Article Text

Statistics from Altmetric.com
Background
Historically hospital design was based on Florence Nightingale's nineteenth-century observations about the advantages of natural light, ventilation and cleanliness.1 Shared patient accommodation of 30 beds became the standard inpatient accommodation in hospitals globally.2 The suitability of such wards in modern hospitals is now questioned in terms of quality, safety and experience.3 Subdivisions of wards into smaller rooms and bays has become the norm, and internationally, the case is being made for more single-room accommodation in new hospital designs. Arguments for the abolition of all shared accommodation4 are based largely on the belief that patients prefer single rooms and benefit from improved patient outcomes compared with open hospital wards.5
Most current evidence derives from the USA and Scandinavia,6 and while some evidence may be transferable, variation in financial, cultural and organisational systems means that generalisation should not be assumed. The available evidence is both weak and equivocal, suggesting a range of potential benefits for patients and staff but also potential disadvantages.
Potential advantages of single-room accommodation for patients include increased patient privacy, dignity, comfort and less disruption from other patients7–9 and also enhanced patient satisfaction with communication with staff.7–10 Patients rated privacy and personal space as important but they also said that when ill they wanted nurses to be closer.11–13 Potential advantages for staff of working in single rooms include more personalised contact with patients and fewer interruptions for care delivery.14 Improved safety outcomes could include fewer medication errors,15 faster patient recovery rates7–9 and reduced infection rates.7 ,16–18 Perceived economic advantages include the potential for cost savings associated with reduced length of stay and infection rates and fewer medication errors.19 ,20
Potential disadvantages of single-room accommodation for patients include increased rates of slips, trips and falls and other adverse events through less patient surveillance,7–9 ,21 and reduced social interaction22 and patient isolation7–9 ,23 with consequent negative impacts on patients’ mental well-being and behaviour.24
Suggested disadvantages of single rooms for staff/organisations include an increase in staff walking distances (reducing time for direct care)25 and workload3; potential need for an increase in staffing levels and/or adjustments to staff skill-mix8 ,9 ,24; increase in staff stress26 ,27 and potential risks to staff through working in isolation.26–30
The international healthcare literature on the advantages and disadvantages of single-room accommodation for patients and staff is of variable quality, and some aspects have been studied more closely than others. Research on the impact of single-room accommodation on staff experiences of work and care provision is limited, the evidence does not clearly point to a preference for single rooms among patients and little is known about patient preferences across different age and cultural groups.31 There is very little evidence from well-designed research studies, and most claims are unsupported by evidence of changes in clinical outcomes; research designs are weak, typically relying on staff opinion or simple before-and-after comparisons.
Finally, it is clear that decisions around ward design are complex and trade-offs are likely to be necessary between design considerations, patient and staff preferences, changes in clinical needs/demand and economic considerations.
Objectives
We aimed to identify the impact of the move to a newly built acute National Health Service (NHS) hospital in England with 100% single rooms on staff and patient experience, patient safety and costs.
Design and methods
Study setting
In 2011, Tunbridge Wells Hospital opened, replacing old facilities (some 100 years old) at Pembury and Kent and Sussex hospitals. This was the first NHS hospital in England to have 100% single inpatient rooms in all wards. Staff and patients moved from predominantly large bays and open Nightingale wards in two phases in January and September 2011.
Design
The study was a mixed methods evaluation of the impact of the move and included a before-and-after study of patient and staff experience, a quasi-experimental before-and-after study of safety outcomes using two control hospitals, and a cost analysis. Data were collected in the new hospital between September 2012 and June 2013. A fuller report of the study and methods can be found elsewhere.6
Patient and staff experience
Trust-wide data comprised 20 pre-interviews and 21 post-interviews with senior managers (eg, director of nursing, of infection control and of therapies), clinicians (doctors, allied health professionals, ward managers), ward clerk and staff managing the move or architects/builders (see online supplementary appendix). Other patient and staff data were collected from four case study adult inpatient wards, purposively selected to encompass a range of different clinical areas and patient groups: medical assessment unit (MAU), surgical, medical (older people) and maternity. These data comprised 119 hours of structured ward observations pre and 250 hours post; 24 pre and post semi-structured ward staff interviews. The observation of practice was to understand how and where staff spent their time and determine whether the proportion of time they spent on each activity changed following the move to single-room accommodation. The researcher shadowed staff and recorded their activities on a personal digital assistant using HanDBase software in a structured time and motion data collection tool developed by the research team. This drew on a similar tool used in healthcare research designed and developed by Westbrook and Ampt32 (work observation method by activity timing) (see online supplementary appendix for observation categories). The following data were also collected in each of the four case studies: 32 pre and post semi-structured patient interviews; 55 pre and post staff surveys and pedometer data from 53 staff pre move and 56 post move. Further details can be found in the online supplementary appendix.
The structured observation, pedometer and staff survey data were entered into Excel and analysed in SPSS using descriptive and parametric statistics.6 Staff perceptions of the ward environment pre and post move were compared statistically using an unpaired t test. Travel distance data were analysed using a repeated-measures general linear mixed model (SPSS MIXED) with steps per hour as the dependent variable and pre-post new build, ward (maternity, surgical, older people, MAU), observation session (repeated measure), staff group (midwife, registered nurse (RN), healthcare assistants (HCAs)) and day of the week as independent variables. Midwives were only employed on the maternity ward, and therefore, this introduced an element of confounding. For this reason, the maternity ward was excluded from the modelling. Its exclusion resulted in an improved model fit. A sensitivity analysis to assess the effect of repeated measures on the small number of people who contributed more than one data collection session found that there was no effect and so the data were treated as a between-subjects design. The moderating effects of ward and staff group on the pre-post move were also tested by fitting these two interactions to the main effects model. F tests and adjusted means with 95% CIs have been presented.
Interviews were recorded, transcribed verbatim and analysed using a framework approach, a method that involves a systematic analysis of verbatim interview data within a thematic matrix.33 Data synthesis occurred as part of the analytical process, and connections were made between qualitative and quantitative data sources in order to identify core themes and connections.34 ,35
Safety outcomes
We recruited two control hospitals; one in which no move occurred (steady-state control) and one that moved to a new build with an increase in single rooms (but fewer than 100% single rooms) during the study period (new-build control). Patient outcomes (safety events—falls, pressure ulcers, medication errors—and hospital-acquired infections—methicillin resistant Staphylococcus aureus (MRSA) and Clostridium difficile) were collated for a 3-year period from January 2010 to December 2012 for three of the four wards (MAU, older people and general surgery) of the same type as the study site. Maternity was excluded as pressure ulcers and falls were not applicable and infection rates low. Data sources were discharge data from the patient administration system (including patient age and diagnosis) and incident reporting system for safety surveillance and infection control purposes (see online supplementary appendix). Time series were analysed by means of statistical process control charts (SPC, u-charts) to look for evidence of special cause variation associated with the move to single rooms.36 Where special cause variation was found, we further explored data to assess whether it could be attributed to the move to 100% single rooms. To attribute a change to single rooms, we explored change in case mix as an alternative explanation and looked for a similar but attenuated pattern in the new-build control where the proportion of single rooms increased. For space reasons, we report safety or infection events (eg, per falls or medications errors) per 1000 patient-days in four phases: ≥10 months before moving, 1–9 months before moving, 1–9 months after moving and ≥10 months after moving.
Costs associated with single rooms
We conducted a comparative analysis of costs associated with single rooms. To do this, we collected data on bed occupancy, administrative data on cleaning costs, nurse staffing, payroll, length of stay and build costs. Structured observation data were also analysed for proportion of time spent on direct care with patients. We modelled the impact of these costs over the lifetime of the hospital in discounted cash flow/net present value terms. In addition, 12 experts from the architecture, construction, hospital and facilities management and operations were interviewed to inform analysis on the relative impact of different hospital designs on costs and resource use (see online supplementary appendix).
Results
Patient experiences
At interview, patients in the shared accommodation wards reported enjoying the security of being very visible to staff and to each other, which resulted in good patient camaraderie for some. However, the disadvantages of shared patient accommodation included exposure to confused and disruptive patients, lack of privacy and lack of physical comfort. Four dimensions reflect patients’ overall experiences of shared patient accommodation: security, community (advantages and disadvantages), lack of privacy and lack of physical comfort. Four dimensions reflected patients’ overall experience of single-room wards: comfort, control, connection and isolation (table 1).
Patient advantages and disadvantages of shared patient accommodation and single-room accommodation
Patients experienced high levels of comfort in the single rooms and compared the hospital room favourably to a hotel or home environment allowing them to experience the comfort and control of home or a hotel, in hospital. Patients also experienced a high degree of personal control in the single room; feeling not as ‘on show’ as in shared patient accommodation. Patients in single rooms described being able to do as they pleased at any time without worrying about other patients. This was in contrast to patients’ experiences in shared accommodation.
Patients appreciated the confidentiality afforded by the single room, and the privacy and flexibility it gave for visitors. Patients rarely used dayrooms (communal social spaces) (available on two wards); they were only orientated to their room. They did not know where dayrooms were and were uncertain if they could leave their rooms. Interaction with other patients was largely absent in the new hospital, leading to a sense of isolation for some patients. Patients reported regular visits to their single room by various staff, and all patients described nursing staff conducting frequent intentional ward rounds. These nursing rounds were introduced as a method of ensuring all patients were observed and had their needs met regularly and to counter isolation in single rooms. Some patients experienced a good quality of communication and felt connected with staff; others experienced care as largely task-driven and functional, which may have enhanced the disconnection experienced by some patients.
Overall, the majority of patients (two-thirds of those interviewed) expressed a clear preference for single rooms. Privacy and en-suite bathrooms were important aspects of this. All the women in the postnatal unit liked single rooms. One-fifth of patients, including almost half the men interviewed, said they preferred multi-bedded accommodation. Staff associated loneliness with older patients, but it was experienced by patients in all age groups in this study. Single rooms were a clear preference for many patients, but a significant minority, including patients of varying ages and patient groups, wanted greater choice, either in terms of having the option of shared accommodation or being able to interact with other patients in communal spaces of the hospital. Approximately one in three patients interviewed (11 of 32) reported lack of interaction with other patients as a main disadvantage of the single room.
Staff experiences
At interview, before the move to 100% single-room hospital, staff identified the advantages of shared patient accommodation as good visibility of all patients, which facilitated surveillance and monitoring; supporting good teamwork, which was enhanced by being able to see and find staff easily that enabled staff to support each other. Staff also identified that shared patient accommodation allowed social contact between patients, which helped staff and enhanced recovery (see table 2). Disadvantages of the shared patient accommodation included an inadequate physical environment for patients and for care delivery and poor privacy, sleep and rest for patients.
Staff advantages and disadvantages of shared patient accommodation and single-room accommodation
Following the move, staff reported that single rooms improved privacy, dignity and confidentiality for patients and were better for visitors. Single rooms were perceived to facilitate communication with patients, with reduced interruptions and allowed more personalised care. The single rooms provided an improved working environment for care delivery, being modern, clean and spacious, and the en-suite bathrooms made personal care easy to deliver. Staff also noted the improved ward layout and felt the single-room environment reduced the risk of infection (table 2).
Analysis of pre-move and post-move survey data found staff perceived statistically significant improvements in the efficiency of the physical environment, the patient amenity, the effect of the environment on infection control, patient privacy, and family and visitors. The largest increases were found for perceptions of infection control and patient privacy (see table 3). The new wards were perceived by staff to support good hygiene practices; however, there was a perception by infection control staff that single rooms induced a degree of complacency in relation to basic precautions and there was a perceived need to reinforce infection control procedures and protocols. Basic infection control principles were revisited to counter the belief that single rooms protected from hospital-acquired infections. Perceptions of the effect of the single-room environment on teamwork and staff's ability to deliver high-quality care were significantly more negative after the move than before (see table 3).
Results of t tests comparing staff perceptions of the ward environment pre and post move
Staff rated the post-move single-room accommodation as significantly lower for their ability to deliver high-quality care (table 3). A notable disadvantage that staff highlighted at interview was the reduced visibility offered by the single-room design, making patient surveillance difficult. Staff identified various obstacles to safe and efficient working, one unique to this particular hospital design (in-board bathrooms that protrude into corridors obscuring views into more than one room at a time). Staff saw their greatest challenge as monitoring and keeping patients safe, especially those at risk of falls. Although staff found the initial increased rate of falls distressing, their rating of patient safety in the survey was not significantly different from pre move (table 3). All staff interviewed perceived a lack of visibility of patients in the single-room wards had contributed to an initial increase in falls in the new hospital. Experienced nursing staff felt it easier to prevent falls in shared patient accommodation because they could ‘keep an eye’ on patients and were more aware of warning signals, for example, patients attempting to get up from their chair or bed. Nurses had to work differently and adapt their working practices to ensure all patients were seen regularly, requiring teamwork with colleagues and the initiation of regular hourly intentional rounds. Other successful examples of new ways of working included supervisory roles for situation awareness; falls interventions and starting a lunch club in a shared social space for patients on the older people's ward to combat isolation and improve food intake at lunchtimes. Nurses found time management and prioritisation of workloads challenging in the new environment and struggled to divide their attention between all the patients they were caring for (they had found this easier in shared patient accommodation). Staff recognised that they required different strategies to enable them to divide their time between patients and feel satisfied that they were giving all patients sufficient personalised care (again easier on multi-bedded wards), but this challenge had largely been left to individuals to resolve, with reportedly limited success and associated dissatisfaction (table 2). Trial and error was a feature of innovations, with staff teams trying, for example, different ways of preventing falls and different configurations of decentralised teams.
Social isolation was perceived by staff to be a real disadvantage for both staff and patients. Staff also felt that the quality of teamwork they had enjoyed on shared accommodation wards was difficult to recreate. Nurses described seeing less of their colleagues, being unaware of what was happening in other parts of the ward and sometimes feeling isolated. Patients were nursed in three groups of 10 patients by sub-teams of nursing staff. Staff adapted to these decentralised nursing teams, but information exchange within wider nursing teams was perceived to be worse. Locating colleagues to obtain assistance was one of the main difficulties described by staff and was largely unresolved by new ways of working and by use of communication technology (table 2).
Pedometer data showed an increase in the mean number of steps per hour for all wards and staff groups (table 4).
Mean steps per hour by wards, pre/post move and staff group
The modelling, which adjusted for ward, staff group and day of week, showed a significant increase from a mean of 716 (95% CI 660 to 771) before the move to a mean of 839 (95% CI 787 to 892) after the move (F(1, 83)=10.36, p=0.002). HCAs (mean 836, 95% CI 776 to 895) walked significantly further than RNs (mean 719, 95% CI 667 to 772, F(1,83)=8.01, p=0.006), but there was no significant difference between wards in the distance walked (F(2, 89)=2.38, p=0.099). The effect of the move was not moderated by either ward (F(2,82)=0.64, p=0.53) or staff group (F(1,76)=3.48, p=0.066).
Analysis of the time and motion observation data showed an increase in the proportion of direct care, indirect care, professional communication and medication tasks and a decrease in ward-related activities such as cleaning and bed-making, but none of these were statistically significant. There were, however, fewer interruptions during tasks and work was less fragmented. There were no significant differences in staff well-being and stress post move.
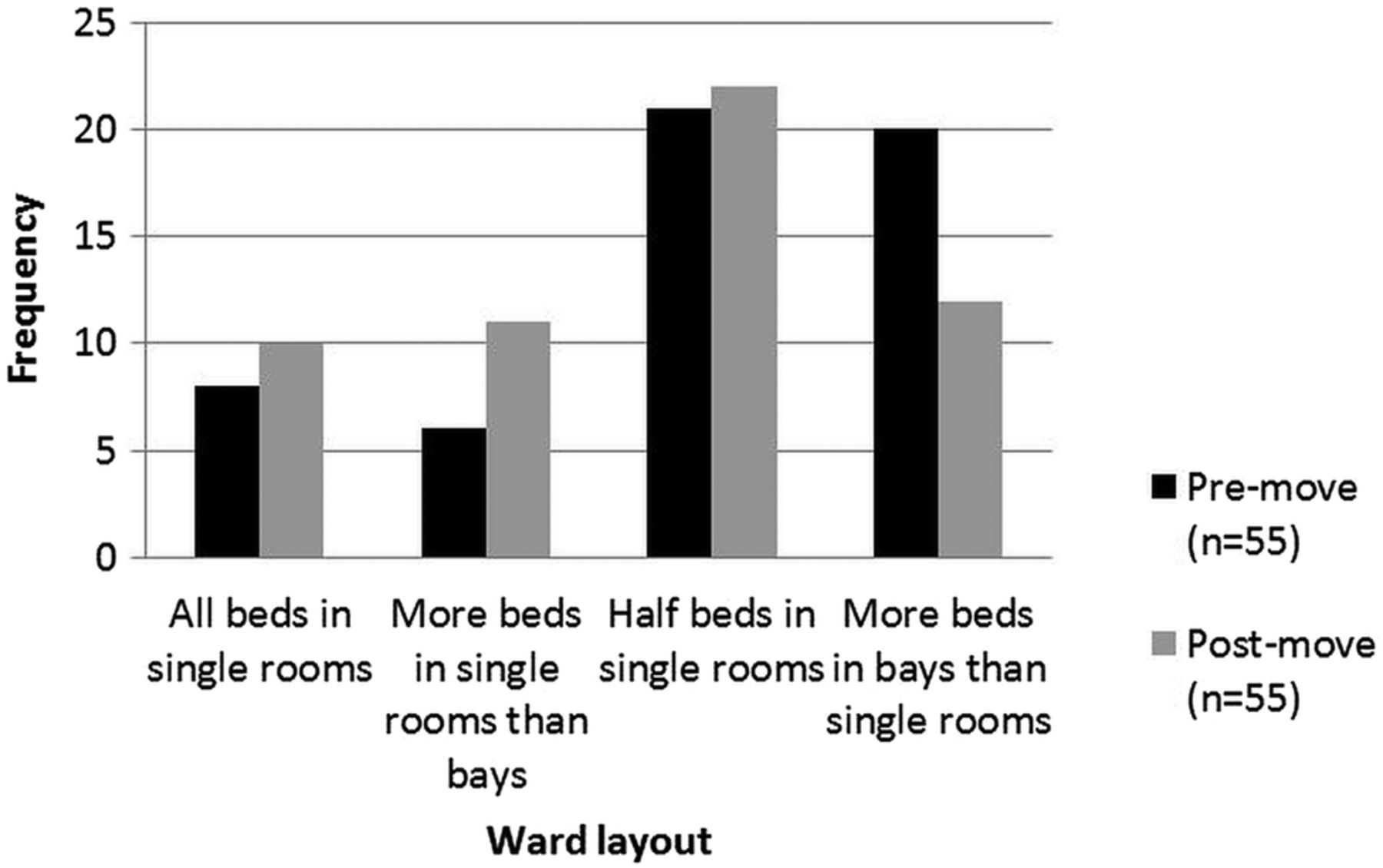
Overall, when asked their preference, most staff said they would prefer wards with a mix of single rooms and multi-bedded accommodation both before and after the move. After the move, only 18% (n=10) of staff indicated a preference for 100% single rooms (figure 1). The most common preference, before (38% n=21) and after (40% n=22) the move, was a combination of 50% of beds in single rooms and 50% in bays. More staff in the pre-move survey reported a preference for more beds in bays (36%, n=20) than in the post-move phase (22%, n=12).

{kind=link}
Nurse preferences for single-room or multi-bed accommodation.
Impact on patient safety
There were few changes in safety outcomes that might be attributed to the move to single rooms. Only 5 of 15 SPC charts across the 5 outcomes from 3 wards at the single-room hospital showed special cause variation following the move (bolded in table 5). Increases of falls and medication errors in the MAU immediately following the move were found but rates decreased to previous levels 9 months after the move. No equivalent change was observed in the ‘new-build’ control hospital. Increases in C. difficile infection, falls and pressure ulcers post move were observed in the older people's ward. Again, no equivalent change in outcomes was observed in the new-build control hospital. However, a reduction of about 50% in length of stay (LOS) indicates a substantial change in case mix on the older people’s ward and so these outcomes could not clearly be attributed to the move or the environment.
Safety and infection control outcomes before and after the move
Although nurses perceived increased falls as a ‘single-room issue’ because of diminished visibility, the temporary nature of the increase in Tunbridge Wells Hospital and lack of a similar pattern in the new-build/mixed accommodation control site suggest that the observed adverse outcomes are not directly associated with single rooms. One explanation might be the disruption from the move to a new environment and the need to adjust work patterns, before patterns of falls settled down again. Our staff interview data suggest some of the necessary adaptations that were made in the 100% single rooms (eg, use of technology, non-slip socks and improved assessment to prevent falls). To minimise falls, the rooms had non-slip flooring and in-board bathrooms with bathroom doors on the bed head wall with hand rails (to prevent falls risk by patients walking across an open floor to get to the bathroom). However, as outlined above, the in-board bathrooms meant that staff sight lines were limited to one patient.
Impact on costs
An all-single-room hospital requires more floor space for wards, but space requirements for other areas are the same. Interviews with architects and construction experts suggested that the cost of building an all-single-hospital in the UK is probably no more than 5% higher than a 50% single-room hospital. There was no evidence of difference in maintenance costs per square metre, nor of an increase in the cost of preparing and serving meals related to single rooms. We modelled the cleaning costs for a 500-bed hospital with a 100% and 50% single-room design (table 6). Total annual costs for cleaning ward areas were 53% higher in the all-single-room design and added approximately £1050 per bed per year for cleaning. For a Trust with approximately 500 beds, this cost would be approximately 0.14% of annual budget. We analysed the impact of a number of other costs, such as catering, falls, length of stay and infections.37 However, it was impossible to attribute any observed differences to a ‘single-room effect’, and these are not therefore included here.
Comparing nurse staffing data in the 19 months before and after the move up to March 2013, there was an overall increase in whole time equivalent (WTE) for nurses and also a change in the skill mix of staff (a slight increase in proportion of RNs). Overall, under the planned investment at Tunbridge Wells Hospital, there was a 0.9% decrease in beds (from 791 to 784 beds), a 3% increase in WTE staff (from 1793 to 1847 WTE) and a 2.7% increase in total staffing costs (from £60 878 000 to £62 548 000). Attributing how much of the planned investment was the result of a ‘single-room effect’ is, however, not possible. In some areas, including maternity, the changes were part of an overall review of nursing levels and the general restructuring of patient pathways. While there may have been some impact on operational costs arising from increased numbers of staff, this is partially due to the change in number of beds, the cost of staff time and change in the skill mix of staff. There is an opportunity cost associated with time spent walking; this time is not available for other activities such as spending time with patients or administrative activities.
Impact on costs
Discussion
A disadvantage of single rooms for approximately a third of patients was a sense of isolation and loneliness confirming a recent survey in Scotland.38 Patients missed opportunities for interaction with other patients, confirming previous findings.7 ,9 ,23 Patients and staff noted the potential for loneliness, boredom, loss of shared experience and absence of distraction and social interaction offered by multi-bedded wards. Dayrooms were rarely used, and patients were only orientated to their rooms. However, on balance, most patients in our study preferred single rooms. Comfort, control, privacy and en-suite bathrooms were important aspects that influenced this preference.
Nurses needed to adapt their working practices significantly and felt ill prepared for working on single-room wards, resulting in trial and error of new approaches to care. Staff walking distances increased, and a number of aspects of care, including providing adequate surveillance, were challenging. Staff preference remained for a mix of single rooms and bays, and our findings suggest that a move to all single rooms may have significant implications for the nature of teamwork in the longer term, confirming evidence that suggests 100% single-room facility design made team communication and patient monitoring difficult, and that it limited social interaction among staff.39
Our findings suggest single rooms have implications for teamwork and informal learning (ie, observing how colleagues handle situations/role modelling), something not previously identified in the literature. Future research is needed to explore different room designs and ward layouts and consider the long-term impact of single-room working on staff, including the nature of teamwork and informal learning.
Staff interviews highlighted concern about loss of panoptic surveillance of patients, which was seen as a major disadvantage of the new wards, and linked to the perception that falls had increased because of single rooms. While our results suggested that any increases in falls could be explained by changes in case mix, previous evidence suggests single rooms could mean less surveillance by staff and increased rates of slips, trips and falls40 ,41 and falls that are unnoticed by staff or other patients.8 ,9 ,21 Restricted line of sight into the room and the linear ward layout may have increased walking by nursing staff and reduced efficiency, which confirms other research.42 With a different design (eg, observation points and large glazed windows and doors), such adverse effects on staff-to-patient observation might be mitigated.9 Design features of wards with single rooms and technology need to be maximised to ensure that privacy and comfort for patients does not compromise staff's ability to monitor them.
The temporary nature of falls increases, and lack of a similar pattern in the control wards, which also experienced an increase in single rooms, suggests that it is not an inevitable result of single rooms. This conclusion must also be interpreted in the light of an overall increase in falls at the hospital level associated with changing patient-level risk factors (an increase of comorbidities associated with service reconfigurations). While we did see a sustained increase in falls in the older people's ward, a strong correlation between changes in the fall rate and in patient-level risk factors associated with service reconfigurations makes it difficult to conclude that single rooms are the cause. However, the possibility that some groups, such as older people, are adversely affected cannot be discounted.
The discrepancies between patient and staff views in terms of preference for single rooms are notable; on balance, two-thirds of patients we interviewed preferred single rooms while only 18% of staff indicated a preference for 100% single rooms. Most staff said they would prefer a mix of single rooms and multi-bedded accommodation, to allow them more panoptic surveillance of very sick and frail elderly patients in particular. A mix of accommodation that allows flexibility or accommodation that can be changed to adapt to patient needs, with sliding glass walls for example, may be a solution. Key for patients was access to an en-suite bathroom, which for many tipped the balance in favour of single rooms, despite some patients experiencing loneliness and isolation. If future innovation in single-room design can enhance visibility for staff, while maintaining access to en-suite bathrooms and facilitate more communal spaces for patients to interact, then staff and patient preferences may become more closely aligned.
Strengths and limitations
Studying one specific hospital in depth through four case study wards provides rich in-depth data generating important learning for future new hospital builds. Sampling four different wards provides a range of ages; conditions, hospital length of stay and a range of contexts in which to understand staff work experiences and patient experiences of care. However, we were not able to interview patients who were very sick or who had dementia or delirium and we did not interview carers/relatives.
The 152-item survey was designed specifically for this study. Apart from the adapted Teamwork and Safety Climate Survey and some staff well-being questions from the NHS staff survey, the survey was, however, not standardised. Items were generated by reviewing the literature and a pool of potential items were reviewed and revised by a group of health services researchers and pilot tested with a group of 20 nurses. Our controlled before-and-after design provides weak causal inference, but our cautious approach—use of SPC charts within units followed by close scrutiny of other sources of data, including case mix, to assess whether cause was plausible and likely—means that we are unlikely to make incorrect attributions. This is in stark contrast to most previous studies where simple before-and-after comparisons have been used. We used aggregated routine data without individual risk adjustment for patient safety because of the available data (monthly reports of rates), and so a regression-based analysis with individual risk adjustment was not possible. While such routine data are problematic because of coding and reporting bias, our approach to analysis, a time-series-based approach at unit level, using SPC charts, was most appropriate for the data we were able to collect43 and protected against many potential biases.
We could not make a causal link between single-bed rooms and changes in the rate of falls, so the cost of falls was not included in the economic analysis, although we recognise that these costs are potentially high. As noted above, differences in healthcare resourcing, cultural and workforce expectations and organisational systems mean it should not be assumed that our findings are necessarily generalisable to other countries.
Conclusion
This study is one of very few to have examined in depth the experiences of patients and staff in single-room hospital accommodation and provides valuable evidence to guide policy, planning and hospital design. Based on our data, there appear to be no strong economic or safety reasons for choosing 100% single rooms in the UK. Our findings suggest it would be beneficial for managers planning a similar move to encourage staff to prepare and rehearse for working in single rooms, to plan for a possible increase in nurse staffing, to review and reinforce infection control and falls policies for single-room working and to actively manage and monitor changes in work practices and inpatient experiences before and after any changes. Nurses in our study preferred a mix of single rooms and shared patient accommodation. The majority of patients in our study preferred single rooms, but consideration needs to be given to the minority of patients who experienced isolation in single rooms as well as those very sick patients and frail older people, including those with dementia and delirium whom we did not interview. The possibility that some groups, such as frail older people, are adversely affected cannot be discounted. It is therefore important to give careful consideration to the likely patient population when thinking about the mix of accommodation types in other new hospital builds.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Correction notice This article has been corrected since it was published Online First. Table 5 title has been corrected.
Contributors JM led the overall study design, led and undertook data collection, analysis, final report writing and preparation of this manuscript . PG contributed to overall study design; led the comparator study design and analysis, contributed to report writing and gave final approval of manuscript. CP contributed to overall study design, led and conducted data collection and analysis of case study qualitative data, contributed to report writing, and gave final approval of manuscript. MS conducted data collection and analysis of comparator study, drafted that section of this paper and gave final approval of manuscript. JEA contributed to overall study design, led the case study quantitative analysis and report write up and gave final approval of manuscript. GR contributed to overall study design and report write up and gave final approval of manuscript. EP conducted data collection, analysed and wrote up the costing study with JB, and gave final approval of manuscript. JH undertook additional data analysis of case study qualitative data, contributed to report write up and gave final approval of manuscript. TM contributed to overall study design, quantitative analysis and report write up and gave final approval of manuscript. JB contributed to overall study design; worked with EP on the cost study design, analysis and write up, contributed to report writing and gave final approval of manuscript.
Funding Department of Health–National Institute for Health Research–Health Services and Delivery Research (HS&DR) Programme 10/1013/42.
Competing interests None declared.
Disclaimer The views and opinions expressed are those of the authors and do not necessarily reflect those of the [Health Services and Delivery Research Programme], NIHR, NHS or the Department of Health.
Ethics approval King’s College London Psychiatry, Nursing and Midwifery Research Ethics Committee (PNM/09/10-30).
Provenance and peer review Not commissioned; externally peer reviewed.