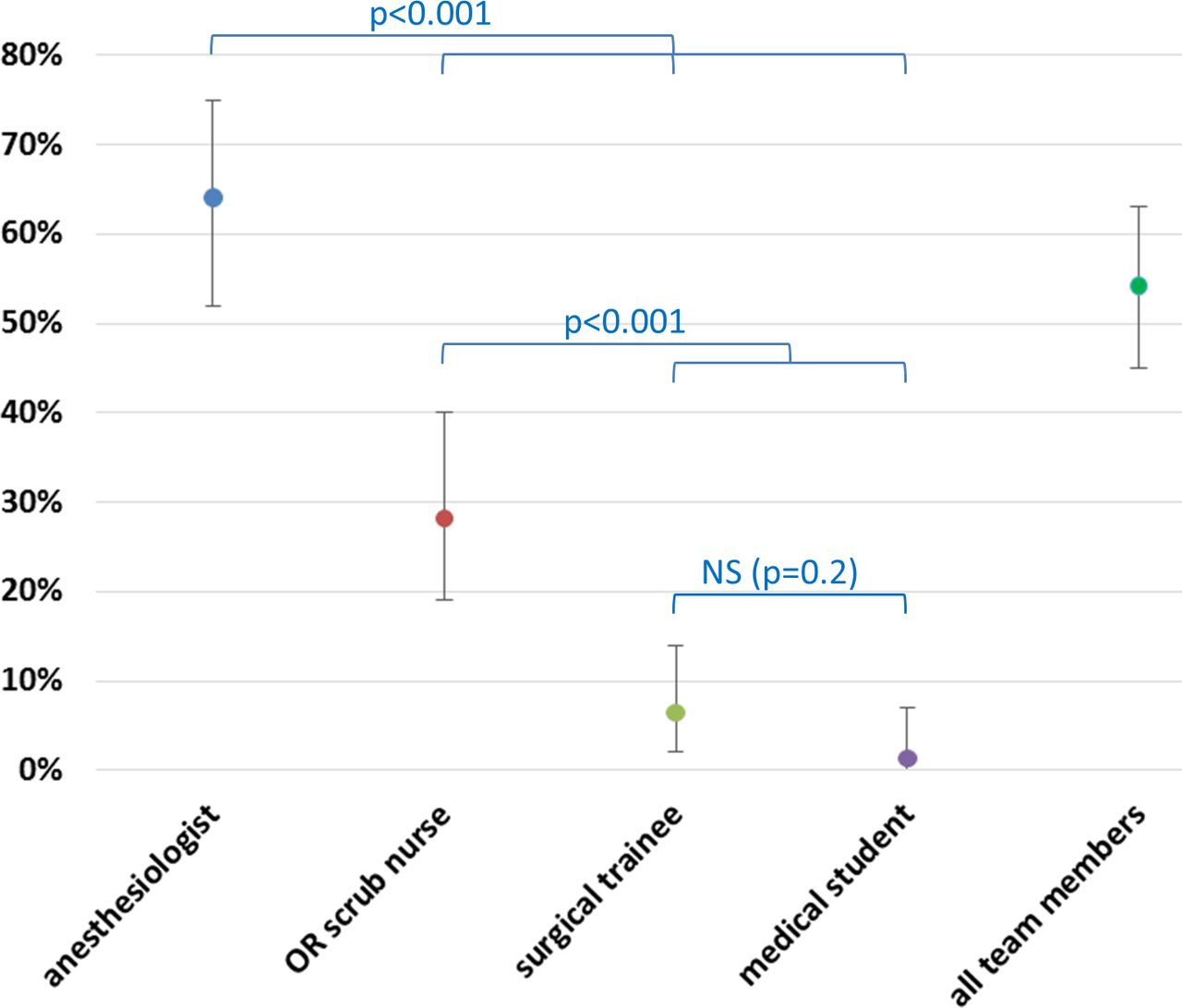
Detection rates and their differences by profession or team function are graphically presented in figure 2. Errors were reported most frequently by an anaesthesiologists (64%), followed by nursing staff (28%), surgical residents or fellows in training (6%) and medical students (1%).
{kind=link}
{kind=link}
Error detection rates by profession/function in the operating team. Error bars represent 95% CIs. NS, not significant.
Discussion
In this first experimental field study, we assessed the surgical team’s detection of randomly planted errors during the timeout procedure. Particularly its undercover design allowed us to obtain more accurate information on how effective a timeout procedure truly is to pick up potentially hazardous errors.
There may be several putative factors decreasing the efficacy of surgical safety checklists. Stress and hastiness in the operating room may lead to omission of important data points. On the other hand, the timeout may be perceived as yet another bureaucratic burden imposed on busy clinicians by the hospital administration, rather than a helpful tool to bring the entire surgical team together onto one page at the beginning of the procedure. Inattentiveness may be another factor that compromises the timeout. Before an operation, there are many issues to tackle, distracting individual team members, and keeping them from listening carefully. The surgical checklist timeout may thereby become a routine litany that is passively endured rather than actively participated in. Trainees, in particular, may not realise the importance of the timeout procedure, either because they have not been instructed appropriately or because they are overwhelmed by other aspects of the operating room environment.
In our study, anaesthesiologists were much more likely than any other team members to point out errors. Perhaps this is due to the relevance of their role in patient management, in which items such as age, weight and allergies are important. The higher detection rates may be related to anaesthesia’s active role in the procedure itself. In our hospital, as in most institutions, both the anasthesiologist and the scrub nurse are required to actively verbalise certain parts of the checklist. Other reasons for higher anaesthesiologist challenge rates may include their independence from surgical and other hospital workflow, as well as pertaining to a specialty that has a long history of patient safety recognition, training and culture.14
In our study, hierarchy appears to have affected detection rates. Trainees and students called out errors less often than attending anaesthesiologists or professionally experienced scrub nurses. Hierarchy may therefore play an important role in how likely a team member interjects when they notice a mistake. Modern safety culture and crew resource management calls for flat hierarchies to allow any member to verbalise discrepancies and potential hazards without fear of repercussion.15 There is appreciable evidence that lower hierarchy members of the surgical team (eg, trainees and junior nurses) are less likely to speak up about safety concerns.16 In a simulation study, more senior anaesthesia trainees were more likely to challenge their attending’s decisions.17 Others have shown negative hierarchical influence on the interactions and communication in a high-fidelity simulated operating room environment.18
The higher detection rates of gender versus age may point to a baseline general attentiveness within the team that makes members react to obvious but not to subtle discrepancies. Also, reporting gender errors may be less risky for low hierarchy team members.
The major weakness of this study is the single centre design, which by nature can only describe our own local situation and circumstances. Other paediatric surgery teams may perform differently
The experimental design of the study focused on the cases with deliberate errors; it did not assess how many possible non-deliberate errors occurred in the rest of the cases during the observational period, how many of these were reported or how they were dealt with.
Compliance with the standardised timeout procedure in the other cases not performed by the investigators is also unknown, since this was not the focus of the study. The study assessed only the physician’s portion of the timeout, not the nursing part.
Another limitation is the early correction of verbalised errors by the attending at the end of the physician’s portion of the timeout procedure. Giving the team more time to correct an error may have increased the correction rates. However, the particular timing used in our study was a requirement set forth by the ethics committee to make sure that the risk of adverse consequences is minimised.
Unfortunately, the study design did not allow us to tease out the reasons for why an error was missed. We did not query the team members why they failed to point out an error. Future studies should survey the participants about inattentiveness, intimidation due to hierarchy or other reasons.
This study does not answer questions on the clinical relevance of missed errors. While some errors, such as a minimal age discrepancy, may be trivial, others can pose a considerable risk to the patient. Still others depend on clinical context.
The question remains how to improve timeout error detection rates. In a prospective field study, at least one member of the operating room team was actively distracted in more than 1 out of 10 procedures observed.19 Similar deficiencies were recorded in a clandestine study in which medical students observed and recorded the timeout procedure in a large academic medical centre.20 In our opinion, attentiveness may perhaps be effectively facilitated by requiring interactive participation in the timeout by everybody in the room, including trainees and students. Although team members should regard themselves as a valuable part of the timeout safety check, systems safety science acknowledges that general imperatives such as ‘try harder’ and ‘pay more attention’ are very unlikely to be successful. Changing a deeply seated cultural hierarchy requires a multimodal, long-term approach.
Checklists are one of the fields that lend themselves to computerised assistance. Modern data processing equipment could enhance the timeout procedure by providing an interactive, voice-controlled platform in which the team members sign in and then verbalise the items of a structured timeout procedure after being prompted. The system itself could check for plausibility according to the data in the electronic medical record, and at the same time verify issues such as patient weight, allergies or relevant medications. It may also be programmed to check for completeness, for example, whether all items and datapoints were mentioned.
Finally, artificial intelligence combined with camera technology and motion detection could make sure that the patient is positively identified, and that the surgery is performed on the correct side or site. Future developments such as interactive, voice-activated platforms, computer-assisted timeout protocols, automatic patient identification, facial recognition and the use of artificial intelligence may potentially be useful to improve and enhance the quality of the surgical timeout procedure. Interventions to increase error reporting rates should be prospectively assessed in the future and benefits should be weighed against their costs.
Conclusions
In summary, almost half of deliberately sown errors in the timeout routine were not reported by the team in this experimental field study. A wide variety of errors in the surgical timeout procedure were often not recognised. Therefore, even when compliance with the timeout procedure is 100%, this does not necessarily translate to safer care, given that many errors go unreported. The checklist can easily become a passive exercise, rather than an active safety tool. This may explain why the introduction of surgical safety checklists has had mixed impact on avoidance of errors in surgery. Factors associated with these findings may be inattentiveness, non-participation, false sense of hierarchical inferiority, or situational stress. This study indicates that the standard, structured verbal timeout procedure in its current form does not provide comprehensive protection from medical errors. Additional research is needed, including evaluation of the potential benefits of advanced technology.
Data availability statement
The anonymised, non-identifiable data this study is based on are available upon request. Requests should be directed to the corresponding author. Reuse is permitted for scientific purposes and quality initiatives.
Ethics statements
Ethics approval
This study was approved by the ethics comittee of the state of Rhineland-Palatinate (approval number 837.105.17/10939, 2017). A particular request of the ethics board was that errors be corrected during the timeout procedure for safety reasons.
References
Footnotes
Contributors OJM: conception of study, participation in the timeout procedures, data interpretation, drafting of the manuscript. JG: participation in the timeout procedures, data interpretation and review of the manuscript. Mentorship to HK: randomisation, monitoring in the operating room, recording of data, analysis and review of the manuscript. AP: statistical design and analysis, review of manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.