Article Text

Abstract
Background Pharmacists’ completion of medication reconciliation in the community after hospital discharge is intended to reduce harm due to prescribed or omitted medication and increase healthcare efficiency, but the effectiveness of this approach is not clear. We systematically review the literature to evaluate intervention effectiveness in terms of discrepancy identification and resolution, clinical relevance of resolved discrepancies and healthcare utilisation, including readmission rates, emergency department attendance and primary care workload.
Methods This is a systematic literature review and meta-analysis of extracted data. Medline, Cumulative Index to Nursing and Allied Health Literature (CINAHL), EMBASE, Allied and Complementary Medicine Database (AMED),Education Resources Information Center (ERIC), Scopus, NHS Evidence and the Cochrane databases were searched using a combination of medical subject heading terms and free-text search terms. Controlled studies evaluating pharmacist-led medication reconciliation in the community after hospital discharge were included. Study quality was appraised using the Critical Appraisal Skills Programme. Evidence was assessed through meta-analysis of readmission rates. Discrepancy identification rates, emergency department attendance and primary care workload were assessed narratively.
Results Fourteen studies were included, comprising five randomised controlled trials, six cohort studies and three pre–post intervention studies. Twelve studies had a moderate or high risk of bias. Increased identification and resolution of discrepancies was demonstrated in the four studies where this was evaluated. Reduction in clinically relevant discrepancies was reported in two studies. Meta-analysis did not demonstrate a significant reduction in readmission rate. There was no consistent evidence of reduction in emergency department attendance or primary care workload.
Conclusions Pharmacists can identify and resolve discrepancies when completing medication reconciliation after hospital discharge, but patient outcome or care workload improvements were not consistently seen. Future research should examine the clinical relevance of discrepancies and potential benefits on reducing healthcare team workload.
- medication reconciliation
- pharmacists
- primary care
- transitions in care
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
There is growing policy interest in improving the safety of transition between different health service locations or settings.1–4 Transitions include admission to hospital from the community, transfers within secondary care and discharge back to the community. Safe transitions often require coordinating care with healthcare professionals in both primary and secondary care and providing patients with accessible information on post-transition care.5 One area where these actions are crucial is in communicating medication information. Harm from prescribed or omitted medications is higher after discharge, and effective medication reconciliation has been promoted as one way to improve safety.1–4 6–8 Multiple definitions of medication reconciliation exist, but all involve defining the list of medications the patient should be taking, altering records to reflect changes and ensuring patients and/or carers are aware of the changes.1–3 9
At the transition from hospital to community, medication reconciliation is necessary for hospital-initiated medication changes to be maintained. The medication taken by patients in the community, and prescribed by their general practitioner or primary care physician (from now on both termed GP), is often changed during hospital admissions.10 On discharge, a document is sent to the patient’s GP, and sometimes their community pharmacist, detailing medication regimen changes implemented during their inpatient stay. Medication reconciliation ensures the list held by the GP or community pharmacist (preadmission medication) is updated to reflect hospital-initiated changes. Following this process, discrepancies that exist between the primary care list of medications and the discharge medication list are either intentional discrepancies (a conscious decision has been made not to implement changes) or unintentional.
From the perspective of the UK, models for providing primary healthcare are changing. As in many sectors of healthcare, the roles of pharmacists (and other health professionals) are being extended.11 Completion of medication reconciliation by community pharmacists (whose traditional role is medication dispensing) and primary care pharmacists (employed by primary care organisations) has been prioritised.12 13 It is assumed this will increase the safety of care after discharge, improve outcomes such as readmission rate and have workload benefits by freeing clinical time for GPs. While in secondary care improvements in patient outcomes of this type of intervention have been reported, effectiveness in the community has not been established.7 A previous systematic review that examined all interventions to improve medication reconciliation in primary care found two studies that evaluated medication reconciliation after hospital discharge by pharmacists.14 These were of low quality and evidence of benefit was not found. A further systematic review evaluated all interventions (including medication reconciliation) undertaken by pharmacists in the community after hospital discharge.15 This showed that pharmacists can identify potential drug-related problems, but the impact on outcomes, such as healthcare utilisation, was inconsistent.
We aimed to focus, in depth, on medication reconciliation performed by community and primary care pharmacists after hospital discharge, by systematically reviewing published studies that compared this process with usual care. The aim was to determine the effectiveness of this intervention on overall discrepancy identification and resolution, the clinical relevance of resolved discrepancies and healthcare utilisation in terms of readmission rates, emergency department attendance and primary care workload.
Methods
The study was conducted using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) group guidelines.16 The completed PRISMA checklist is included as an online supplementary file
Supplementary file 1
Scope of the review
Studies were included that compared community and primary care-based pharmacist-led medication reconciliation with usual practice. We defined medication reconciliation as the reconciliation of preadmission and postadmission lists of medication. Many studies evaluated interventions that included medication reconciliation combined with other actions. Studies where drug-related problems (such as drug interactions) were identified and corrected were included,17 but studies focused on medication review (eg, recommendations to optimise medication regimens) were not.18 Randomised controlled trials (RCTs), cohort studies and pre–post intervention studies were included.
Information sources
We searched the Medline (Ovid), Cumulative Index to Nursing and Allied Health Literature (CINAHL) (EBSCOhost), EMBASE (Ovid), Allied and Complementary Medicine Database (AMED) (Ovid), Education Resources Information Center (ERIC) (Ovid), NHS Evidence, Cochrane electronic databases and Scopus databases from inception until 1 September 2017. The reference lists of selected studies were hand-searched to identify any additional relevant studies. Citations were imported into RefWorks and all versions of citations lists were kept.19
Search strategy
To identify studies pertaining to our definition of medication reconciliation, a combination of medical subject heading terms and free-text search terms was developed by the review team in collaboration with a knowledge manager, a qualified librarian whose role includes searching and accessing published healthcare evidence. To identify studies describing medication reconciliation, the search terms ‘medication reconciliation’, ‘medicines reconciliation’, ‘medication discrepancy’, ‘medication error’, ‘medication adherence’ and ‘medication counselling’ were combined. Search terms to identify studies at discharge from hospital included ‘discharge’, ‘transition’ and ‘patient transfer’, and terms to identify pharmacists included ‘pharmacist’, ‘pharmacy’ and ‘community pharmacy’. To identify studies set in the community rather than in hospital, several terms were combined, including ‘primary health care’, ‘ambulatory care’, ‘family practice’, ’general practitioner’ and ‘home care services’. No limit was placed on date of publication or language, and the search was adapted for each database. The final search syntax for Medline is available as an online supplementary file.
Eligibility criteria
For inclusion, studies had to fulfil the criteria in table 1. Following removal of duplicates, two reviewers independently screened titles and abstracts of all citations (DM and MR). Full texts of all articles considered to be relevant were obtained and screened by two reviewers independently (DM and MR). Disagreements were resolved by discussion of full article content with the remaining reviewers.
Study inclusion criteria
Data extraction
Once the final set of studies was agreed, the lead reviewer (DM) extracted data from all studies. A second data extraction was completed independently by another member of the review team. A template was created to allow collection of data relevant to the study questions. This was piloted with two studies and adapted following discussion of extracted data by the review team. The data extracted comprised details of the authors, publication, funding, aims, study design, inclusion and exclusion criteria, method of allocation to intervention or control group, sample sizes, participant characteristics, setting and details of the intervention, statistical techniques used, outcome data, and reported strengths, weaknesses and conclusions.
Study details were tabulated to codify the study design, type of pharmacists, setting of intervention, number, timing and duration of contacts, and the description of collaboration with other team members. The outcome data that were extracted from each paper were rates of identification and resolution of discrepancies; rates of resolution of clinically relevant discrepancies; and measures of healthcare utilisation (rates of readmission, emergency department attendance, GP attendance and measures of healthcare team member workload).
Risk of bias
The quality of each study and risk of bias were assessed independently by the two reviewers who performed the data extraction using the relevant Critical Appraisal Skills Programme (CASP) tools.20 These checklists facilitate a systematic approach to considering the presence or absence of certain elements within the study that may cause bias. Following completion of the CASP tool, the two reviewers discussed their findings for each study and graded the risk of bias as low, moderate or high. For example, one section asks: ‘Were controls recruited in an acceptable way?’ Selection bias may be introduced if participants are not randomised but could select allocation to the intervention or control group. Studies that recruited control groups in this manner would be deemed to have a higher risk of bias.
Data synthesis and analysis
Studies were grouped into RCTs, case–control studies and pre–post intervention studies. Other than for readmission rate, meta-analysis of outcome data could not be performed due to lack of data, heterogeneity of data and method of reporting outcome. To synthesise discrepancy rate resolution and healthcare utilisation data, outcomes were compared narratively with the appraised risk of bias of each study defined by the weight given to findings.
Meta-analysis of readmission data was performed by calculating the Mantel-Haenszel risk ratio (RR) and 95% CIs. As interventions in the included studies varied, it was thought that there would not be one ‘true’ effect size; therefore, a random-effects model was used within the Cochrane Review Manager (RevMan) V.5.3 software to synthesise results by constructing a forest plot.21 For studies that reported outcomes over different durations, the longest follow-up period for which all data were presented was used for analysis. Statistical heterogeneity was assessed by calculating τ2, χ2, I2 and P values. Publication bias was evaluated by construction and inspection of a funnel plot.
Results
The electronic database search identified 3220 citations, with four more identified from the reference lists of included studies. After removal of duplicates, 1610 citations remained. Following title and abstract review, 157 publications underwent full-text review. Fourteen studies met the inclusion criteria (figure 1).
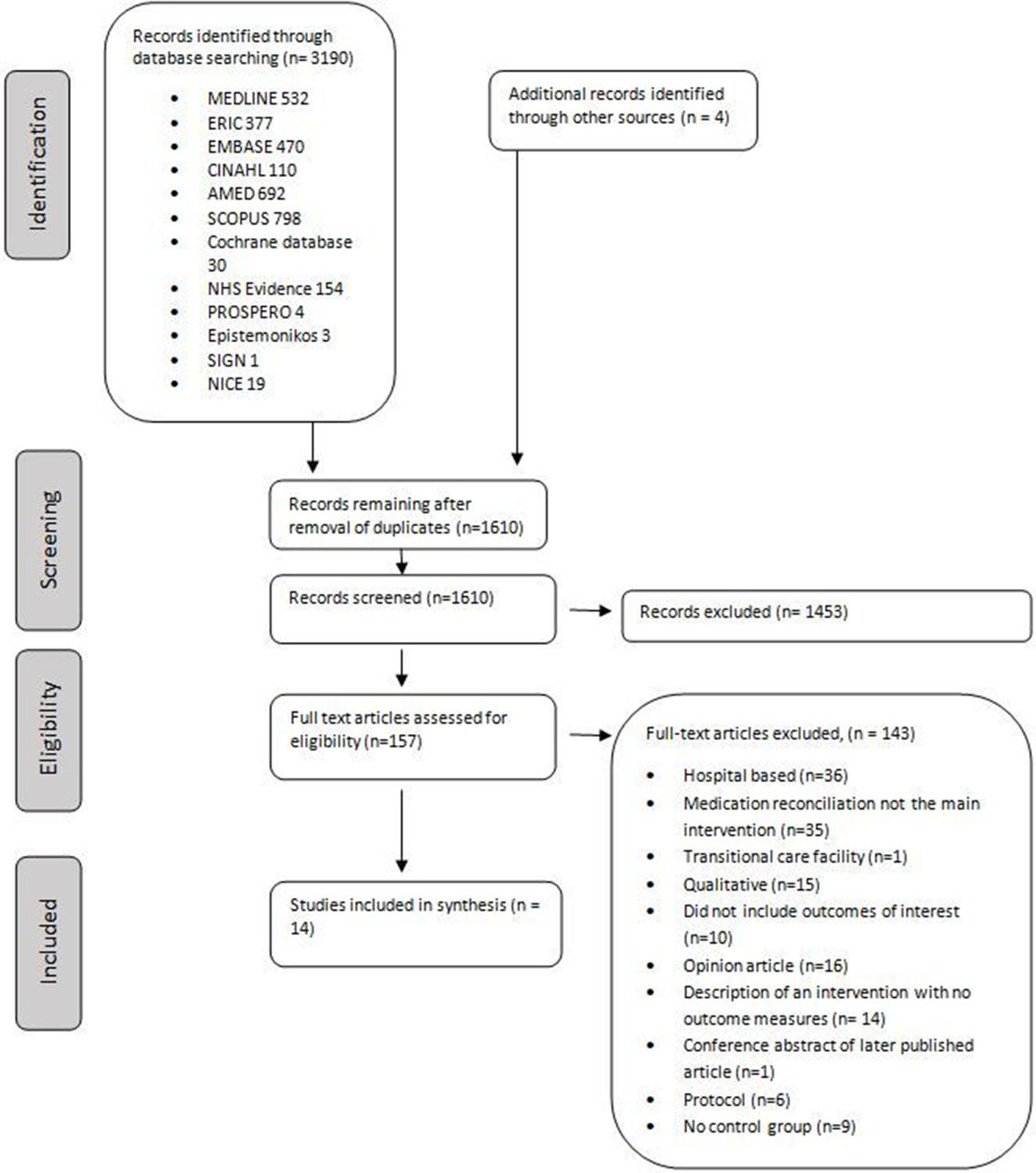
PRISMA flow diagram of selection of eligible studies. NICE, National Institute for Health and Care Excellence; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; AMED, Allied and Complementary Medicine Database; ERIC, Education Resources Information Center; CINAHL, Cumulative Index to Nursing and Allied Health Literature.
Characteristics of included studies
Five included studies were RCTs, six were cohort studies, two were pre–post intervention studies and one was a quality improvement (QI) project that presented a run chart detailing pre–post intervention data (table 2). Two studies17 22 were deemed to have a low risk of bias. Although they were not blinded, both studies were RCTs and described robust randomisation techniques to intervention or control group that otherwise received similar care. All significant results were presented and treatment effects were presented in a precise manner. Eight studies were deemed to be of moderate risk of bias.23–30 RCTs in this group had less robust randomisation,24 25 had low numbers25 and were unable to account for all patients who entered the study (one24 reported a large dropout rate, and another25 had several patients who were unable to be reached by telephone for follow-up). Cohort studies in this group had robust methods to select controls and presented relevant data in a precise manner.26–29 Four studies had a high risk of bias.31–34 These studies had less robust methods for assigning patients to intervention or control groups,31 32 or did not present all information on group allocation.33 34
Description of study and intervention characteristics including collaboration between pharmacist and GP of included studies
Sample sizes ranged from 61 patients25 to 829.17 Interventions varied by the patient group targeted, the setting within which it was completed, and the timing and number of contacts. Most studies targeted those considered at higher risk of readmission either through age17 22 30 32 or presence of a long-term condition.25 28 Five studies evaluated medication reconciliation undertaken by the pharmacist in the patient’s home,17 22 26–28 whereas in three studies medication reconciliation was performed with the patient at a primary care clinic appointment.23 25 30 In one study, medication reconciliation was completed by telephone,33 and in another, reconciliation was performed either at a home visit for those with high risk of medication-related problems or by telephone for those with moderate risk.31 Two were set in nursing homes29 34 and one in a community pharmacy.24 In two studies medication reconciliation was completed in the absence of the patient.24 32
In seven studies patients were contacted once,25–29 33 34 in two studies twice,17 23 and in three studies the number of contacts varied dependent on patient preference and perceived need by pharmacists.22 30 31 Medication reconciliation was completed 2 days before hospital discharge to the nursing home in one study.34 Six studies contacted the patient within the first week of discharge25 27 29–31 33 and four in the second week.17 22 23 26 In seven studies, pharmacists discussed outcomes of medication reconciliation with other team members such as the GP or nursing staff,22 25 26 30–33 whereas in four a written report was produced for other clinical staff.17 23 27 28
Effectiveness of identification, resolution and clinical relevance of discrepancies
The identification and resolution of discrepancies by pharmacists completing medication reconciliation was compared with usual care in four studies.24 25 28 32 In all four studies, rates of identification and resolution were greater in the intervention group (table 3).
Two studies compared the clinical relevance of resolved discrepancies between intervention and control groups and suggested that there was the potential for fewer adverse drug events after pharmacists had completed medication reconciliation (table 3).24 29 Seven studies described the type of discrepancy found when pharmacists perform medication reconciliation (such as drug–drug interaction identified) but did not describe the clinical relevance.25–28 31 32 34
Identification, resolution and clinical relevance of discrepancies and reported healthcare utilisation
Healthcare utilisation
Healthcare utilisation was reported in 12 of the included studies. The different outcome measures reported included readmission rate at 1, 3, 6 and 12 months, emergency department attendance, and additional GP and secondary care consultations (table 3). Three studies reported a statistically significant reduction in readmission rate,25 31 33 whereas one reported an increase in readmission rate.17 Data from seven studies were included for meta-analysis. One study was excluded as only admissions related to myocardial infarction or coronary revascularisation were included,23 another as the number of days hospitalised (rather than readmission rate) was reported28 and three more were excluded as they did not report numbers of patients readmitted.29 33 34 One of these33 reported a reduced readmission rate, whereas the others29 34 reported no change. Two studies reported readmission rates over different time scales.22 27 In one study the longer time scale was used.27 The shorter time frame was used in the second study as the composite readmission rate over the longer time frame was not clear. The pooled RR across all included studies (total number of patients=2336) was 0.91 (95% CI 0.66 to 1.25), indicating no clear effect on readmission rate (figure 2). There was a high degree of statistical heterogeneity. As few studies were included, I2 is the most suitable statistic for assessing the impact of heterogeneity. An I2 value of 71% and P=0.002 were calculated, indicating high heterogeneity.35
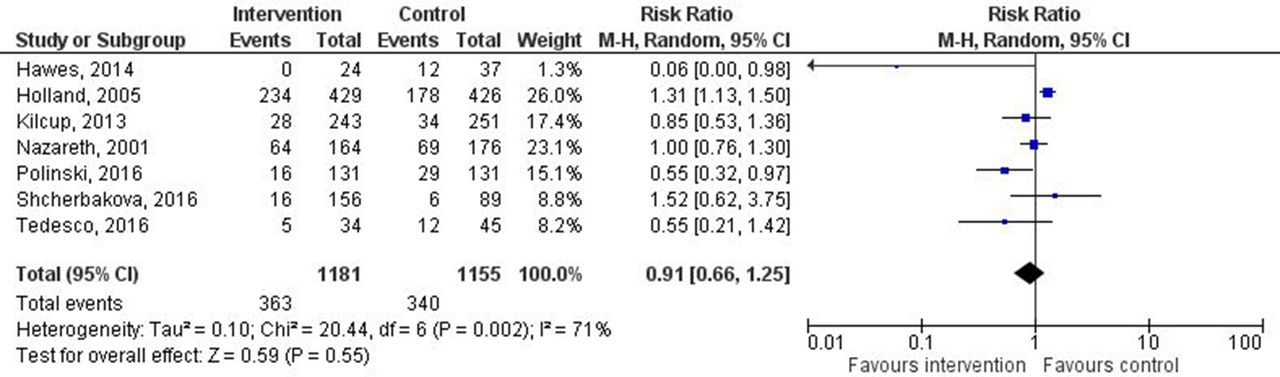
Forest plot of intervention effects on the proportion of patients with all-cause readmission. Diamond represents pooled estimate of relative risk calculated using Mantel-Haenszel (M-H) random effects model and 95% CIs. Squares represent study weighting, and horizontal bars represent 95% CI.
Emergency department attendance rate was measured in three studies.25 26 34 No difference was observed between intervention and control groups in two studies,26 34 whereas in one a large reduction was found and this was a small RCT with a moderate risk of bias.
One study17 reported an increase in GP visits of 43% in the intervention group, while another reported no significant difference in GP attendance.22 Two studies reported that pharmacist completing medication reconciliation had the potential to free up clinical time for other healthcare team members. One reported that 2 hours of pharmacist time freed 3 hours of nursing time and 1 hour of physician time,34 and the other stated that planned and unplanned physician visits were reduced.28 Three studies reported the mean time taken to complete medication reconciliation by pharmacist. This varied from 1 hour 27 min to 3 hours 51 min per patient.
Discussion
The literature was systematically reviewed to evaluate the effectiveness of pharmacist-led medication reconciliation performed in the community after hospital discharge. Pharmacists were more effective at identifying and resolving discrepancies compared with the usual care process. Meta-analysis did not demonstrate a statically significant reduction in readmission rates, and the effect on emergency department attendance and workload of other healthcare team members was rarely measured and no consistent evidence of related benefit was found.
Comparison with previous literature
Previous systematic reviews also reported the ability of pharmacists to effectively identify and resolve discrepancies in community14 and hospital settings.8 36 37 The clinical relevance of reduced discrepancy resolution has been questioned in studies set in the community as many discrepancies remained after interventions14 and the effect on patient outcomes was not consistent.15 Several of our included studies derived their taxonomies of discrepancies empirically, which did not aid evaluation of clinical relevance.25–28 31 32 34 The lowest mean time to complete medication reconciliation reported in our included studies was 1 hour 27 min.22 The time taken in usual care processes was never accurately reported. Having more time to perform this task may be the reason why more discrepancies are identified.
Unlike our study, a recent systematic review and meta-analysis of pharmacist-led medication reconciliation in hospital performed at care transitions demonstrated a reduction in healthcare use after discharge.7 One possible explanation is that Mekonnen et al included studies with multiple intervention components, including patient education, follow-up telephone call, home visit, medication review, enhanced communication with primary care and the use of strategies to enhance adherence. Interventions in our systematic review included some of these components but excluded those describing a medication review and, as medication reconciliation was performed in the community, infrequently involved interventions to improve primary/secondary care communication. This may reflect the problem of varying definitions of medication reconciliation. The WHO defines medication reconciliation as ‘The formal process in which healthcare professionals partner with patients to ensure accurate and complete medication information transfer at interfaces of care’.1 Such a definition may legitimately include all the aspects of interventions included by Mekonnen et al. The Joint Commission definition of ‘The process of comparing a patient’s medication orders to all of the medications that the patient has been taking’ is more precise and may not include such diverse activities.3 It may be that these additional components are important to influence health outcomes; however, recent systematic reviews of pharmacist-completed medication reviews in various settings have failed to show a benefit to patient outcomes.38 39
It is reported that roughly half of all discharge communications have been found to contain unintended medications.40 Performing an accurate medication reconciliation using such a list is unlikely to improve patient outcomes as unintended medications will continue to be prescribed.17 However, even when medication is reconciled before discharge and patients followed up by pharmacists to improve adherence, clinically important medication errors and harm due to medication are not reduced.40
Implication for future policy and research
The lack of effect on patient outcomes raises the question of what role the pharmacists should play postdischarge. Patients are at a high risk of harm due to medication following discharge, and the involvement of pharmacists seems a logical step to reduce the risk of harm.41 Despite this, there is a paucity of high-quality studies investigating pharmacist-led medication reconciliation postdischarge, and the few that do exist do not provide conclusive evidence of benefit. At present, pharmacist-completed medication reconciliation postdischarge cannot be promoted to reduce harm and improve health outcome. Future research must do more than evaluate process measures such as discrepancy rate detection, and focus on evaluating the clinical relevance of resolved discrepancies such as potential or actual adverse drug events. This may be more resource-intensive as clinical review of notes is required to make judgements on clinical relevance.24 29 40 In addition, the development of an agreed taxonomy of discrepancies would be beneficial to aid process evaluation of such interventions and understanding of discrepancy relevance and why they occur.9
The lack of improvement in patient outcomes may be less important to policymakers and front-line clinical teams if reduction in workload pressures improves performance in other areas of primary care such as face-to-face clinical care or administrative tasks such as laboratory test results handling. High levels of workload are perceived as a major safety concern in UK general practice, and one of the main policy drivers of pharmacist role development is to free clinical and administrative time for GPs.42 The effect of pharmacist-led medication reconciliation on these related systems has not been studied previously and further research is clearly needed.
If the pharmacist’s role in medication reconciliation postdischarge is to free clinical time, then implementation at scale will require significant financial and personnel resources.43 Future research should determine if these predicted efficiency savings exist and if other healthcare team members, such as pharmacy technicians or existing primary care staff, can perform medication reconciliation equally safely and improve cost-effectiveness.44 This research may identify if certain high-risk groups are more likely to derive benefit from pharmacy input postdischarge and what type of intervention has the most impact on medication safety (eg, reconciliation, review, adherence aids, health literacy aids).
Strengths and limitations
The search strategy included several relevant databases, with no limitation placed on date of publication or language. Broader terms than medication reconciliation were included in the search to incorporate studies reporting medication reconciliation as part of wider interventions. For example, although Holland et al describe their intervention as a medication review, we deemed it to be similar enough to our classification of medication reconciliation to be included. Screening for inclusion, data abstraction and quality appraisal were independently completed by two reviewers to enhance study rigour.
The study has several limitations. Some studies that would have been valuable in answering our questions may have been excluded as their focus of intervention was not on medication reconciliation per se.45 One study evaluated a community liaison pharmacist intervention but was based in hospital and so was excluded.46 Healthcare settings vary and findings from different countries may not be comparable. For example, studies were set in North American primary care services run by large organisations often with links to hospitals that may blur the lines between primary and secondary care.23 33 Others involved home care services that may not be present in other areas.28
The CASP tools used to assess bias and quality are designed for use in RCTs and cohort studies and were adapted to assess the quality of QI projects and pre–post intervention studies. This led to these studies being treated as having a higher risk of bias. Several of the included studies were described as pilot projects25 32 or QI projects,27 33 34 and require more robust evaluation of their findings to determine if they are replicated at scale or in different settings. Included studies were generally of low to moderate quality and susceptible to bias, which means the positive outcomes reported in this systematic review must be treated with caution.
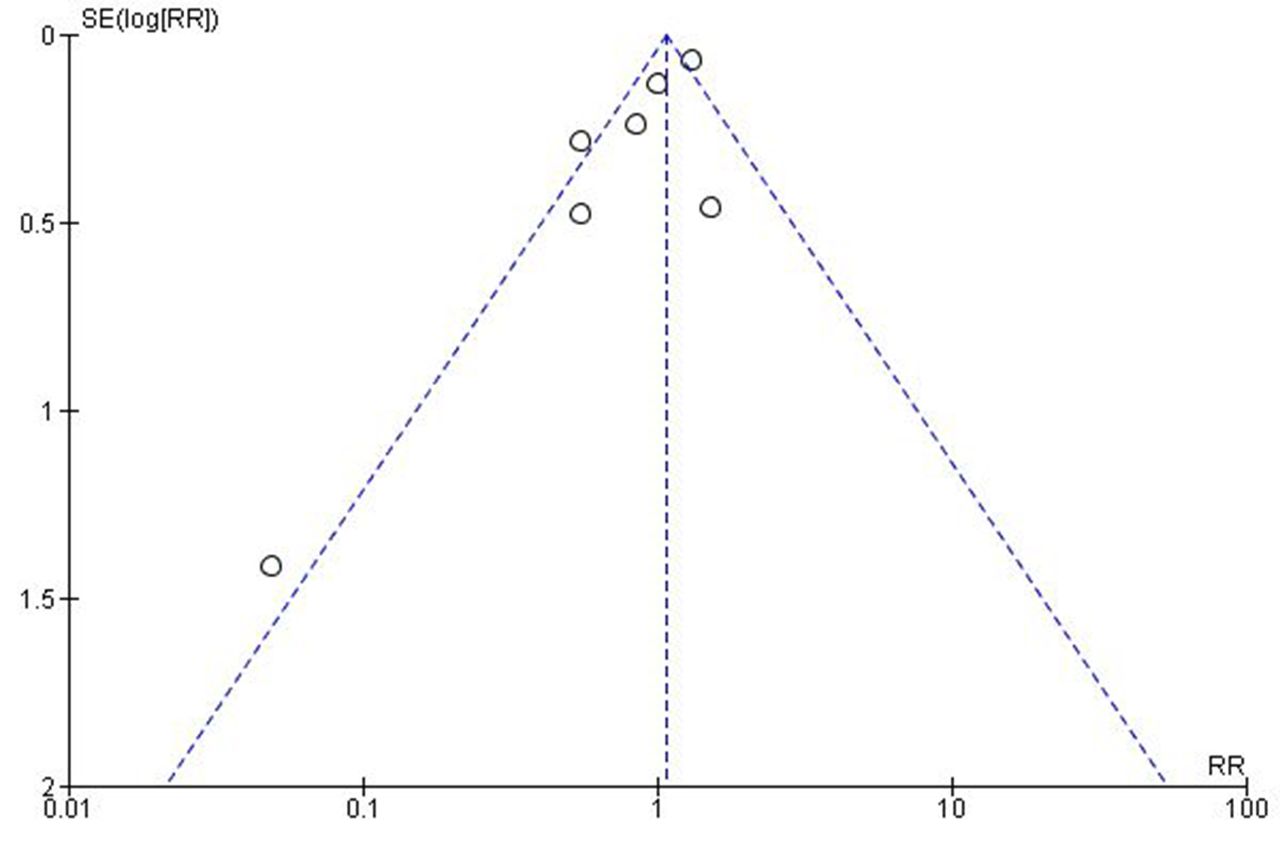
The meta-analysis of data from studies reporting readmission rates was limited to studies that reported similar outcomes; however, this approach may still be open to challenge. A high level of heterogeneity was identified with possible reasons including different study designs, settings, intervention components, outcome definitions and follow-up periods. This means that it is difficult to draw definitive conclusions from the meta-analysis other than to say that there is currently no firm evidence that readmission rate is reduced. Meta-analysis of other outcome measures was not possible due to heterogeneity of reported outcomes. For example, discrepancy identification rates were reported as the number of discrepancies per drug prescribed24; the number of patients in a study who had a discrepancy25; full or partial implementation of the patient plan32; and the number of discrepancies resolved.28 Despite the inclusion of a wide range of study type, publication bias may still influence results as demonstrated by the asymmetry of the funnel plot (figure 3). Of note, the smallest study showed the largest positive effect.25 It may be that smaller projects with less robust methods that did not show a positive effect were not published.
{kind=link}
{kind=link}
{kind=link}
Funnel plot of SE of risk ratio (RR) versus risk ratio.
Conclusions
This systematic review has shown that pharmacists can identify and resolve discrepancies while completing medication reconciliation after hospital discharge; however, the clinical relevance of these discrepancies has rarely been reported. The evidence does not support a reduction in readmission rates and there is not consistent evidence that other measures of healthcare utilisation, such as emergency department attendance and GP appointments, are reduced. Future research in this area should compare the clinical relevance of discrepancies identified and measure if this process reduces workload and thus frees clinical time in primary care.
Acknowledgments
The authors would like to thank Dr Lynda Cochrane for her guidance on the statistics used in this paper and Allan Gillies, NHS Education for Scotland, for assistance in designing the search strategy.
References
Footnotes
Contributors DM and MR performed title, abstract and full-text screening. All authors discussed disagreements to reach consensus. DM extracted data from all included studies. A second data extraction was completed independently for each included study. This was divided evenly between PB, AR, GM and JM. All authors reviewed and contributed to writing the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Search syntax for all databases and all versions of citation lists are available from DM.