Article Text

Abstract
Background When the COVID-19 pandemic restricted visitation between intensive care unit patients and their families, the virtual intensive care unit (vICU) in our large tertiary hospital was adapted to facilitate virtual family visitation. The objective of this paper is to document findings from interviews conducted with family members on three categories: (1) feelings experienced during the visit, (2) barriers, challenges or concerns faced using this service, and (3) opportunities for improvements.
Methods Family members were interviewed postvisit via phone. For category 1 (feelings), automated analysis in Python using the Valence Aware Dictionary for sentiment Reasoner package produced weighted valence (extent of positive, negative or neutral emotive connotations) of the interviewees’ word choices. Outputs were compared with a manual coder’s valence ratings to assess reliability. Two raters conducted inductive thematic analysis on the notes from these interviews to analyse categories 2 (barriers) and 3 (opportunities).
Results Valence-based and manual sentiment analysis of 230 comments received on feelings showed over 86% positive sentiments (88.2% and 86.8%, respectively) with some neutral (7.3% and 6.8%) and negative (4.5% and 6.4%) sentiments. The qualitative analysis of data from 57 participants who commented on barriers showed four primary concerns: inability to communicate due to patient status (44% of respondents); technical difficulties (35%); lack of touch and physical presence (11%); and frequency and clarity of communications with the care team (11%). Suggested improvements from 59 participants included: on demand access (51%); improved communication with the care team (17%); improved scheduling processes (10%); and improved system feedback and technical capabilities (17%).
Conclusions Use of vICU for remote family visitations evoked happiness, joy, gratitude and relief and a sense of closure for those who lost loved ones. Identified areas for concern and improvement should be addressed in future implementations of telecritical care for this purpose.
- visiting
- critical care
- human factors
- qualitative research
- quality improvement
Data availability statement
Data are available upon reasonable request. Data can be shared upon reasonable request.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
The COVID-19 pandemic has resulted in increased utilisation and forced adoption of telehealth platforms across the world. Recent updates on telehealth billing include more than 80 new US Center for Medicare and Medicaid Services codes and relaxed requirements for software compliance with the Health Insurance Portability and Accountability Act in the USA, as well as waiving of origination site restrictions,1 collectively contributing to widespread adoption of telehealth technologies. In addition to its utility for screening and non-emergency care, many healthcare organisations have adopted telehealth systems for inpatient settings such as intensive care units (ICUs). Virtual ICUs (vICUs), also known as electronic ICUs and telecritical care, have gained popularity among health systems in the last decade to address a significant shortage of intensivists. These systems have expanded the boundaries of a traditional ICU while delivering tangible benefits such as decreased mortality, reduced length of stay, reduced cost and improved quality of care.2 3 While the telepresence functionality represents its chief utility, vICU’s other latent functions have been recognised by many. For example, ICU patients and their loved ones were deeply affected when, for safety reasons, our hospital restricted visitation to the ICU to prevent infection risk; vICU technology could function to allow for remote visitation.
Many research studies on ICU Liberation Bundle (formerly ABCDEF Bundle) have demonstrated that the family engagement (the F in the A–F Bundle)4 has a positive impact by decreasing anxiety, confusion, agitation and delirium in the ICU patient. Previous studies also show that separating families from the patients can adversely impact the patient’s feelings of security and ultimate outcome.5 In addition, patients with COVID-19 in the ICU face additional risk of acquiring ICU-related physical, cognitive and mental health impairments, or post-ICU syndrome, which may manifest as delirium, depression or post-traumatic stress disorder and can persist beyond the acute hospitalisation. ICU Liberation Collaborative studies have shown that families play a very important role in the recovery of patients and their quality of post-ICU life.6
During the COVID-19 pandemic, almost all hospitals in the USA disallowed visitors for all adult inpatients including all COVID-19 and non-COVID ICU patients. Although commonly available for everyday use, video chat technologies such as FaceTime, Zoom and Skype have limited value in an ICU setting with a highly infectious critically ill patient population. Generally sedated and intubated, these patients cannot independently access these social media oriented technologies and require the medical staff to bring in and position mobile equipment (smartphone or tablet), subjecting the staff to unnecessary risk of infection while drawing down the limited supply of personal protective equipment (PPE). In contrast, the vICU infrastructure provides a much safer and more accessible alternative, reducing in particular the need for staff to go in and out of the protective area.
In the face of mounting patient anxiety due to isolation from their family members, our hospital decided to offer a particular vICU application, called the Consultant Bridge, to virtually connect families with their loved ones in the ICU. Normally reserved for virtual MDs (vMDs) and consultants, Consultant Bridge became instrumental in providing ICU patients emotional support while improving the overall quality of their care. In this paper, we document this improvised utilisation of vICU technology in our health system to allow family members to visit an ICU patient during the COVID-19 pandemic virtually and present the findings from postvisit interviews with family members to understand barriers, challenges, concerns, feelings and opportunities to improve this functionality. To our knowledge, this is the first family-centred study evaluating the usage of a vICU for family visitation.
Methods
Setting
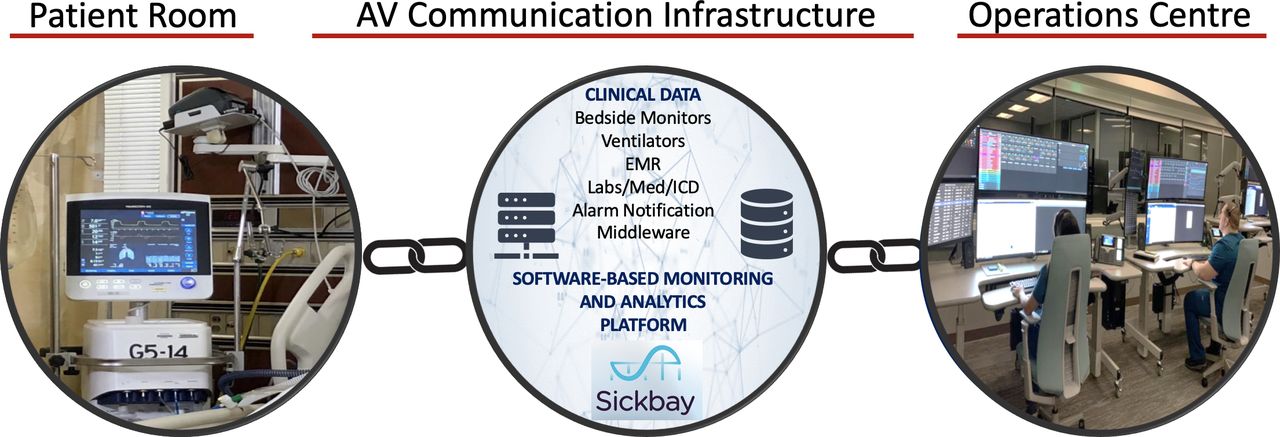
In 2019, Houston Methodist Hospital launched its innovative vICU programme to augment and enhance the critical care services being provided in its ICUs. The virtual ICU at Houston Methodist has three main components: the operations centre (OC), the bedside team and the audio-visual (A/V) communication infrastructure that links the two (figure 1).7

Key components of Houston Methodist Hospital Virtual ICU. ICU, intensive care unit.
The OC provides a central command centre where the vMDs and virtual RNs (vRNs) sit and connect with the bedside clinicians while monitoring the patient. Our OC uses an FDA-cleared software-based monitoring and analytics platform called Sickbay. The physiological data from several bedside monitors and devices including ventilators, haemodynamic monitors and the static data from the electronic medical records interface with this platform. Novel algorithms transform these big data into actionable information in the form of risk scores, which feed into clinical decision support systems. The OC is also where virtual A/V connections are established with the patients’ rooms. The camera in the patients’ room has a 360° pan, tilt and zoom capability so that the vMDs and vRNs can examine the patient and closely observe the intravenous fluids, the drip rates, the monitors and the ventilator settings and, of course, communicate with the patients and the bedside providers.
For any emergent or urgent calls, the bedside teams can access the vICU by pressing the virtual alert button that prompts the vMDs or vRN to immediately camera-in to the patient’s room. Before installation of vICU infrastructure, the vICU team and the bedside clinicians collaborated with the key stakeholders to develop the appropriate workflows.
To arrange a virtual visit, the family members reached out directly to the unit or the vICU OC. The two vRNs in the OC then collaborated with the bedside staff to determine the communication technology capabilities and preferences of the patients’ families, as well as to ensure the patient is camera ready for the family visit. One of the vRNs would then send a text or email link to the family members’ internet-connected devices (eg, smartphones, tablets and computers). Clicking that link instantly connected the patient’s family with the ICU room in which their loved one was present, using the cameras and monitors already installed in the ICU rooms. The bedside nurse usually stayed on to facilitate communication with the family, especially if the patient was intubated. Restrictions on visitors also applied to non-COVID patients, and hence the Consultant Bridge was used for all types of virtual ICU patients. Using Consultant Bridge, we averaged about 35 calls per day in 3 weeks (from 6 to 27 April 2020). The virtual visits lasted around 30 min on average.
Data collection and analysis
A short interview was designed to elicit family members’ experience with their visit after each call. The interview entailed three main areas of questioning: (1) feelings experienced during the visit, (2) barriers, challenges or concerns faced using this service, and (3) opportunities for improvements (see online supplemental file 1 for interview script). The first and third areas involved an open-ended question asking about feelings or opportunities for improvement, respectively. For the second theme, callers were asked to choose from any of the four categories of perceived barriers related to: (1) keeping in touch with their patients, (2) inquiring about health status or care processes being administered, (3) anticipating their loved one’s future course and timeline, (4) questions to providers regarding care, processes or plans, or add any other concerns. Responses to ‘other concerns’ as well as barriers and opportunities were analysed qualitatively.
Supplemental material
Two vRNs (both female) in the OC completed the interviews immediately after the visit over phone. The interviewers did not have prior training in qualitative research and followed a scripted interview guide. Interviewers tried to document the comments verbatim in real time. No probing or follow-up questions were asked. Of the 639 visits completed, 230 family members verbally consented to participate in the postvisit interviews. However, not all participants responded to all questions. Due to the emotional and private nature of the visits, no demographic data were collected. In addition, interviews were not recorded to protect family members’ privacy. Interviews took between 5 min and 10 min. Transcripts were not returned to participants. After each week of the data collection, the authors (FS and AD) reviewed the data and discussed thematic saturation.8 Saturation was reached after 3 weeks of data collection (6–27 April 2020).
An inductive thematic analysis9 was used for the analysis of the second (other concerns) and the third (areas for improvement) interview questions. Two coders (a female MD and a male PhD outcomes researcher), both with experience in qualitative data analysis, independently reviewed each response and assigned tentative labels (or codes) in Microsoft Excel, a process referred to as open coding. Coders then reviewed the responses and open codes to identify relationships and similarities between codes (axial coding) and merge codes into broader themes that represented the core concepts (selective coding). Coders then discussed selective codes iteratively and finalised a set of consensus codes. None of the interviewers or coders had any relationships with the interviewees. The family members were told that the data would be used for research and quality improvement.
For theme 1 (feelings), two types of sentiment analysis were conducted. The first method involved automated analysis in Python using the Valence Aware Dictionary for sentiment Reasoner (VADER) package.10 This package uses a large lexicon of words rated according to their positive and negative polarity to classify sentiments as well as analysing the intensity of each sentiment. In such a valence-based approach, each positive and negative word is assigned a weight; for instance, ‘overwhelming’ has a higher sentiment intensity than ‘good’. A sentiment score varying between −1 and 1 is then calculated based on the type and intensity of the sentiment. For this analysis, VADER was applied to the total text of notes per respondent. In the second method, a coder reviewed each response, manually evaluated the content and labelled them as negative, neutral or positive to define sentiment polarity. The results from the two methods were compared with assess reliability.
The research received an exemption from the institutional review board at Houston Methodist Hospital. The Consolidated criteria for Reporting Qualitative research guidelines11 were used for reporting the methods, analysis and results.
Results
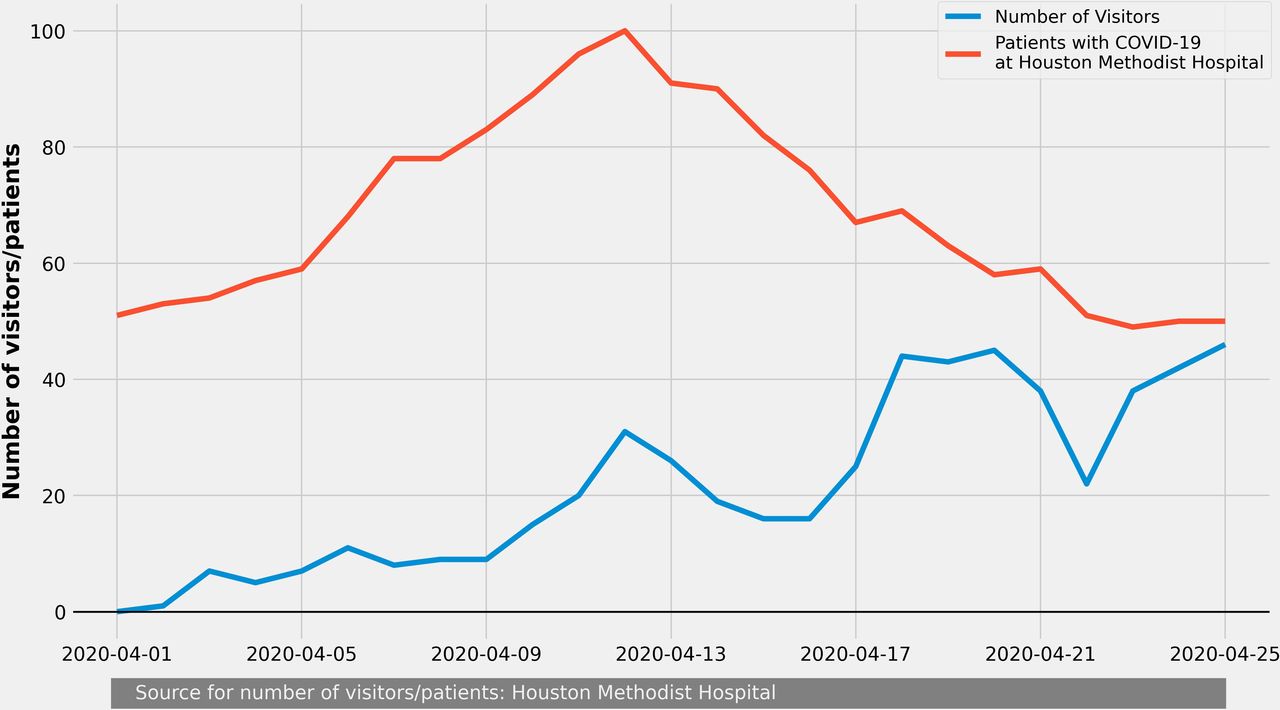
On average, 21.7 calls a day were completed from 1 April to 23 April 2020, representing 230 distinct callers. About 67.8% of callers had a second visit in this period. Figure 2 shows the number of visits compared with the number of COVID-19 positive patients in our hospital system. As shown in this figure, the number of visits increased over time and at the end of this data collection period almost every COVID-19 patient in our ICUs had one visitor per day.

The number of interview participants compared with the number of COVID-19 positive patients.
Overall feelings and sentiments
Figure 3 shows the findings from both the manual and automated sentiment analysis. Our findings show that the sentiments and overall experiences were overwhelmingly positive. Both valence-based and manual coding of sentiment analysis showed that from 230 family members who responded to this question, over 86% had positive sentiments (88.2% and 86.8%, respectively). The mean and median of sentiment intensity were 0.5 and 0.6. This metric is indicative of the degree of the positive opinion of users. However, a small portion of comments were classified as neutral (7.3% and 6.8%) or negative sentiments (4.5% and 6.4%). A two-sample proportion test on the difference of the ratios showed no significant differences between the proportions of negative (z=0.84, p=0.4), neutral (z=0.19, p=0.85) or positive (z=0.43, p=0.66) sentiments between the manual and automated methods. Overall, the majority of participants shared feelings of happiness, joy, gratitude and relief to be able to visit their family members. For some users, there were mixed feelings since seeing their family member intubated contributed to feelings of sadness. For many who lost their loved ones, the technology provided a degree of closure.

{kind=link}
{kind=link}
{kind=link}
Comparison of sentiment polarity between manual and automated classification (A) and intensity of shared sentiments using the automated analysis (B).
So grateful that our whole family and close friends (17 family & friends) had the chance to gather and be united before they unplug all the lines and tubes for our loved one. We were able to pray, cry and sing together. It was really emotional and difficult especially with the current crisis we are all experiencing but we still feel peace and we are grateful that we were able to do this for the last time before he leaves us. He meant a lot to all of us and it pains us to let him go, but we have to. (Participant 45)
Barriers, concerns and challenges
Of the 639 visitors, 170 responded to the first question that allowed them to choose from four predetermined areas of potential concern. Participants could choose more than one category and had the option of adding other concerns. About 15.8% of family members found keeping in touch and/or demonstrating solidarity and support for the patient problematic; 15.8% found inquiring about health status or care processes to be confusing; 11.7% had problems anticipating their family members’ future course; however, only 1% had concerns related to questioning providers regarding care, processes or plans. About 37% of participants had no concerns with their visit and commented that they were satisfied with the system. About 33% of the callers (57/170) who responded to this question commented on other concerns, barriers and challenges. The remainder of the results in this section presents the comments shared by these 57 participants. The qualitative data analysis of comments showed four primary areas of concern: inability to communicate due to patient status, technical difficulties, lack of touch and physical presence and frequency and clarity of communications with the care team.
Inability to communicate due to patient status: about 44% of respondents (25/57) found it challenging to communicate with their patients due to patients being either intubated or going through other procedures. In some cases, patients were sleeping or under the influence of medication. Several family members expressed the importance of, and their expectation for, being able to talk to the patient at the scheduled time and were frustrated when this goal could not be accomplished. One family member complained that calls should not be scheduled at the same time as procedures. Some participants mentioned it was difficult to view the patient who was trying to talk while intubated.
Hardest part is she is not able to speak and voice how she is feeling! (Participant 135)
We couldn’t stay longer because he is sleepy, and we don’t want him to get tired. (Participant 5)
Technical difficulties: about 35% of respondents (20/57) discussed experiencing technical difficulties and found these issues to be a major barrier. The main complaint was related to the inability to hear the patient clearly due to background and equipment noises or the patient speaking slowly or with low volume. Several participants mentioned issues with connection instability (eg, frozen screens). In most of these cases, issues were resolved after a few minutes. A few participants had issues connecting to the system, or in some cases receiving the link due to family members’ network instability. While the system provided the ability to zoom in and out, one participant mentioned difficulty seeing the patient. A few participants mentioned that their patient needed visual (prescription glasses) or hearing support (hearing aids) for communication and the absence of such support was a barrier.
It was hard to hear the patient. He spoke softly. It was easier to hear after putting on earphones. (Participant 66)
Lack of touch and physical presence: about 11% of participants (6/57) mentioned that while the virtual visit filled an important gap, the overall visit experience did not match that of in-person visits. All of these family members shared their desire to be present in person and emphasised the importance of touch, which was lost in their virtual visit.
Frequency and clarity of communications with the care team: about 11% of participants (6/57) expressed concerns related to the impact of virtual visits on the frequency and quality of communication with the care team. Family members expressed concerns regarding the duration of calls and shared their desire to have more time with nurses to ask more questions. A few family members found the ability to schedule calls when they can hear from the attending physician to be a major challenge. One family member found it difficult to understand what the care providers tried to communicate.
Potential improvements to virtual visits
The analysis of data from 59 participants who responded to this question yielded four major themes for potential improvements to virtual family visitation using the vICU technology: on-demand access; improved communication with the care team; improved scheduling processes; and improved system feedback and technical capabilities.
On-demand access: a major theme expressed by half of the participants (51%, 30/59) was the desire to have on-demand access to the technology to initiate calls. The majority of these users expressed their satisfaction with the current technology and asked if it is possible to have more frequent calls with their family members ‘all the time’ or ‘whenever they want’. A few participants requested the ability to control the camera features such as zoom and pan during the call. One user expected to have the ability to send specific requests to care providers (eg, for the patient to watch a movie).
Already grateful for this opportunity, it would be nice if I can just call my patient directly anytime. (Participant 69)
[What I want is to have] unlimited time! It’s a peace of mind to see and hear the patient. (Participant 92)
Improved communication with the care team: about 17% of participants (10/59) discussed the need for more frequent or improved communications with the care team. Participants found the current process of asking for an update somewhat asynchronous. For example, family members expected the care team to provide more frequent updates, provide a rationale for changes in patient status, schedule and plan follow-up calls and schedule visits after major care events. One participant expected to have access to ‘all’ specific updates. A few participants found dealing with multiple care providers difficult and asked for one consistent contact person to inquire about their family member. A few participants requested more access to attending physicians and requested less technical jargon in reporting patient updates.
She’s the healthcare proxy! I’m concerned there wasn’t enough communication! I also can’t translate what the doctors are saying! Too much medical jargon! (Participant 81)
Improved system feedback and technical capabilities: about 17% of participants (10/59) suggested improvements to the technical capabilities of the system as well as better awareness of the system’s existing capabilities. Several participants mentioned difficulties in verifying if the patient could hear their voice. Several others suggested the need for better equipment to reduce the environmental and equipment noise. A few family members suggested improving the network bandwidth to reduce the possibility of being disconnected. One caller suggested using dedicated tablets at the bedside to improve the quality of communication.
Improved process: about 10% of participants (6/59) shared ideas for improving the visitation process. Some participants mentioned long wait times for a virtual call spot due to equipment setup. Others suggested that links should be sent well ahead of time followed by a call to confirm they were received by the family members. Some users suggested the need for reminders regarding the exact time and duration of the call. One participant mentioned the need for better coordination with other family members since several people in the household might want to click on the links sent.
Discussion
In this study, we investigated the family members’ sentiments towards visitation using a virtual ICU platform. While literature establishes the importance of involving family in ICU patient care (eg, refs 4–6), to our knowledge this is the first paper documenting family members’ experiences with virtual patient visits. Our results showed an overwhelming amount of support and approval for the virtual visits. Only a small percentage of family members had negative sentiments, attributed primarily to feelings of sadness stemming from seeing patients in critical condition. Therefore, results should not be interpreted as negative sentiments towards the technology. However, future studies should separate the respondents’ views specific to the technology from their situational emotional responses.
Additionally, vICU technologies have the potential to create an ‘open-ICU’ for family members, enabling them to view/speak to the patient and access a dashboard with real-time patient data. These virtual technological platforms allow family members to participate in the patient care by enhancing the communication between the families and the care teams.
Though highly desirable by family members, on-demand video access to patients can be problematic. Clinical care of ICU patients involves both routine care (eg, bathing, suctioning of endotracheal tube and changing of dressings) and emergent procedures (eg, intubation and central line placement), which may be distressing for patients’ families to observe without context and might be misinterpreted. Due to the unpredictability of bedside care, virtual visits cannot be scheduled in advance but need to take place on an ad hoc basis. Families are often not familiar with the unpredictable nature of ICU care. The nurses in the virtual command centres should explain to family members that appointments may be cancelled or interrupted, should urgent patient care needs arise, to manage family members’ expectations.
At the beginning of the pandemic, our institution, along with others around the country, anticipated a shortage of PPE and implemented protocols to conserve PPE. Using handheld devices such as phones and tablets proved impractical in an ICU setting with highly infectious critically ill patients, requiring the staff to don and doff PPE while bringing the devices in and out of each patient’s room. Therefore, the vICU technology provided an effective tool for us to conserve PPE12 while offloading the bedside nurse from having to hold up or set up a phone or iPad for the patient, particularly if the nurse needs to take care of another patient or conduct other care activities related to the current patient (changing positioning, changing dressings and so on).
In addressing the technical issues encountered with poor video quality or buffering issues, work is needed to investigate whether these issues are related to network issues from the origination site (eg, hospital network) or whether they are due to broadband limitations or interruptions on the user side. In fact, based on these findings, we started an internal investigation and have reasons to believe the connection issues are likely related to the caller’s network. However, callers may not be aware of such issues and may perceive the issue as the ‘system’s’ fault, which may have significant impacts on their overall perception of the system. Providing instructions such as internet speed tests, clear communication of minimum requirements for a virtual call, as well as capabilities to detect slow connections and provide feedback in real-time may help the users calibrate their trust in the capabilities of vICU technology accordingly.
Similarly, our findings show that poor sound quality was a major source of dissatisfaction among users. While more work is needed to evaluate the optimal microphone position and integrate filtering techniques to reduce noise, providing information on the ICU environment in terms of the level of noise, nursing activities and patient condition will help visitors set realistic expectations of the virtual call. For instance, some of the patients were placed in airborne isolation rooms depending on the availability. Turbulence attendant to high air exchange rates in these rooms resulted in unexpected levels of background noise that might explain why some families found the connection to have poor sound quality.
Lastly, there are several opportunities to optimise and streamline processes to enhance the visitors’ experience and support vICU personnel. Currently, the families can arrange the virtual visit by calling the vICU command centre or the bedside nurse. Our current formal protocol for a virtual family visit requires the vICU command centre to coordinate with the bedside team and ensure that the patient is available to participate in the virtual meeting. However, given the increase in demand for such services (as shown in figure 1), there is a need for capacity planning and modelling support to inform coordination efforts. Ideally, the call scheduling feature should be integrated with the medical records and procedure scheduling to avoid any overlap. In addition, visitors can be informed about the uncertainty and possibility that patients may not be available to speak to calibrate their expectations. There is much to learn from the telemedicine literature on processes and protocols for virtual care that is applicable to family visits (see ref 13 for a review of available resources).
This work has several notable limitations. First, in this study, we did not take into account the demographics of families who opted in or out of the virtual visitation programme. We realise that these enabling technologies have the potential to exacerbate racial, income, technological and educational level disparities. Future studies would benefit from incorporating family demographic data to assess the impact of such disparities and encourage equitable access to these technologies. Second, while the feedback received in this study was overwhelmingly positive, such feedback might have been biased by the fact that this was the only available option to visit patients especially after a long wait in some cases. More work is needed to investigate the visitor experiences at various points in time, with larger and more diverse samples, using validated instruments such as Family Satisfaction in the ICU14 to evaluate the sustainability of such initiatives and understand challenges and barriers in more detail. Third, a major limitation of this study is lack of a comparison group. While this was not possible during the COVID-19 pandemic, future studies may consider comparing the findings from the vICU visitation with other modes of family–patient communication such as mobile devices. Finally, the interviewers did not have experience in qualitative research; the interviews were short, which did not allow for elaborations and follow-up questions; the interviews were conducted immediately after the visit when family members might have been emotional; and conversations were not recorded, which might have affected the depth and quality of this inquiry. In-depth interviews using experienced interviewers, and scheduled at a later time, are necessary to investigate issues related to virtual family visitation further.
Conclusion
The COVID-19 pandemic has resulted in the disruption of an integral aspect of care in most ICUs across the world: family visitation. Given the strict isolation and cleaning protocols in most ICUs, using mobile devices poses additional challenges. As a result, patients’ families in many hospitals, including ours, had to wait for weeks without being able to see or talk to their loved ones in the ICU. In this paper, we documented our novel and improvised adoption of the virtual ICU technology to enable family visitation and explore the feedback we received. While the overall experience of family members was overwhelmingly positive, several key barriers, concerns and areas for improvement were identified. Given the promise shown by this successful implementation, recent emphasis on involving family members in care (eg, ref 15) and the importance of visual care platforms in the post-COVID era, we hope that the practical takeaways and suggestions provided here can inform potential future efforts.
Data availability statement
Data are available upon reasonable request. Data can be shared upon reasonable request.
Ethics statements
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors have been involved in the planning, conduct, and reporting of this research.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.