Article Text

Abstract
Background Diagnostic errors unfortunately remain common. Electronic differential diagnostic support (EDS) systems may help, but it is unclear when and how they ought to be integrated into the diagnostic process.
Objective To explore how much EDS improves diagnostic accuracy, and whether EDS should be used early or late in the diagnostic process.
Setting 6 Canadian medical schools. A volunteer sample of 67 medical students, 62 residents in internal medicine or emergency medicine, and 61 practising internists or emergency medicine physicians were recruited in May through June 2020.
Intervention Participants were randomised to make use of EDS either early (after the chief complaint) or late (after the complete history and physical is available) in the diagnostic process while solving each of 16 written cases. For each case, we measured the number of diagnoses proposed in the differential diagnosis and how often the correct diagnosis was present within the differential.
Results EDS increased the number of diagnostic hypotheses by 2.32 (95% CI 2.10 to 2.49) when used early in the process and 0.89 (95% CI 0.69 to 1.10) when used late in the process (both p<0.001). Both early and late use of EDS increased the likelihood of the correct diagnosis being present in the differential (7% and 8%, respectively, both p<0.001). Whereas early use increased the number of diagnostic hypotheses (most notably for students and residents), late use increased the likelihood of the correct diagnosis being present in the differential regardless of one’s experience level.
Conclusions and relevance EDS increased the number of diagnostic hypotheses and the likelihood of the correct diagnosis appearing in the differential, and these effects persisted irrespective of whether EDS was used early or late in the diagnostic process.
- decision making
- diagnostic errors
- decision support
- clinical
- decision support
- computerised
- medical education
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- decision making
- diagnostic errors
- decision support
- clinical
- decision support
- computerised
- medical education
Background
The need for improved accuracy and rapidity of medical diagnoses—extensively documented in the literature1–5 —became an early focus of the field of medical informatics.
Early efforts to augment the diagnostic process with information technology in the 1970s, using the methods of artificial intelligence and so-called ‘expert’ systems that were available at the time, addressed only specific domains such as infectious6 and gastrointestinal7 diseases. These efforts were followed in the 1980s and 90s by more sophisticated and broadly applicable electronic diagnostic support (EDS) systems that spanned most of internal medicine—QMR, ILIAD, DxPLAIN—among others.8–11
These EDS systems were studied from multiple perspectives. Some studies addressed the accuracy of the systems themselves. That is, when data were entered from a case with a known diagnosis, how often did the system yield the correct diagnosis?12 Other studies examined how well the systems augmented the diagnostic reasoning of clinicians across the spectrum of training and experience when confronted with diagnostically challenging cases.13 That is, do clinicians of varying experience levels make more accurate diagnoses with the aid of EDS than without? Individual studies and meta-analyses revealed small but statistically significant improvements in diagnostic accuracy.8–11 14 15 However, these systems required user training and time-intensive manual entry of data, limiting EDS system use to selected cases rather than routine, regular use. Possibly because of their only modest improvements to diagnostic accuracy,8–11 14 15 time-consuming manual data entry13 or clinician perceptions that they are unneeded,1 16 17 many of these systems from the late 20th century have largely passed into obscurity.
A newer system, Isabel, provides a list of relevant diagnoses via a user-friendly, time-efficient platform. The system is designed around entering a small number of symptoms in free-text without the need for symptom qualifiers, pertinent negatives, medical, social or family history background, physical signs, lab values or investigations. Generating differential diagnoses in this way dramatically reduces the time required to several minutes, making it feasible at point-of-care for both physicians and patients.18–23 Though there is no publicly available technical information on the computational methods by which Isabel generates diagnostic hypotheses, the tool is advertised as using artificial intelligence and natural language-processing techniques, and has been adopted in both experimental18–21 and practical22 23 settings. When Isabel was used by clinicians admitting paediatric patients to the intensive care unit, a 4% improvement in diagnostic accuracy was documented—representing a 30% reduction in harm.17 And so while the improvement in diagnostic accuracy may seem small, it is nonetheless important.
Prior studies of Isabel speak to the accuracy of diagnostic hypotheses it generates, but its potential to augment a clinician’s own diagnostic reasoning remains unclear.24 25 In particular, it is unknown whether Isabel should be integrated early in the diagnostic process during the hypothesis generation stage, or later during the deductive analytical stage.25 The present study addresses this gap by replicating and building on a comprehensive study of ILIAD and QMR published more than 20 years ago.13 Using a similar method and identical clinical test cases, here we examined whether Isabel brings clinical medicine closer to the full potential of diagnostic decision support.
To elucidate how Isabel can be best integrated, we explored whether its benefits are moderated by early or late implementation in the diagnostic process. Early use may increase its effectiveness because all data have not yet been gathered and hypotheses are still formative, so it has the potential to shape the collection and interpretation of data during a history or physical. Conversely, its use later in the encounter when all data are available may provide a final check for unconsidered diagnoses. We therefore designed a study to test these two interventions: early EDS use with only the patient demographics and chief complaint, and late EDS use with all available clinical details. We hypothesised that early EDS use would increase the number of differential diagnostic hypotheses generated, but, because available data are limited, will have minimal impact on accuracy of diagnosis. Conversely, we hypothesised late EDS use would improve diagnostic accuracy, but minimally impact hypothesis generation.
Methods
We explored the impact of Isabel by asking clinicians of varying levels of expertise to work through a series of cases on an online web-based platform, providing a differential diagnosis before and after the use of the Isabel EDS and randomising them to receive EDS either early (when limited information was available) or late (when all information was available) in the diagnostic process. We measured the number of diagnostic hypotheses recorded, presence of the correct diagnosis within the differential and time spent working through the cases.
Design and procedures
Participants were randomised into one of two groups: early or late use of EDS using a standard random number generator in Excel (Microsoft, Redmond). Clinicians in the early group were randomised to use the EDS after only the patient’s demographics and chief complaint were presented, whereas those in the late group used the EDS system after all case details were presented. The entire study was administered via an online platform.
A schematic of the design is shown in figure 1. Participants were told they would be diagnosing written clinical vignettes using an EDS system at some predetermined point in the process. For each case they first received the patient’s demographics and chief complaint (eg, a 32-year-old man presenting with diplopia and difficulty swallowing) and provided an initial differential diagnosis, including as many diagnoses as they felt relevant in decreasing order of likelihood.

Study design and randomisation. Participants from three centres were randomised to either early or late use of EDS to work through 16 written cases. Both groups provided a differential diagnosis three times. The early group was asked to provide a differential diagnosis after the chief complaint and demographics, revise it with use of EDS and conduct a final revision with the remainder of the case material available. The late group was asked to provide a differential diagnosis after the chief complaint and demographics, revise it with the remainder of the case material and then use EDS to revise a second time. EDS, electronic diagnostic support.
The two groups differed only after this provision of the initial differential. Participants in the early group were then asked to (1) use the EDS, then provide a revised differential diagnosis, then (2) read the rest of the case material and provide a second revised differential. This format assessed the implementation of EDS during the preliminary hypothesis generation stage before the full case information was available. In contrast, participants in the late group (1) read the rest of the case and revised their final differential without EDS, then (2) were given access to EDS and asked to further revise their differential. This late implementation occurred during the analytical ratification or deductive stage that occurs once all the case information is available. It should be noted that participants could not go back or use the software multiple times; they could only access it at the specified time. Thus, both groups generated a differential both before and after use of EDS, but the timing of EDS served to enhance either early hypothesis generation or the deductive process that follows.
Participants
We recruited participants from six Canadian medical schools between 1 May and 1 June 2020. Medical students, internal medicine residents, emergency medicine residents, internists and emergency medicine physicians were invited to participate via email. Participation was voluntary. A modest stipend was provided after participants completed the study (students $125, residents $150, practising physicians $250).
Case materials
Case materials were derived from a previous study involving EDS.13 The author of the previous study (CF) has maintained control of distribution, so cases cannot have been seen by participants. All cases were based on real patients. Cases were reviewed by two investigators to ensure they were current. Sixteen of the 36 cases available were chosen. We selected the eight easiest and eight hardest cases based on actual performance data from a previous study13 (see online supplemental appendix 1 for a sample easy and hard case). The EDS was not previously trained on the case material (personal communication, IsabelHealthCare.com).
Supplemental material
Electronic differential diagnosis support
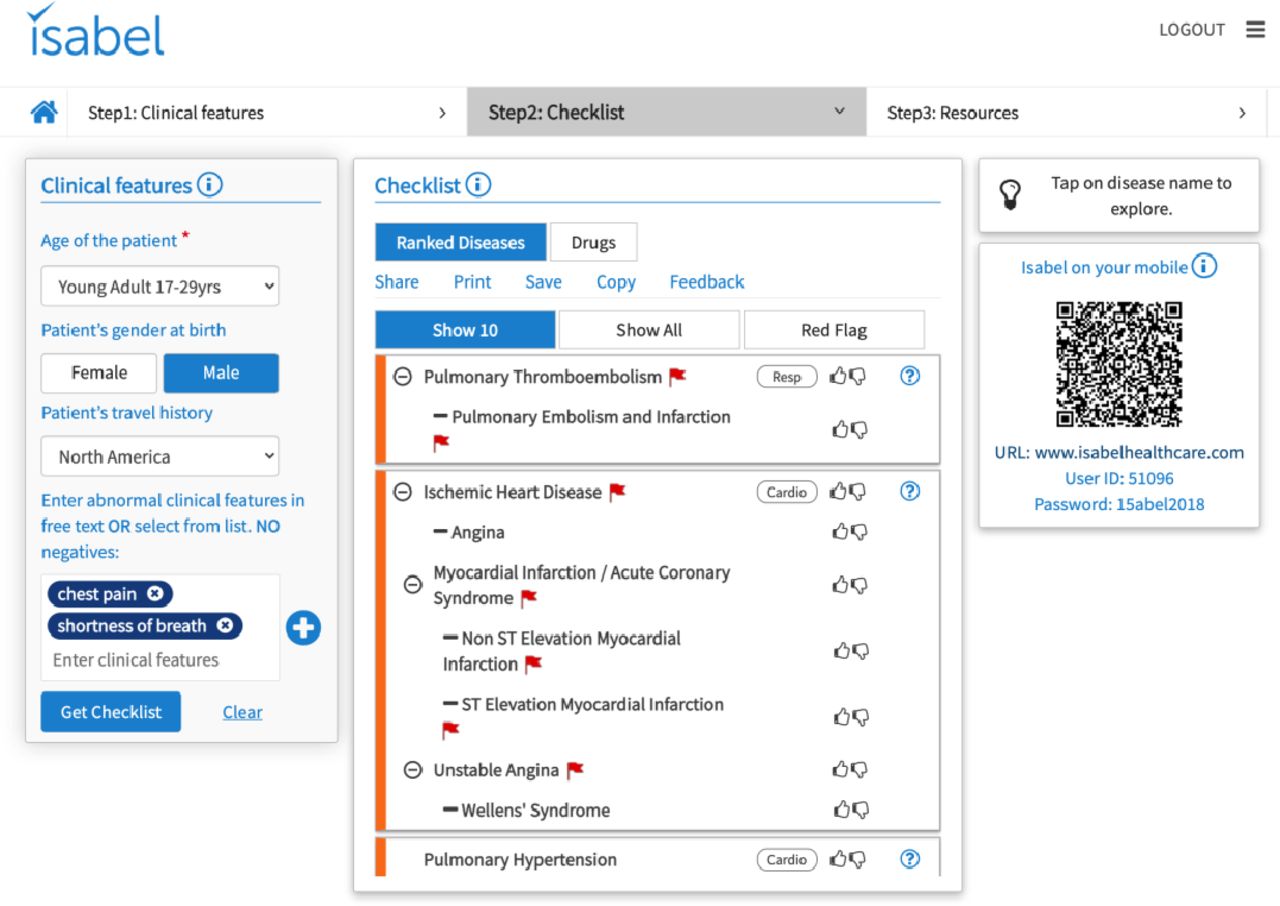
In order to use the EDS, clinicians enter patient demographics and a list of symptoms into an online platform (IsabelHealthCare.com)24 which generates a list of diagnoses to consider, annotating diagnoses that ought not be missed (figure 2). We verified that Isabel contained the correct diagnosis of all the test cases in its database.
{kind=link}
{kind=link}
Isabel interface.
Participants completed a sample case to familiarise themselves with the EDS prior to the study. Pilot work indicated that no formal training was required, as even non-medical volunteers were able to use the interface without receiving any instructions.
Outcomes
Our two principal outcomes of interest were: (1) the number of diagnoses proposed by the clinician per case and (2) presence of the correct diagnosis within the differential. The latter measure involved a binary approach, whereby the correct diagnosis (or its synonyms) being present anywhere on the list was scored as a 1 or its absence as a 0. Lists of synonyms were available from a previous study.13 For each participant, an average was calculated for both outcomes across all 16 cases. Consistent with prior work, we also scored diagnostic accuracy with two additional algorithms: a score that captures the order of the correct diagnosis in the differential as well as the presence of the correct diagnosis in the first seven items listed.13 Analysis of these approaches led to the same conclusions as the simple presence or absence score, and so they have been omitted.
We also timed each step during the diagnostic process: (1) time taken to formulate a differential based on the chief complaint, (2) time taken to revise the differential given all the case materials and (3) time taken to use the EDS.
Analysis
The analysis compared differences between participants using the EDS early or late in the diagnostic process, and across different levels of experience. The primary comparisons are shown in figure 1 labelled A, B and C. SPSS version 26 (IBM) was used for all comparisons.
Comparison A focuses on the effectiveness of EDS for the early group, examining differences between the initial differential (based on demographics and chief complaint) and a subsequent revised differential following use of EDS. Comparison B focuses on the effectiveness of EDS for the late group, examining differences between a later differential (based on all case information) and a subsequent revised differential following use of EDS. For each comparison, we performed separate repeated-measures analysis of variance (ANOVA) for the two outcomes (average number of hypotheses across all 16 cases, average diagnostic accuracy across all 16 cases) using the within-subject factor of time point (before EDS vs after EDS) and the between-subject factor of experience level (student vs resident vs practising physician).
Comparison C instead focuses on overall differences between the early group and late group by comparing their final differentials. Here we performed separate ANOVAs for the two outcomes (average number of hypotheses, diagnostic accuracy) using group (early vs late) and experience level (student vs resident vs practising physician) as a between-subject factors, and case difficulty (easy vs hard) as a within-subject factor.
Finally, we compared the average time spent using the EDS by participant between the early versus late groups using an unpaired t-test.
Effect sizes were expressed as partial eta squared, η2 , which represents the ratio of the variance attributed to the effect compared with all measured variance. Values of 0.01, 0.06, and 0.13 were interpreted as small, medium, and large effects.26 Using the Bonferroni correction for multiple statistical comparisons, a p value of <0.008 would result in rejection of the null hypothesis accepting an overall type I error of 0.95. All interactions were considered hypothesis generating rather than confirmatory27 28 using an alpha criterion of 0.05.
We performed a sample size calculation based on prior published data,13 anticipating an effect size of 0.35 for the overall benefit of EDS with respect to diagnostic accuracy. Using a conventional alpha of 0.05 and beta of 0.20, this equates to a sample size of 130 to detect a main effect of EDS. However, differences between early and late EDS use have no evidence on which to base a sample size calculation. Presuming that a relevant difference in early or late use of EDS would have to be quite substantial to meaningfully impact practice, we used an effect size of 0.50 to calculate a sample size of 64 per group using the conventional alpha and beta values. SPSS version V.26 (IBM, Redmond) was used.
Results
One hundred and ninety participants across six institutions took part in the study. Participants included 67 medical students, 62 residents in internal medicine or emergency medicine, and 61 practising internists or emergency medicine physicians. For the initial differential (ie, before participants from either group received EDS), there was no difference between the early and late groups in the number of hypotheses proposed, nor the likelihood of the correct diagnosis being present (see table 1). At this point, only 10%–13% of participants identified the correct diagnosis.
Baseline characteristics and performance of participants randomised to the early and late use of EDS groups
Comparison A: effectiveness of the EDS early in the diagnostic process
Early EDS use increased the average number of hypotheses across all experience levels from 5.64 to 7.96 (mean difference 2.32, 95% CI 2.10 to 2.49). Students showed the greatest gain, from 4.67 to 7.39 (mean difference 2.72, 95% CI 2.40 to 3.03); residents from 6.47 to 8.89 (mean difference 2.42, 95% CI 2.08 to 2.77) and practising physicians from 5.97 to 7.71 (mean difference 1.74, 95% CI 1.40 to 2.09) as shown in table 2. The main effect of time (ie, before vs after EDS) was significant (F=402, η2=0.81, p<0.0001), as was the interaction between time and experience (F=6.35, η2=0.12, p=0.003).
Outcomes of participants randomised to the early and late use of EDS groups
Early EDS use also improved the likelihood of the correct diagnosis being present in the differential from 0.12 to 0.19 across all experience levels (mean difference 0.07, 95% CI 0.06 to 0.09), with improvements from 0.10 to 0.21 for students (mean difference 0.11, 95% CI 0.08 to 0.13), 0.14 to 0.19 for residents (mean difference 0.05, 95% CI 0.03 to 0.08) and 0.12 to 0.17 for practising physicians (mean difference 0.05, 95% CI 0.03 to 0.08). The main effect of time was significant (F=110.9, η2=0.54, p<0.0001), as was its interaction with experience level (F=7.71, η2=0.14, p=0.001).
Comparison B: effectiveness of the EDS late in the diagnostic process
Late EDS use increased the average number of hypotheses from 5.30 to 6.19 (mean difference 0.89, 95% CI 0.69 to 1.10; F=117.4, η2=0.572, p<0.0001), and did not vary by experience level.
Late EDS use also increased the likelihood of the correct diagnosis being present in the differential from 0.21 to 0.30 (mean difference 0.09, 95% CI 0.07 to 0.10), with a significant main effect of time (F=112.1, η2=0.56, p<0.0001), significant main effect of experience level (F=6.19, η2=0.12, p=0.003), and a significant interaction between time and experience level (F=8.06, η2=0.16, p=0.001). Students improved from 0.13 to 0.26 (mean difference 0.13, 95% CI 0.10 to 0.15), residents from 0.25 to 0.34 (mean difference 0.08, 95% CI 0.06 to 0.11) and physicians from 0.25 to 0.30 (mean difference 0.05, 95% CI 0.02 to 0.07).
Comparison C: effectiveness of early versus late use of EDS
At the final time point, there was a trend toward more hypotheses being considered by the early group than the late group (7.06 vs 6.19; F=5.39, η2=0.028, p=0.02). This benefit was present for students and residents, but not for practising physicians (interaction with experience level: F=3.32, η2=0.04, p=0.04). However, the correct diagnosis was more likely to be present in the late group than in the early group (0.30 vs 0.25 mean difference 0.05 95% CI 0.01 to 0.08, F=7.71, η2=0.040, p=0.006). The interaction with experience level was not significant.
The main effect of hard versus easy cases on accuracy was significant (hard=0.12, easy=0.44; F=841, η2=0.82, p<0.00001). There was also a small interaction with expertise (F=10.87, η2=0.11, p<0.0001) such that, where students had greater difficulty with hard cases, but performed similarly to more experienced physicians on easy cases (data not shown).
Comparison of early and late groups on time spent using Isabel
Collapsing across both groups, participants took an average of 99 s (95% CI 67 to 130) per case to review the chief complaint and formulate a differential diagnosis, then an additional 188 s (95% CI 173 to 201) to revise this differential upon receiving the rest of the case information. As for time spent using the EDS to further revise their differential, participants took an additional 137 s (95% CI 128 to 148), but these times varied between the early and late groups: participants spent less time with the EDS when using it early in the process compared with late in the process (89 vs 189 s, mean difference 100 s, 95% CI 81 to 124, p<0.002).
Discussion
In this multicentre, randomised study, EDS improved the diagnostic process by both increasing the number of diagnostic hypotheses and the likelihood of the diagnosis being present in the differential. The effect size of EDS for both outcomes was large. While clinicians of all experience levels benefited, the impact was most pronounced among novice clinicians.
The effect of EDS on the diagnostic process was present regardless of whether it was used early or late in the diagnostic process. Timing of use did moderate the increases in number of diagnostic hypotheses and likelihood of the correct diagnosis being present. Early use of EDS resulted in an increase of more than twice as many hypotheses as late use (2.32 vs 0.89). Conversely, late use resulted in greater accuracy (ie, inclusion of the correct diagnosis) at the conclusion of the case (0.30 vs 0.25). Such findings suggest that early use of EDS serves to expand the pool of hypotheses under consideration, whereas late use of EDS is useful in helping clinicians carefully decide among alternatives. Ours is not the first study to examine differences in diagnostic support system effectiveness based on when it is used in the diagnostic process. Prior work showed improved diagnostic accuracy with use of a computerised diagnostic support system after a chief complaint and pertinent case details were provided, but not after participants had already proposed a diagnosis.29 Importantly, our study differed in asking participants to refine a differential rather than establishing and revising a diagnosis, a subtle but important distinction that may account for differences in effectiveness with late use of diagnostic support.
The increased rate of listing the correct diagnosis with EDS in this study is consistent with prior reports using other computer-based diagnostic systems.13 29 Friedman et al observed an improvement of 8% with the QMR EDS and 4% with the ILIAD EDS.13 Kostopoulou et al 29 found a 6% increase with the DxPLAIN EDS when used early in the diagnostic process. These are comparable with the 7% (early) and 8% (late use) improvements in listing the correct diagnosis seen with the Isabel EDS in this study. The larger improvement with novices was also noted in Friedman’s work with improvement in diagnostic accuracy for medical students, residents, and practising physicians of 9%, 5%, and 3%, compared with 11%, 5%, and 5% in the present study. In routine clinical practice, diagnostic error rates are estimated to be 1%–15% of all patient encounters.2 4 5 30 Improvements in diagnostic accuracy as small as 4% resulted in substantial harm reduction,31 suggesting that if the 5%–11% improvements in the diagnostic process noted in this study were transferable to routine practice, it would be meaningful.
Nevertheless, the critical difference between Isabel and the previous systems is ease of use. In the present study, average time spent with Isabel ranged from 1.5 to 3 min, whereas average times for previous systems were much longer, ranging from 22 to 240 min.13 ,32 This is not simply due to a more streamlined interface; unlike prior systems, Isabel uses a minimal amount of (primarily) historical data and yet achieves similar accuracy18–23 as previous systems that required far more information.13 29 An important implication of this efficiency is that it becomes feasible to integrate EDS into one’s processing of a case in real time.
Interestingly, different advantages with an EDS system at early and late time points are consistent with dual-process models of the diagnostic process from the fields of cognitive psychology25 and clinical reasoning.33 Elstein’s hypothetico-deductive model proposes that clinicians initially put forth hypotheses based on patient cues, then later ratify them via analytical reasoning.25 But less experienced clinicians are less likely to generate correct hypotheses34 and more easily swayed by early diagnostic suggestions35–37—a potential explanation for the disproportionate increase in diagnostic hypotheses adopted by less experienced clinicians with early EDS use. And though more experienced clinicians generate more correct hypotheses, they are still capable of diagnostic error,33 so late use of EDS may help them reconsider a common diagnosis that was initially overlooked—thereby functioning as a diagnostic checklist37 38 or a way to re-evaluate their initial impressions.39 EDS systems can help clinicians guard against search satisficing, where the first diagnosis that comes to mind is too easily accepted31 and a differential diagnosis is not generated at all.40 Even experienced clinicians may not recognise a correct diagnosis from the EDS list if they are unfamiliar with it or do not see its relevance to the case. This provides an upper bound on the utility of an EDS in practice, and an important conceptual limit in the use of EDS to improve clinician diagnostic reasoning.
Several limitations of the present study are worth mentioning. First, we used archived cases. While these were derived from actual patient presentations, the codifying of information into written form removes important steps from the authentic clinical process (eg, building a relationship with a patient, using a shared language to elicit symptoms, then interpreting this experience and integrating into a diagnostic process). This complex task competes with the use of EDS in the clinical environment, making it more difficult to use in practice than in studies. Second, whether or not adding a diagnosis to a differential will result in meaningful avoidance of misdiagnosis is still reliant on downstream clinician behaviour to appropriately investigate feasible alternative diagnoses. Clinicians may avoid investigating because of resource constraints, perceived liability or norming pressures within clinical practice groups. These influences may impair some of the benefits of an EDS-assisted approach. Future research should employ EDS in an authentic clinical environment to demonstrate feasibility in the process of care, and also assess whether this benefit with written cases persists in more authentic clinical environments. Third, we might be faulted for our choice of cases, which were designed to be difficult. In prior studies, even academic internists achieved only 40%–50% accuracy.13 We make no pretence that they are representatives of all problems in practice; quite the opposite. By selecting difficult cases, these are likely more representative of the kind of cases where physicians may seek help from an EDS. Finally, we did not involve a control group tasked with revisiting the differential diagnosis without EDS, leading to an upper limit estimate of EDS effectiveness that includes whatever benefit might be conferred by simply revisiting the differential diagnosis without EDS.
In conclusion, this study demonstrates that the integration of electronic decision support into the clinical diagnostic process across a wide range of experience increases the length of differentials and increases the likelihood of the diagnosis appearing within the differential. This benefit was observed regardless of whether the EDS system was used early or late in the process. In contrast to previous systems, current generation EDS systems are easy and quick to use, permitting easy integration into the clinical reasoning process in real time. Future research should investigate whether these benefits transfer to real-time clinical use.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval was obtained through the Hamilton Integrated Research Ethics Board, protocol #4945. All participants provided written informed consent. Access to Isabel was provided by Isabel HealthCare. The authors have no other relationship and no reporting requirements to the company.
Acknowledgments
The authors acknowledge Amy Keuhl for her role in project management, Mark Lee for his role in project management and manuscript preparation, Betty Howe for her role in platform design and recruitment.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @sibbaldmatt, @monteiro_meded
Contributors All authors contributed to study design, analysis, interpretation and manuscript preparation. MS wrote the first draft which was critically revised by all authors.
Funding This project was funded by a Physicians' Services Incorporated Medical Education Research grant.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.