Article Text

Abstract
Background Studies carried out in simulated environments suggest that checklists improve the management of surgical and intensive care crises. Whether checklists improve the management of medical crises simulated in actual emergency departments (EDs) is unknown.
Methods Eight crises (anaphylactic shock, life-threatening asthma exacerbation, haemorrhagic shock from upper gastrointestinal bleeding, septic shock, calcium channel blocker poisoning, tricyclic antidepressant poisoning, status epilepticus, increased intracranial pressure) were simulated twice (once with and once without checklist access) in each of four EDs—of which two belong to an academic centre—and managed by resuscitation teams during their clinical shifts. A checklist for each crisis listing emergency interventions was derived from current authoritative sources. Checklists were displayed on a screen visible to all team members. Crisis and checklist access were allocated according to permuted block randomisation. No team member managed the same crisis more than once. The primary outcome measure was the percentage of indicated emergency interventions performed.
Results A total of 138 participants composing 41 resuscitation teams performed 76 simulations (38 with and 38 without checklist access) including 631 interventions. Median percentage of interventions performed was 38.8% (95% CI 35% to 46%) without checklist access and 85.7% (95% CI 80% to 88%) with checklist access (p=7.5×10−8). The benefit of checklist access was similar in the four EDs and independent of senior physician and senior nurse experience, type of crisis and use of usual cognitive aids. On a Likert scale of 1–6, most participants agreed (gave a score of 5 or 6) with the statement ‘I would use the checklist if I got a similar case in reality’.
Conclusion In this multi-institution study, checklists markedly improved local resuscitation teams’ management of medical crises simulated in situ, and most personnel reported that they would use the checklists if they had a similar case in reality.
- checklists
- crisis management
- simulation
- team training
Data availability statement
Data are available in a public, open access repository. All data relevant to the study are included in the article or uploaded as supplementary information. The data collected for this study and the programs that analysed these data are publicly available. The data for this study are posted at https://www.dropbox.com/sh/u1xfkz2s7fyjxsc/AAD3l3ZL1mHqoeRkNDkTCKr0a?dl=0inanExcelspreadsheetnamedChecklists_ED_interventions.xlsx. It is freely available to anyone. To make a copy of this file, go to this URL, pull down the Open box next to Checklists_ED_interventions.xlsx and select 'Open in Excel'.
Statistics from Altmetric.com
Introduction
Roughly 15% of patients presenting to the emergency department (ED) require immediate or urgent interventions to decrease morbidity and mortality.1 2 Anaphylaxis is an example of a medical crisis where fatal outcomes are associated with delayed treatment with epinephrine.3 4 A minority of medical crises do not respond to first-line treatment, and more complex therapies are required. For example, 0.4% of patients with anaphylaxis are refractory to intramuscular epinephrine, and these cases are associated with a mortality of 26%.5 Managing such medical crises is challenging given their high acuity, low frequency and increased complexity.
Checklists are cognitive aids that outline assessments or actions and that are designed to be carried out systematically. Cognitive aids such as checklists may help teams manage unusually severe medical crises by palliating for the unfamiliarity and stressful nature of the situation.6–8 Given the low-frequency and high-acuity nature of crises, simulation-based trials have been used to study the impact of checklists on crisis management. One study reported that access to surgical crisis checklists decreased the rate of missed life-saving processes of care in the operating theatre from 23% to 6%.9 Another study reported that access to checklists for emergency procedures improved the completion of critical treatment steps in the intensive care unit.10 The aim of this randomised controlled simulation-based trial was to evaluate the impact of checklists on the management of medical crises by local resuscitation teams during their clinical shifts using simulations carried out in the ED.
Methods
Crises
Eight crises were selected for the study: anaphylactic shock, life-threatening asthma exacerbation, haemorrhagic shock from upper gastrointestinal bleeding, septic shock, calcium channel blocker poisoning, tricyclic antidepressant poisoning, status epilepticus and increased intracranial pressure. Each of these potentially fatal conditions is an emergency in which patients can fail to respond to initial measures and for which there are established non-first-line therapies.
Checklists
A checklist was developed for each crisis through an iterative process involving specialists and residents in emergency medicine and senior nurses working in the ED. Checklist format and design was informed by the literature pertaining to emergency and abnormal checklists in the aviation industry11–13 and by articles on medical checklists.8 14 15 Each checklist outlined interventions to consider during the management of the crisis, based on current authoritative sources and consensus from four specialists in emergency medicine. Each intervention was associated with a popover window displaying indications, contraindications and risks, and for each medication, the medication name(s), location, dose, route and rate of administration. The checklists were customised to display the commonly used names and the locations of medications for each ED where the study was carried out (figure 1; online supplemental appendix 1 Sections I–II). The checklists were not disseminated in the EDs prior to the study.
Supplemental material

Sample checklist and popover window.
Scenarios
Scenarios were developed for each of the eight medical crises based on actual cases that had presented to one of the EDs. The nature of the medical crisis was readily apparent from the scenario introduction read out prior to each simulation and the clinical findings provided during the primary survey. For example, teams were informed that the patient had vomited a mixture of fresh blood and coffee grounds throughout the night prior to the upper gastrointestinal haemorrhage scenario (online supplemental appendix 1 Section III). For each scenario, 7–10 emergency interventions were identified as indicated (online supplemental appendix 1 Section III).
Study sites
Sample size calculations based on results from a pilot study16 indicated that performing each scenario twice (with and without checklist access) in three EDs would be sufficient to detect a clinically meaningful difference of 20% in performed emergency interventions with a power of 0.80 and a type I error probability of 0.05 (online supplemental appendix 1 Section IV). Since the feasibility of performing simulations in situ in busy resuscitation rooms was unclear, we aimed to perform the study in four EDs. These EDs cater primarily to adult patients, with a yearly number of patient visits of 85 000, 80 000, 65 000 and 35 000. Two of these EDs belong to an academic centre (a tertiary care university hospital), one to a large community hospital and one to a rural community hospital.
Study participants
Study participants consisted of the medical personnel on clinical duty composing a resuscitation team assigned to manage priority 1 patients. In two of the EDs, an additional resuscitation team was scheduled to work during the mornings of the study week to ensure that both teams could partake in the simulations without having to manage actual priority 1 patients. Study participants were not informed in advance of the nature of the scenarios.
Allocation to scenario and checklist access
The sequence according to which the eight scenarios were carried out at each ED was predetermined through permuted block randomisation. Whether the first simulation in each ED was run with checklist access (+) or without (−) was alternated between EDs. Checklist access was alternated thereafter within each ED. For example, if the randomly generated scenario sequence was 53284617 and the first scenario was run with checklist access, the following sequence was generated: 5+, 5−, 3+, 3−, 2+, 2−, 8+, 8−, 4+, 4−, 6+, 6−, 1+, 1−, 7+, 7−. This sequence can be thought of as a stack of 16 cards, with the top card representing scenario 5 with checklist access and the bottom card scenario 7 without checklist access.
For a given team, the allocated scenario was the highest card in the stack representing a scenario that none of the team members had performed previously. This feature ensured that no participant performed the same scenario more than once. Once a team had successfully carried out a whole simulation, the corresponding card was discarded. When a given team could perform a second simulation, the allocated scenario was the highest card in the stack representing a scenario that none of the team members had performed previously and with a different checklist access than during the first simulation. This feature ensured that teams that could perform two scenarios performed one with and one without checklist access. If the team had to interrupt the scenario prior to its completion, the card was left in the stack at its original position, until a team consisting of different personnel could perform the scenario, and the incomplete simulation was excluded from the study.
Simulations
All simulations were run between 08:00 and 11:00 when the lead nurse and physician in the ED deemed that the timing was suitable. The lead nurse and physician in the ED had the mandate to interrupt the study at any time to ensure patient safety in the ED. The resuscitation team was gathered in the resuscitation room, team members were enrolled in the study and signed an informed consent form, and scenario and checklist access was determined as described above. Personnel were instructed to locate actual equipment and medications during the simulations in order to receive training equipment and clearly marked placebo medications, and instructed to treat the manikin as they would a real patient. All teams were informed that the diagnosis would be readily apparent from the scenario introduction and that the simulations would focus on treatment (online supplemental appendix 1 Section IV). Personnel were explicitly allowed to use their usual cognitive aids (eg, pocketbooks, internet) but not allowed to request help from other personnel during the simulation.
Simulations were performed using an adult manikin (Laerdal Extri Kelly) that could quickly be wheeled out of the resuscitation room if necessary. Computer-generated vital signs were displayed on the screen used during actual clinical practice or on a screen of similar size placed in a similar location. All simulations were video recorded using two cameras. Simulations were terminated when all indicated emergency interventions had been performed, when the team expressed that they could not think of any other intervention to perform or when 15 min has elapsed, whichever came first.
Each scenario was simulated at least twice, once with and once without checklist access, in each of the four EDs. Each team performed two separate scenarios, one with and one without checklist access, unless precluded by actual emergencies. Simulations that had to be interrupted were repeated with a team consisting of other personnel. No personnel participated in a given scenario more than once. In one ED, all 16 scenarios were performed over the course of 3 weeks. In the other three EDs, all scenarios were performed during five consecutive weekdays, with a target of four simulations per day and the possibility of performing additional simulations on the fifth day.
Checklist display
The checklists were stored on a tablet computer. The tablet computer was connected to a screen large enough to be seen by all team members during the simulation (online supplemental figure 1). Two of the four resuscitation rooms were equipped with large wall-mounted screens that are routinely used to display information to the whole team, and the checklists were displayed on these screens. In the other two resuscitation rooms, the checklists were displayed on a large television mounted on a trolley. When teams were allocated to checklist access, a demonstration checklist was presented to the team prior to simulation, and the nurse or medical secretary assigned the task of managing the checklist familiarised himself or herself with the popover window function. The investigator running the simulation selected the relevant checklist once the simulation had begun. The investigator was not allowed to encourage personnel to use the checklist during the simulation. Personnel who had run a simulation with checklist access were subsequently asked to fill out a survey evaluating the checklist.
Statistical analysis
Video recordings of all scenarios were independently reviewed by two emergency physicians. In addition, a random sample of two scenarios with, and two without, checklist access from each site was reviewed by an outside emergency physician unaware of the study hypothesis. Reviewers independently recorded whether the predefined indicated emergency interventions were performed on the manikin (as opposed to just ordered) using a yes/no coding, and when these interventions were performed. The primary outcome measure was the percentage of interventions carried out by the team within 15 min from simulation start. The order according to which interventions were performed did not impact on the primary outcome measure. In our primary analysis we used bootstrapping to determine how the median percentage of interventions performed varied between teams that did, or did not, use checklists.17 In a secondary analysis using a mixed-effects ordinal logistic regression model,18 we assessed how the number of interventions performed varied among teams that did, and did not, use checklists. This model included random intercepts for EDs, and teams nested within EDs, in order to determine whether the effect of checklist access on number of interventions performed varied between teams or between EDs. The importance of these random effects was assessed by the magnitude of their SEs when the model’s likelihood function was maximised and by a likelihood ratio test. Using similar models, we separately regressed the number of interventions against senior physician’s experience, whether the senior physician was a specialist, senior nurse’s experience and scenario type. To explore whether these variables and the use of local cognitive aids acted as effect modifiers, we also ran models that included checklist access, the variable of interest and the interaction between checklist access and the variable of interest. For example, for the specialist status of the senior physician, we regressed number of interventions against checklist access, specialist status and an interaction term obtained from the product of the checklist indicator and the specialist status indicator.
Cohen’s kappa was used to assess agreement between the two physicians who reviewed each of the simulations. After resolution of discrepancies, Cohen’s kappa was used to assess agreement with the outside reviewer. All reported p values are two sided. Data were analysed with Stata Release V.16 (College Station, Texas: StataCorp). The data from this study are provided open source, and the codes that analysed the data and created the figures are provided in online supplemental appendix 2.
Results
Characteristics of the participants
A total of 31 physicians, 54 nurses, 37 nursing assistants and 16 medical secretaries composing 41 resuscitation teams participated in the study; 25 of the 31 physicians were residents (table 1). In two EDs, the standard team consisted of one physician, one nurse, one nursing assistant and one medical secretary (18 teams), but in two teams a nurse replaced the nursing assistant. In the other two EDs, the standard team consisted of one physician, two nurses and one nursing assistant (13 teams); three teams included an additional physician, three teams an additional nursing assistant, one team an additional nurse and in one team a nurse replaced the nursing assistant (online supplemental table 5). Of the 138 participants, 114 participated in one or two scenarios, 19 in three or four scenarios and 5 in five or six scenarios (online supplemental table 6).
Professional characteristics of the participants
Simulations performed and use of cognitive aids
All eight scenarios were performed twice (once with and once without checklist access) in each of the four EDs. In each of the three EDs, it was possible to perform an additional four simulations, resulting in a total of 76 simulations including a total of 631 indicated emergency interventions. Thirty-five of the 41 teams performed two simulations, one with and one without checklist access. Six teams performed only one simulation (three with and three without checklist access). The three teams that only performed one scenario with checklist access did not differ significantly from the three teams that only performed one scenario without checklist access in regard to team size, physician and senior nurse age and experience. One simulation (upper gastrointestinal bleeding without checklist access) had to be interrupted due to an actual emergency; the scenario was subsequently rerun with another team. Scenarios were terminated because all interventions had been performed in 14 simulations with checklist access and none without; because of no further ideas in 4 simulations with checklist access and 12 without; because 15 min had elapsed in 20 scenarios with checklist access and 26 without (online supplemental table 8). There was no significant difference between the simulation durations with or without checklist access (p=0.12) (online supplemental table 9). In all but 3 of the 76 simulations, physicians had ordered diagnostic-specific first-line interventions, and when simulations were terminated at 15 min, teams were dealing with non-first-line interventions. Usual cognitive aids were used to guide treatment during 26 simulations without checklist access and in six simulations with checklist access (online supplemental table 11). In all 38 simulations without checklist access, the physician provided proof of diagnostic awareness by either stating the diagnosis or ordering diagnosis-specific interventions (online supplemental table 16).
Impact of checklist access
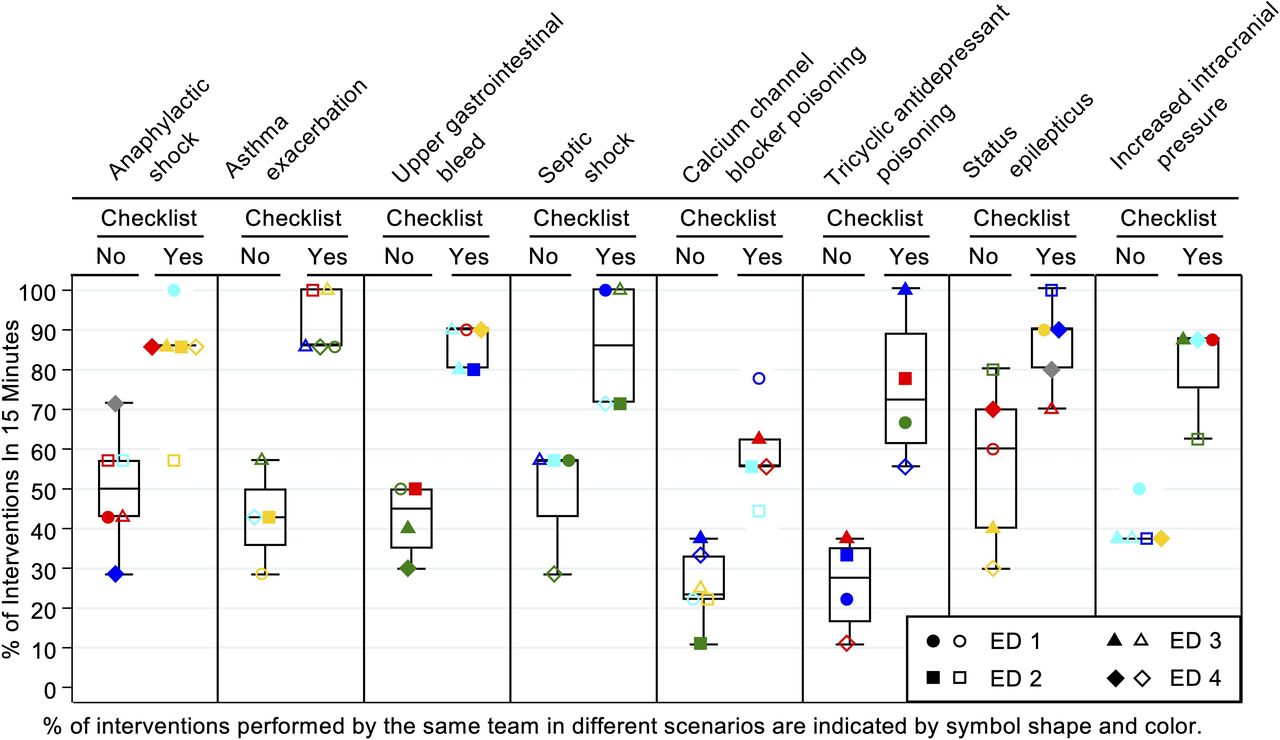
The median percentage of interventions performed was 38.8% (95% CI 33% to 44%) without checklist access and 85.7% (95% CI 80% to 88%) with checklist access (p=7.5×10−8). There was a marked difference in the distribution of interventions performed by teams with and without checklist access (figure 2 and online supplemental table 12). The number of interventions performed was unaffected by ED, team, senior physician experience, whether she/he was a specialist and senior nurse experience (online supplemental table 13). There was no evidence that any of these variables acted as effect modifiers to the relationship between checklist access and number of interventions performed (online supplemental table 14). Nor was there any evidence that scenario type (p=0.27) or use of cognitive aids (p=0.72) modified the impact of checklist access on number of interventions performed (online supplemental table 14).

Percentages of performed indicated emergency interventions. ED, emergency department.
Figure 3 shows the effect of checklists on median percentage of interventions performed as a function of time. Checklist access did not impede the performance of initial interventions. Table 2 provides examples of how checklist access impacted on the performance of specific interventions. Dangerous or inappropriate interventions occurred in 15 instances, of which 14 were during simulations performed without checklist access (online supplemental table 15).

{kind=link}
{kind=link}
{kind=link}
Median percentage of emergency interventions performed by teams with and without checklist access throughout the simulation.
Impact of checklist access on specific interventions
Inter-rater agreement
Each simulation was independently reviewed by two investigators. The inter-rater agreement with respect to emergency interventions performed was high (kappa=0.92, 95% CI 0.89 to 0.95). Initial disagreement was easily resolved given that the interventions were hard endpoints. For the 16 simulations randomly selected for review by an outside physician, the inter-rater reliability with respect to interventions performed was also high (kappa=0.89, 95% CI 0.81 to 0.97).
Survey responses
On a Likert scale of 1–6, 94% of all participants agreed (ie, gave a score of 5 or 6) with the statement ‘I would use the checklists if I got a similar case in reality’. Profession and scenario had no substantial effect on the responses to the survey (online supplemental tables 18–20).
Discussion
This study found that checklist access was associated with an increase from 39% to 86% in the median percentage of indicated emergency interventions performed by teams managing simulated medical crises. There was no evidence that checklist use delayed the initial performance of emergency measures. Most participants indicated that they would use the checklist if they had a similar case in reality.
It may seem tautological to randomise teams to checklist access and evaluate performance based on completion of items featuring on the checklist. Yet, given that crises are by nature rare, unexpected, high-stakes events, it is logistically and ethically problematic to evaluate, in a clinical study, an intervention designed to facilitate the provision of currently recommended emergency interventions using as outcome measures morbidity and mortality. Simulation is specifically advantageous as research modality for studying rare events where experimentation may not be appropriate for ethical reasons, and for evaluating interventions that seek to improve care.19 In this simulation-based study, the outcome measure was the performance of indicated emergency interventions based on current authoritative sources. The study results could have suggested that checklist access does not impact on emergency intervention performance, either because the checklists are unnecessary or because they do not adequately address the actual challenges of medical crisis management. Instead, the study results suggest that carefully designed, up-to-date, customised team checklists may promote the delivery of indicated emergency interventions during an actual medical crisis in the ED.
Two studies performed in simulated environments have reported a benefit of crisis checklists: one found that access to 10 surgical crisis checklists increased the rate of life-saving processes performed in the operating theatre from 77% to 94%,9 while another reported that access to checklists for emergency procedures increased the median number of key items performed from 7 to 9.10 The current study found a more dramatic effect of checklist access on performance, presumably due to the complexity of the second-line and third-line therapies for the selected crises.
In comparison to these previous studies, the current study evaluated checklists through simulations carried out by actual resuscitation teams, during their clinical shifts, in their own resuscitation rooms, with access to their usual cognitive aids and having to locate their own equipment and medications. Healthcare delivery is dependent on the attributes of healthcare personnel, the tools and technology at their disposal, the physical and organisational environment they work in and interactions between these factors.20 The results of in situ studies may better approximate the effectiveness of a new tool than those obtained in simulated environments with volunteers deprived of their usual cognitive aids.
The study results may be less generalisable to EDs with different resuscitation team member characteristics, tools and support at their disposal. In the present study, the majority of physicians were residents, and resuscitation teams were not allowed to call other personnel for assistance. The benefit of checklist access may be diminished if the physicians were specialists, yet no association was found between physician experience and team performance in this study. Given that medical crises seldom occur, it is plausible that specialists would also benefit from cognitive aids. Furthermore, stress affects the performance of even seasoned professionals.21–24 Some recommend that critical event checklists be geared to the level of the most junior physician expected to practise independently.15
This study focused on the management of crises where the diagnosis was clear from the outset. In practice, establishing the most likely cause of the patient’s symptoms is not always clear-cut. Yet, even when diagnostic uncertainty is present, acute management is based on presumptive diagnosis. The relevant checklist was provided directly to the team at the outset of the simulation, in order to avoid displaying the main menu featuring all eight study crises, given the possibility that some team members would perform additional simulations on a later day. The study therefore did not evaluate personnel’s ability to navigate among a collection of checklists.
It may be hypothesised that teams with checklist access benefited from knowing the diagnosis from the start, while teams without checklist access suffered from diagnostic uncertainty. Yet the diagnosis was readily apparent from the scenario introduction provided, video recordings provide proof of diagnostic awareness in all 38 simulations without checklist access and potential delay in diagnostic awareness cannot account for underperformance of teams without checklist access (online supplemental appendix 1 Section VIII).
When faced with a medical crisis in the ED, personnel need to know the indications for potential interventions, be able to locate relevant equipment or medications and deliver specific therapies and feel authorised to do so. Failure at any of these steps results in the intervention not being carried out. Medical crises unresponsive to first-line therapies are especially challenging given that their management may require the administration of unfamiliar medications under time pressure, each with specific generic and commercial names, dosages, routes and rates of administration. Checklists augment memory and attention25 and presumably improved team performance during simulated complex medical crises by compensating for the unfamiliarity and stressful nature of the situation.6–8
The quality of teamwork in emergency medicine and during resuscitation has been linked to patient safety,26 27 and the crisis resource management paradigm emphasises the centrality of customised team-based tools when managing complex high-risk situations.28 The checklists evaluated in this study were displayed to all team members on large screens, contributing to a shared awareness of the severity of the situation, promoting a joint involvement in patient management and implicitly endorsing the delivery of indicated interventions. Displaying the checklist to the whole team may have encouraged crosschecking, a practice which has been shown to improve performance.29 30 Assigning the task of systematically implementing the checklist to a nurse, as is the case for the Time Out section of the WHO Surgical Safety Checklist,31 or to a medical secretary, may also have contributed to effective checklist use.32
It is unrealistic to expect healthcare personnel to keep up to date with non-first-line therapies for all potential medical crises that may present to an ED, where the medications are located, their generic and commercial names, their dosages and modes of administration. Cognitive aids such as pocketbooks and resources accessible through the internet may palliate for knowledge gaps, but they are not necessarily up to date and they may cause confusion when they recommend medications that are not available or are referred to by a different name. They often lack practical information such as where to find the medication, whether it needs to be diluted and its administration rate. Two-thirds of teams without checklist access used their usual cognitive aids, but this use did not significantly mitigate the benefit of checklist access. There is currently no standard framework for the development and design of medical checklists,14 15 nor any requirements for their availability and use. Customised team checklists such as those used in this study may provide an updatable platform to translate best practices for patient care during acute events.6
This study suggests that carefully designed, customised checklists visible to the whole resuscitation team may significantly improve the management of complex medical crises. An interview-based study of emergency manual use during perioperative crises reported positive impacts on patient care delivery and teamwork, and no impediments.33 Integrating checklist use in clinical practice is contingent on an implementation process that addresses why, how, when and by whom the checklist is intended to be used, and routines to update and improve the checklists.15 31 Future research evaluating, during actual clinical practice, a large collection of checklists addressing the most common diagnostic and treatment processes encountered in the resuscitation room is warranted.
Figure 1 displays the checklist for asthma exacerbation. The backbone features seven interventions. Each intervention is associated with a popover icon (a white plus sign within a red dot); pushing on the popover icon brings forth a popover window. The illustration shows the content of the popover window for the intervention ‘5. Magnesium?’. The seventh intervention (Betapred) was not considered an emergency intervention within the context of the study (online supplemental appendix 1 Emergency Intervention Criteria).
These combined scatter and boxplots illustrate the percentages of indicated emergency interventions performed within 15 min for all 76 simulations, according to scenario and checklist access. Each team is represented by a unique colour and symbol combination. The symbol shape represents the ED where the simulation was performed. For example, round symbols denote teams from ED 1. The solid red circles in the anaphylactic shock scenario and the increased intracranial pressure scenario give results obtained by the same team performing without, and with, checklists, respectively. Thirty-five teams performed two simulations each, one with and one without checklist access; six teams performed only one simulation. The figure illustrates the profound effect of the checklist for each scenario. There is no obvious difference between the performance of the different EDs or different teams. Boxplots drawn behind the scatterplots give the 25th, 50th and 75th percentiles of the per cent of indicated interventions performed for each scenario, with and without checklists.
This figure illustrates the median percentage of indicated emergency interventions performed by teams that did, and did not, use the checklist as a function of time since the start of each scenario; 95% CIs for these percentages were derived from 2000 bootstrapped samples.17 The sampling unit for these bootstrapped samples was the team. Since our study design required equal number of teams that used and did not use the checklists, these bootstrapped samples were stratified by checklist usage. Percentil-based confidence bands are displayed in this graph. Checklist access did not impede the initial performance of emergency interventions. After 7 min, checklist teams were performing significantly more interventions than non-checklist teams. As of 10 min into the simulation, virtually no additional interventions were performed in the no-checklist teams while additional interventions were performed throughout the final 5 min by teams with checklist access. This suggests that a longer simulation duration would, if anything, have resulted in an increased impact of checklist access on performance.
This table provides, for each of the eight scenarios, the number of times two emergency interventions were performed given access or not to crisis checklists, along with the total number of times the scenarios were performed.
Supplemental material
Data availability statement
Data are available in a public, open access repository. All data relevant to the study are included in the article or uploaded as supplementary information. The data collected for this study and the programs that analysed these data are publicly available. The data for this study are posted at https://www.dropbox.com/sh/u1xfkz2s7fyjxsc/AAD3l3ZL1mHqoeRkNDkTCKr0a?dl=0inanExcelspreadsheetnamedChecklists_ED_interventions.xlsx. It is freely available to anyone. To make a copy of this file, go to this URL, pull down the Open box next to Checklists_ED_interventions.xlsx and select 'Open in Excel'.
Ethics statements
Ethics approval
The study was approved by Lund’s Regional Ethics Committee (Dnr 2013/858) and the heads of the four emergency departments, and all study participants gave written consent.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors ED is a specialist and educator in emergency medicine. He contributed to the conception of the study, the acquisition, analysis and interpretation of data, drafting and revising the manuscript and approving the current version submitted for publication. JLF and CHS are specialists in emergency medicine and contributed to the acquisition of data, revising the manuscript and approving the current version submitted for publication. WDD is a Professor of Biostatistics and Preventive Medicine and contributed to the analysis and interpretation of data, revising the manuscript and approving the current version submitted for publication. AB is a Professor of Practical Medical Education and contributed to the conception of the study, the interpretation of data, revising the manuscript and approving the current version submitted for publication. UE is a Professor of Emergency Medicine and Associate Professor of Physiology. He contributed to the conception of the study, the analysis and interpretation of data, revising the manuscript and approving the current version submitted for publication.
Funding This study was funded by Region Skåne (ALF 2018-0152, REGSKANE-627931, REGSKANE-814271).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.