Article Text

Abstract
Background Clinical practice guidelines emphasise the role of regular monitoring of glycated haemoglobin A1c (HbA1c) for patients with type 2 diabetes, with most recommending 6-monthly testing. Nonetheless, there are few in-depth studies evaluating the clinical impact of the recommended testing frequency for patients to underpin the significance of guideline adherence.
Objective This study aimed to examine associations between patient outcomes and adherence to HbA1c testing frequencies recommended by Australian guidelines (6-monthly for patients with adequate glycaemic control and 3-monthly for patients with inadequate glycaemic control). The primary and secondary outcomes of interest were longitudinal changes in HbA1c values and development of ischaemic heart disease (IHD) and chronic kidney disease (CKD).
Methods This 5-year retrospective cohort study (July 2013–June 2018) evaluated HbA1c testing frequency in a subset of patients with type 2 diabetes identified within data collected from approximately 250 Australian general practices. The study included patients who were aged ≥18 in 2013 and had a record of HbA1c testing in study practices during the study period. Each patient’s adherence rate was defined by the proportion of HbA1c tests performed within the testing intervals recommended by Australian guidelines. Based on the adherence rate, adherence level was categorised into low (≤33%), moderate (34%–66%) and high (>66%). Generalised additive mixed models were used to examine associations between adherence to the recommended HbA1c testing frequency and patient outcomes.
Results In the 6424 patients with diabetes, the overall median HbA1c testing frequency was 1.6 tests per year with an adherence rate of 50%. The estimated HbA1c levels among patients with low adherence gradually increased or remained inadequately controlled, while HbA1c values in patients with high adherence remained controlled or improved over time. The risk of developing CKD for patients with high adherence was significantly lower than for patients with low adherence (OR: 0.42, 95% CI 0.18 to 0.99). No association between IHD and adherence to the recommended HbA1c frequency was observed.
Conclusion Better adherence to guideline-recommended HbA1c testing frequency was associated with better glycaemic control and lower risk of CKD. These findings may provide valuable evidence to support the use of clinical guidelines for better patient outcomes in patients with type 2 diabetes.
- diabetes mellitus
- clinical practice guidelines
- chronic disease management
- general practice
- compliance
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Diabetes mellitus, commonly known as diabetes, is a metabolic disease that results in high blood glucose levels and affects 1 in 10 adults in high-income countries.1 Type 2 diabetes is the most common form of diabetes, accounting for approximately 90% of diabetes cases worldwide.2 Type 2 diabetes is a long-term condition requiring regular follow-up and often lifelong pharmacological treatment after diagnosis. Poor diabetes management can contribute to serious complications, which can be microvascular (eg, nephropathy, neuropathy, retinopathy) or macrovascular (eg, cardiovascular disease, stroke) complications.3 These subsequent complications may have significant impact on patient well-being and quality of life, with major healthcare cost implications.4
Patients with type 2 diabetes receive regular blood sugar monitoring to assess progression and risk for complications. These tests include blood glucose tests as an acute short-term indicator; however, since these can fluctuate hourly, the more stable glycated haemoglobin A1c (HbA1c) test is used as an indicator of longer term glycaemic control. HbA1c in blood reflects the average blood glucose level over the preceding 8–12 weeks.5 Hence, HbA1c testing is widely considered as the gold standard for monitoring and treatment of type 2 diabetes.6 Current national and international guidelines across many developed countries including Europe (ie, UK, Belgium, France, Germany, Italy, The Netherlands, Sweden),7 8 USA9 and Australia10 also highlight the importance of HbA1c monitoring in type 2 diabetes management, with the recommendation that it be tested at least every 6 months in patients with stable glycaemic control.
Despite the importance of HbA1c testing in diabetes care management, there is a lack of evidence underpinning the importance of adherence to guideline-recommended testing frequencies for patient outcomes. The results from existing literature are currently limited to descriptive studies based on a short observation period (eg, 1 year)11 12 and highly selective populations (eg, a sample from one tertiary hospital11 13 or a private health insurance provider).12 Thus, it remains unclear how adherence to the guidelines impacts on the course of disease progression in the long term among the general type 2 diabetes population. There is a clear need to better understand this relationship, using comprehensive and rigorous evaluations on adherence to HbA1c.
In Australia, general practitioners (GPs) play a central role in type 2 diabetes care,14 and access to public healthcare including visits to GPs and pathology testing is generally covered by universal health insurance. A recent study using Australian general practice data has demonstrated the value of electronic data to evaluate the quality of care and patient outcomes in a sample population approximating the Australian diabetes population.15 This population therefore provides a valuable opportunity to undertake a longitudinal cohort study on type 2 diabetes outcomes in general practice.
Our objective was to address the gap in evidence on the impact of HbA1c testing adherence, compared with the guidelines, on patient outcomes in type 2 diabetes. The aim of this study was to evaluate associations between adherence to the guideline-recommended testing frequencies and patient outcomes using a 5-year longitudinal sample collected from approximately 250 Australian general practices. In this study, we examined longitudinal changes in HbA1c values as the primary outcome to observe disease progression over time. The secondary patient outcome was the development of complications such as cardiovascular disease (ischaemic heart disease (IHD)) and chronic kidney disease (CKD). IHD and CKD were observed in this study since they were the most common serious microvascular and macrovascular complications.16 We compared the cumulative risk of complications by adherence to guideline-recommended testing intervals.
Methods
Study period and population
The study period was 5 years, from July 2013 to June 2018. Inclusion criteria for patients included the following: (1) active patients who regularly attended a general practice during the study period—active patients were defined, based on the definition from the Royal Australian College of General Practitioners (RACGP),17 as individuals who had attended the practices three or more times in the past 2 years at the time of visit; (2) individuals aged ≥18 as of 2013 with a diagnosis of type 2 diabetes at least 1 year before the study period (ie, from July 2012 to July 2013); and (3) patients with two or more HbA1c tests during the study period, with at least one performed in the first year of the study period. Patients with a history of IHD and CKD before July 2013 were considered to have possible pre-existing diabetes-related complications and were thus excluded. In Australia, since patients can visit different general practices, there was the potential that some patients could receive diabetes care outside the catchment practices. To minimise such cases, patients who had regular visits to GPs with records of HbA1c testing were targeted in this study. At least two HbA1c tests were required for this study to examine adherence to the recommended testing frequency and a change in HbA1c value in patients.
Data
Study data included non-identifiable electronic health records collected from a total of 254 general practices situated in the state of Victoria, Australia. Outcome Health, as data custodians, routinely gather the electronic data from clinical information systems (CIS) in general practices into the Population Level Analysis and Reporting (POLAR) Aurora research platform in a de-identified format.18
The details of the data extracted from POLAR are well documented elsewhere.19 Briefly, the data primarily consisted of patient demographics (age, gender, year of birth, socioeconomic status (SES), remoteness of residential location), practice visit (date of visit, purpose), diagnosis, pathology testing (both ordered tests and results) and prescription. Pathology data include not only information on the tests ordered by GPs but also the results of those tests. In Australia, as the samples are collected and the results become available, pathology laboratories send the electronic results to the CIS of practices who requested the tests.
Patients with type 2 diabetes and complications of interest were identified using their Systematized Nomenclature of Medicine-Clinical Terms (SNOMED) codes in the diagnosis field. The SNOMED codes that fall into the parental concept of ‘diabetes mellitus type 2 (disorder)’, ‘acute ischemic heart disease (disorder)’ and ‘chronic kidney disease (disorder)’ as per Public Health Information Network Vocabulary Access and Distribution System20 were extracted for this study. Identification of pharmacological treatment for patients with diabetes was derived from the Anatomical Therapeutic Chemical classification code in the prescription data. Prescriptions under the group of A10 were selected as diabetes medication. In this study, treatment regimen was categorised into three groups: insulin (A10-A), oral glucose-lowering agents only (A10-B) and no medication (ie, no A10 group prescription records). An insulin group can include patients using the combined therapy with oral glucose-lowering agents (oral agents).
Adherence rate and groups
An adherence rate (%) was calculated for each patient by dividing the number of HbA1c tests performed within the recommended intervals (n) by the total number of the conducted tests (N) minus 1 during the study period and multiplying by 100, that is, (n/(N−1)×100). As the first test observed during the study period does not have the preceding test, one test is subtracted from the total number of observed tests (N). For instance, if a patient had a total of 8 HbA1c tests during the study period and 5 of these were performed within the recommended time intervals since the preceding tests, the adherence rate would be 5/(8−1)×100, thereby 71.4%. As per Australian clinical guidelines,9 14 we considered 6 months (+15 days) as the recommended interval when a previous HbA1c testing result was at goals of ≤53 mmol/mol with a range of 48–58 mmol/mol. The recommended interval until the next test was considered 3 months (+15 days), otherwise (ie, above the target range). To compare patients with different levels of adherence rate, patients were categorised into three groups based on the equally spaced range of adherence rates: low (≤33%), moderate (34%–66%) and high (>66%).
Statistical analyses
The primary outcome of interest was the longitudinal changes of HbA1c levels over 5 years by adherence to the testing frequency recommended by clinical guidelines. The secondary outcomes included the association between adherence levels and the development of IHD and CKD during the study period. Since adherence and outcomes of interest in this study had no temporal relationships, this study did not set out to establish the causal relationships but to examine the associations.
Two descriptive analyses were carried out as the preliminary evaluation on study patients. The first descriptive analysis presented the median and interquartile range (IQR) of adherence rate by patient characteristics and medication treatment at baseline. Baseline refers to the time of the first HbA1c test in a patient. The second descriptive study was an assessment of the sociodemographic distributions of patients by adherence group.
Based on the descriptive studies, a generalised additive mixed model (GAMM) with propensity score weighting was used to evaluate how the primary outcome (ie, HbA1c levels) in each adherence group had changed over time. The application of a propensity score method is to control for sample selection bias in non-randomised or observational studies.21 The common techniques for achieving this include matching, stratification and weighting.22 In this study, the propensity score weighting for each study patient was estimated based on generalised boosted models22 to adjust for the potential confounders of the three adherence groups. The variables included in computing the propensity score weights were determined by descriptive analyses. Balance diagnostics were conducted to assess the quality of the estimated weights by using the absolute standardised mean difference and the p-value tests.22–24 After quality assessments, we then built a GAMM with the estimated propensity score weights which regressed the HbA1c value on covariates, such as time to adjust for unknown time-varying effects, and adherence group (ie, low, moderate or high). Patient sociodemographic variables selected using a stepwise process with significance criteria (p<0.05) were also included in the final model in order to adjust for the associations with HbA1c values. To ensure selecting the important sociodemographic covariates, we iterated the processes of both backward and forward methods, changing the combinations of variables and assessing the goodness of fit for models by using the likelihood ratio tests. Additive models were used in this study due to no a priori linearity assumptions between continuous variables (eg, age and time) and HbA1c levels. A variable for patient was included as a random effect in GAMM to account for the repeated HbA1c testing per patient.
To examine the association between adherence level and development of IHD and CKD during the study period, the estimated propensity score weighting was similarly applied in logistic regression models using the quasibinomial distribution with robust standard errors (SEs). The regression models for the secondary outcome included, in addition to adherence group, the covariates of age and gender as their linkage with these diseases are well acknowledged.25 26 Other sociodemographic covariates (eg, SES, remoteness) were included based on the stepwise process as undertaken for the primary outcome. Since the frequency of practice visits for HbA1c testing can be associated with the diagnoses of diseases, the number of HbA1c tests observed during the study period was also included as the proxy of visits.
All regression analyses included a variable for a patient’s treatment regimen to account for the underlying severity of the patient’s diabetes condition and the risk of subsequent complications. To achieve the target HbA1c, the RACGP guideline14 recommends diabetes management to begin with lifestyle modification (eg, exercise and diet) followed by pharmacological interventions as the disease progresses. If lifestyle mediation is not effective enough in controlling hyperglycaemia, then oral glucose-lowering medication, such as metformin, is generally suggested as the first line of pharmacological therapy.14 The use of insulin is recommended for patients with suboptimal glycaemic control despite the usage of the maximum doses of oral glucose-lowering agents.14
All regression analyses results were provided by group of adherence level (ie, low, moderate and high adherence groups). All analyses were performed in R (V.3.4.1) with the twang package23 for estimating propensity score weights.
Sensitivity analysis
Demographic distributions were compared between patients who were selected and excluded from this study in order to examine consistency in population characteristics. Another sensitivity analysis was conducted for regression analyses with different cut-off points for grouping patients by adherence rate to ensure the consistency of the results since the cut-off points (low: ≤33%; moderate: 34%–66%; and high: >66%) were arbitrarily determined. The regression analyses without propensity score weights were also examined to check whether or not the results differed.
Results
Patient selection
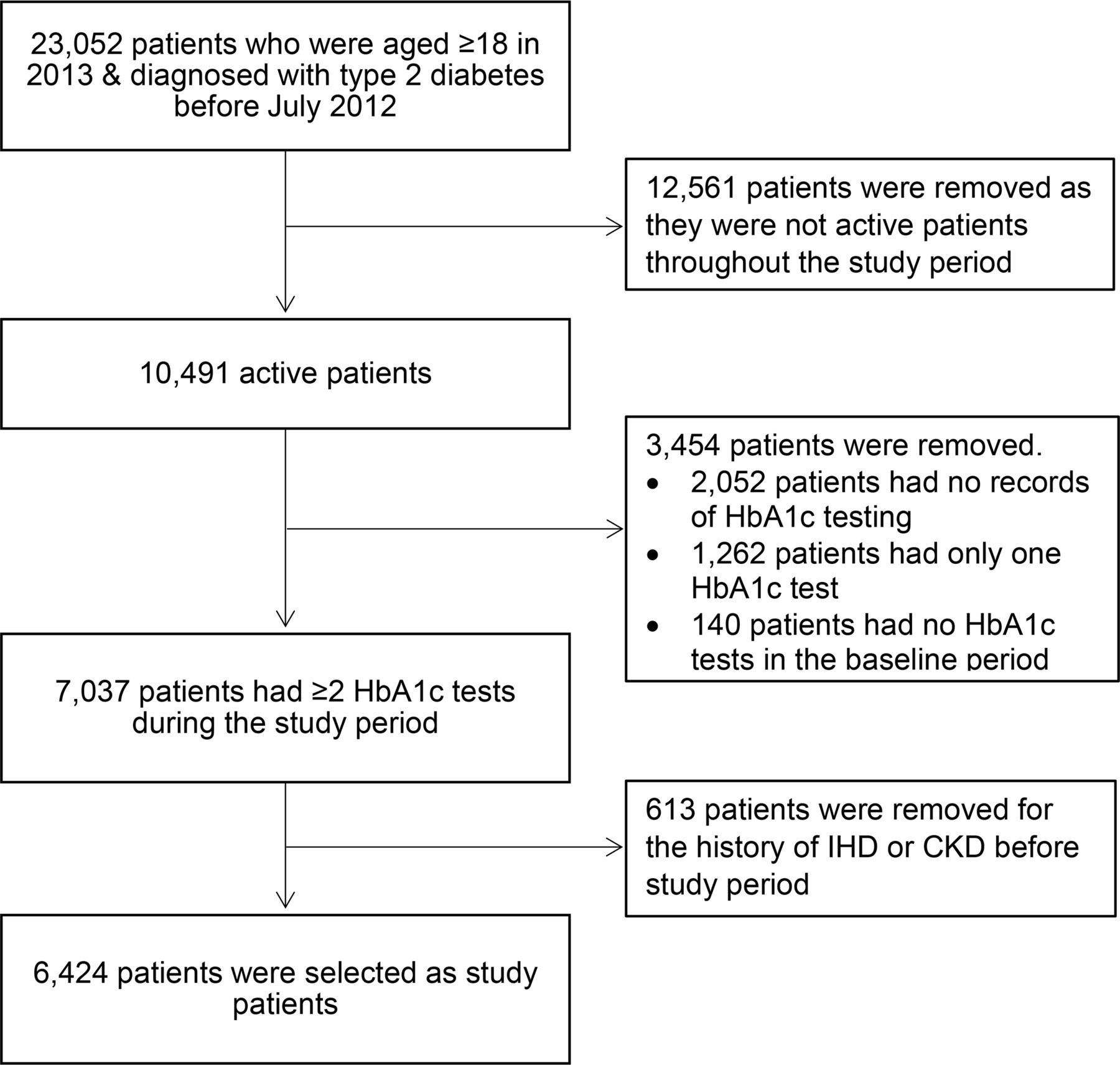
There were a total of 23 052 patients who were ≥18 years old in 2013 and diagnosed with type 2 diabetes before July 2012 in the original extracted data (figure 1). Within the identified patients, 10 491 had attended study practices as active patients throughout the study period. Of these patients, 7037 met the inclusion criteria of two or more records of HbA1c tests from July 2013 to June 2018, one of which was carried out in the first year of the study period. After a further 613 patients were excluded due to history of IHD or CKD before the study period, a final data set of 6424 patients were identified for the study. The make-up of population demographics was similar between the selected and excluded patients (online supplemental figure S1).
Supplemental material

Flow chart of study population selection. CKD, chronic kidney disease; HbA1c, glycated haemoglobin A1c; IHD, ischaemic heart disease.
Descriptive analyses
Among the 6424 study patients, the median number of total HbA1c tests performed during the study period per patient was 8 times (IQR 6–11 times). The yearly median was 1.6 tests per patient (IQR 1.2–2.2 tests). Patient distributions and adherence rate by sociodemographic characteristics are provided in table 1. The majority of patients at baseline were aged ≥55 (85.9%), were in middle or higher SES (SES ≥3, 75.5%), resided in major cities (80.0%) and were treated with a pharmacological regimen (72.0%) (table 1). The overall median adherence rate for patients with type 2 diabetes was 50% (IQR 25.0%–71.4%). The median adherence rates showed an increasing trend by age. The adherence rates were relatively similar when considering other demographic variables.
Patient characteristics at baseline
The distribution of patient population by adherence level is presented in table 2. There were a total of 1928, 2411 and 2085 patients in the low, moderate and high adherence groups, respectively. The median number of HbA1c tests carried out during the study period increased with adherence level: 5 times (IQR 4–7) in the low adherence group and 8 (IQR 7–10) and 11 (IQR 11–13) times in the moderate and high adherence groups. The mean age (low: 65.3; moderate: 66.7; high: 68.0) and proportion of patients from regional or remote areas (low: 17.9%; moderate: 19.5%; high: 22.3%) slightly increased as adherence improved. The lowest proportion of patients who developed complications during the study period was found in the low adherence group.
HbA1c testing frequency and patient distributions by adherence level
The cumulative incidence of IHD in all adherence groups was about ≤20 cases (≤1%) (table 2). The crude odds ratios (ORs) of IHD were 1.5 (95% confidence interval (CI) 0.7 to 3.2) and 1.7 (95% CI 0.8 to 3.5) when the IHD incidence in the low adherence group was compared with the moderate and high adherence groups, respectively. The CKD incidence in the low adherence group (2.0%) was nearly half of the incidence in the moderate (3.7%) and high (3.8%) adherence groups. The crude ORs of the CKD cumulative incidence were 1.9 (95% CI 1.3 to 2.8) and 2.0 (95% CI 1.3 to 3.0) when the low adherence group was compared with the moderate and high adherence groups, respectively.
Regression analyses
As per the descriptive evaluations, all sociodemographic variables (ie, age, gender, SES and remoteness) in addition to the HbA1c value and medication regimen at baseline were included in computing the propensity score weight for each patient. Balance diagnostics were conducted to assess the balance of the covariates after estimating the weights (online supplemental figures S2−S3). The estimated weights were then incorporated into a mixed-effect model. The regression model included age at the time of testing in addition to treatment regimen at the time of testing, time to adjust for time-varying effects and adherence group. Other sociodemographic variables such as gender, SES and remoteness were also assessed, but not considered in the model as neither improved model fitness nor were significant associations with HbA1c detected.
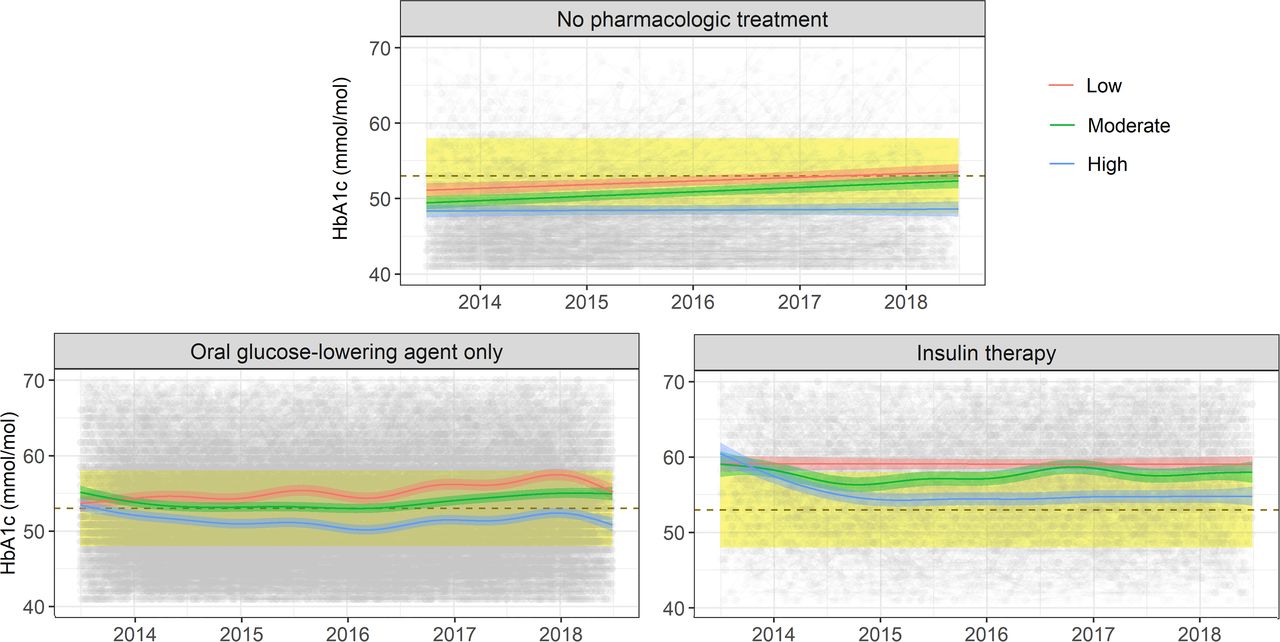
Figure 2 shows the estimated longitudinal change in HbA1c values by adherence group for each treatment regimen. Overall, the estimated HbA1c values at the beginning of the study period were similar across all three adherence groups; however, the HbA1c values for patients with low adherence either increased over time or remained above the target range.
{kind=link}
{kind=link}
Estimated HbA1c values by adherence and treatment. The dotted lines and yellow bands present the point and range of target HbA1c values (53 mmol/mol with a range of 48–58 mmol/mol). The coloured lines and shades denote the estimated HbA1c values and 95% confidence intervals, respectively. Grey shades are observed HbA1c values in patients. HbA1c, glycated haemoglobin A1c.
Among patients with no pharmacological interventions, HbA1c values in all adherence groups were at the lower end of the target range at the beginning of the study period. The HbA1c values remained low over 5 years for patients with high adherence, whereas the values gradually increased for patients with low and moderate adherence. Similar results were observed in patients taking oral glucose-lowering drugs. The HbA1c values in patients with low and moderate adherence gradually increased, while HbA1c levels in the high adherence patients were consistently below the target level throughout the study period.
For patients on insulin therapy, HbA1c values already exceeded the target range at the beginning of the study period. The HbA1c levels in patients with high adherence, however, declined towards the target level in the first couple of years and remained close to the target level for the rest of the study period. In contrast, the blood glucose levels in patients with low adherence did not change and thus remained above the target range throughout the study period. The moderate adherence group also exhibited HbA1c levels that hovered around the upper end of target range.
After adjustment for demographic factors (ie, age and gender) and the propensity score weights in the regression analyses, there was a potentially negative association between adherence to the recommended HbA1c testing frequency and CKD. While moderate adherence had no conclusive association with CKD (OR: 0.46, 95% CI 0.19 to 1.07), patients with high adherence (OR: 0.42, 95% CI 0.18 to 0.99) showed significantly less risk of developing CKD when compared with the low adherence group. The association between adherence and IHD was similarly assessed but was not identified (online supplemental table S1).
For sensitivity analyses, regression models with different cut-off points for adherence groups were performed. The longitudinal trends in HbA1c values and diabetes-related complications were consistent with the main results regardless of changing the cut-off points. In other sensitivity analyses for regression analyses without weights, there were slightly greater differences in HbA1c values between three adherence groups in the early study period; however, the overall longitudinal trends did not change. The analysis on diabetes-related complications without weights also had consistent results with the main results (online supplemental table S1 and figure S4).
Discussion
We demonstrated that patients’ HbA1c testing adherence to the guidelines in type 2 diabetes had a striking and important association with patient outcomes in Australian general practice. First, we identified the course of change in HbA1c outcomes by adherence to the practice guidelines on testing frequency. To our knowledge, this study was the first to examine in depth the longitudinal changes of glycaemic control with testing intervals in patients with type 2 diabetes, underpinning both the importance of adherence to guidelines, as well as evidence that supports the guidelines’ recommendations. Our results illustrated that HbA1c values in patients with poor adherence gradually increased over time, or if it reached a level above the target range it remained uncontrolled. Adequate adherence to the recommended testing frequency appeared particularly crucial for patients on insulin therapy. For patients taking insulin, only when patients had high adherence HbA1c levels could be controlled well within the target range. The finding was not surprising, considering patients on the potent pharmacological regimen commonly have marked hyperglycaemia, which requires close monitoring and care for control.
Second, we identified an association between inadequate HbA1c testing frequency and higher risk of CKD. Previously, a 9-year retrospective cohort study from a tertiary care centre in India had similarly identified in the descriptive analyses that patients with irregular HbA1c testing had significantly higher HbA1c values as well as a higher incidence of kidney disease than patients who regularly performed the testing biannually.13 The positive association between regular monitoring testing and better patient diabetes outcomes can be attributed to various factors, of which regular patient–clinician interaction is critical. Regular patient–clinician communication not only supports the provision of timely care, but can include informational and emotional support.27–29 Emotional care, such as mutual trust and acceptance from clinicians, is particularly linked with open communication about self-care and thus improves self-care behaviours in patients.30 In diabetes care, self-care such as exercise, healthy diet, self-monitoring of blood glucose and adherence to medications is also an essential element of diabetes management and a significant predictor of patient outcomes.31
Our study also identified that the overall adherence rate was only 50%, with the median testing frequency of 1.6 tests per year, which is less than the recommended frequency (ie, at least 2 tests yearly). Although studies examining HbA1c testing frequency in line with clinical guidelines in patients with type 2 diabetes are limited, low adherence rate and low testing frequency in the population have been suggested by some studies. For example, one 3-year retrospective cohort study from the USA12 reported only 7% of patients were fully meeting the testing frequency recommended by the American guidelines (the same recommendations as Australian guidelines). Another study on a diabetes cohort from Luxembourg also reported that more than half of the population (55%) had no HbA1c tests from 2000 to 2006.32 These findings illustrate the underuse of HbA1c testing as well as low adherence to the guidelines’ recommended testing frequency are potential issues in patients with type 2 diabetes.
There are some limitations to consider in this study, however. One is that our study population consisted of patients who regularly visited practices with records of HbA1c testing and with no history of IHD and CKD. Although the selection of such patients was necessary to identify patients who were present in the study practices throughout the study period and to examine the development of complications over time, it may have contributed to selection bias in our findings due to exclusion of patients who were less healthy and less engaged in monitoring care. However, our sensitivity analysis has shown no obvious differences in the demographics between patients who were selected and excluded based on the criteria of regular practice visits and records of HbA1c testing. In addition, the existing literature has well documented the association between good glycaemic control and better self-care management, including adherence to practice visits for follow-up.33 Given the positive association between practice visits and glycaemic control, it seems more reasonable to consider that our findings are conservative estimates. Also, if a patient visited a practice outside our study boundary as a one-off, those results may not be captured unless they were asked to be forwarded to their regular study practice. However, such cases would be limited since it is less common for Australian patients, particularly patients aged over 50 (13%–22%), to attend multiple practices.34 Thus, it is less likely that we have missed a substantial amount of HbA1c tests to the extent of significantly changing our findings. The other limitation is that the general practice data did not contain sufficient data that would allow us to examine mortality and some of the serious complications that require tertiary or special care. The number of complications is most likely underestimated considering that the current literature suggests approximately 19%–35%35 and 10%–21%36 for CKD and IHD prevalence in patients with diabetes, while our study identified only 3% and 1% of study patients developed CKD and IHD, respectively. Another important limitation is the unavailability of information in our study due to insufficient quality of data, such as dose modification of the antidiabetic medication and patients’ body mass index, weight, family history, smoking habit and ethnicity. Such data, however, would have been a critical resource to determine patients’ disease progression as well as predisposition to complications.
Despite these limitations, there are substantial strengths in our study that existing research could not offer. One is the representation of a general diabetes population. Our study used data collected from about 250 general practices in Australia, where the universal healthcare system ensures equal access to public healthcare, including visits to GPs for continuity of care for chronic diseases like diabetes.14 Thus, the use of data collected from Australian general practices offers us a great advantage to understand the general characteristics of patients with diabetes and their care.15 Furthermore, our results reinforce the importance of the use of clinical guidelines for better diabetic care. Current guideline recommendations on testing frequency are largely established by expert opinion,8–10 with few studies rigorously evaluating the clinical impact of the testing frequency in line with guidelines on patient outcomes. While this study did not evaluate the causal relationship between adherence to the recommended HbA1c testing frequency and patient outcomes, our findings may be used as supporting evidence for the effectiveness of guideline-recommended testing intervals as well as the significance of adherence to guidelines for better outcomes in patients with type 2 diabetes.
Overall, our study points to the continuing need to improve adherence to the guidelines on HbA1c testing for better patient outcomes. In planning practical quality improvement interventions, however, it is important to acknowledge that the mechanisms of regular monitoring care adherence in type 2 diabetes are highly complex. The existing literature suggests patient engagement in monitoring care can be impacted by patient-centred (eg, health literacy, transportation, SES) and clinician-centred (eg, gender) factors and by the relationship between the patient and the clinician.29 30 37–39 Thus, the key factors for monitoring care adherence can vary by population and location due to different environments (eg, healthcare systems, access to healthcare) and demographics of patients and clinicians.40 While a multifaceted approach that integrates both patient and clinician factors is imperative, the design of initiatives may ultimately require a population-specific investigation to identify the key factors and drivers of improvements in monitoring care, including HbA1c testing, in patients with type 2 diabetes.
Conclusion
This in-depth study was the first to examine HbA1c levels in patients with type 2 diabetes longitudinally in relation to adherence to clinical guidelines. Our results illustrated the potential link between adherence to testing frequency recommendations and better glycaemic control and lower risk of subsequent complications.
Data availability statement
No data are available.
Ethics statements
Ethics approval
Outcome Health obtained ethical approval to use de-identified data extracted from general practices for research purposes (The Royal Australian College of General Practitioners (RACGP) National Research and Evaluation Ethics Committee (NREEC) 17-008). Ethical approval for data access and analysis for the study was also obtained from Macquarie University Human Research Ethics Committee (5201700872).
Acknowledgments
Authors would like to thank the staff of Outcome Health and three PHNs (Eastern Melbourne (EMPHN), Gippsland (GPHN), and South Eastern Melbourne (SEMPHN) whose feedback allow for a deeper understanding of the data and characteristics of Australian general practice.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @HardieRae
Contributors AG initiated the project and led the development of the Quality Use of Pathology Program grant proposal for this study. AG is a chief investigator on the project and has contributed to the grant proposal. CI developed the design of this paper, extracted the data, performed the data analysis, interpreted the findings and drafted the paper. LL contributed to the development of the design and statistical methods of this study. R-AH contributed to the development of the grant proposal, interpretation of the findings and drafting of the paper. All authors have reviewed and approved the final version of the manuscript.
Funding This study was funded by the Australian Government Department of Health, Quality Use of Pathology Program (4-2QFVW4M) and NHMRC Partnership Centre for Health System Sustainability (910003).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.