Article Text

Abstract
Background Identifying characteristics associated with struggling healthcare organisations may help inform improvement. Thus, we systematically reviewed the literature to: (1) Identify organisational factors associated with struggling healthcare organisations and (2) Summarise these factors into actionable domains.
Methods Systematic review of qualitative studies that evaluated organisational characteristics of healthcare organisations that were struggling as defined by below-average patient outcomes (eg, mortality) or quality of care metrics (eg, Patient Safety Indicators). Searches were conducted in MEDLINE (via Ovid), EMBASE, Cochrane Library, CINAHL, and Web of Science from database inception through February 8 2018. Qualitative data were analysed using framework-based synthesis and summarised into key domains. Study quality was evaluated using the Critical Appraisal Skills Program tool.
Results Thirty studies (33 articles) from multiple countries and settings (eg, acute care, outpatient) with a diverse range of interviewees (eg, nurses, leadership, staff) were included in the final analysis. Five domains characterised struggling healthcare organisations: poor organisational culture (limited ownership, not collaborative, hierarchical, with disconnected leadership), inadequate infrastructure (limited quality improvement, staffing, information technology or resources), lack of a cohesive mission (mission conflicts with other missions, is externally motivated, poorly defined or promotes mediocrity), system shocks (ie, events such as leadership turnover, new electronic health record system or organisational scandals that detract from daily operations), and dysfunctional external relations with other hospitals, stakeholders, or governing bodies.
Conclusions Struggling healthcare organisations share characteristics that may affect their ability to provide optimal care. Understanding and identifying these characteristics may provide a first step to helping low performers address organisational challenges to improvement.
Systematic review registration PROSPERO: CRD42017067367.
- quality improvement
- healthcare quality improvement
- patient safety
- qualitative research
- leadership
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The Institute of Medicine’s 2001 report addressing variation in quality of care1 spurred strong interest by healthcare organisations and patients to improve quality.2 Today, US healthcare quality is publicly reported and linked to reimbursement, providing an impetus for improvement. Some healthcare organisations, however, still have difficulty crossing the quality chasm.3 The potential causes of failing to attain quality targets are myriad. For example, resource availability, location and patient case-mix can affect performance.4–8 Yet, these factors only partially explain variation in quality.7
Studies of top-performing organisations suggest they share common features, including a positive ‘organisational culture’ (ie, the norms, values and basic assumptions of an organisation) that embraces change.9–11 This flexibility may accelerate adoption of patient safety initiatives that improve care.12–16 In addition, high performing organisations often have robust patient safety programmes,15 16 led by committed individuals who support and respect employees.16 While much is known about success in high-performing organisations, little is known about why low performing organisations struggle. Addressing this gap can help organisations most in need identify and overcome barriers.
We thus conducted a systematic review of qualitative studies that evaluated healthcare organisations with below-average performance in patient outcomes or quality of care metrics. Taking advantage of detailed, discovery-oriented data contained in qualitative studies,17 we performed framework-based thematic synthesis18 19 to: (1) Identify organisational factors associated with struggling healthcare organisations and (2) Summarise these factors into actionable domains that may inform efforts to improve quality.
Methods
A research team composed of experts in implementation science, qualitative research methods, patient safety and systematic reviews was convened to determine project design and data throughout the study. We developed and registered a study protocol (PROSPERO: CRD42017067367, available at: http://www.crd.york.ac.uk/prospero/display_record.asp?src=trip&ID=CRD42017067367) following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses recommendations.20
We focused on qualitative studies—those that use open-ended techniques, such as interviews and non-statistical techniques for analysis17—for three reasons. First, qualitative data are useful to evaluate some concepts (such as culture) that can be difficult to measure quantitatively.21 Second, qualitative studies allow concepts to be evaluated in context (eg, how do the beliefs and experiences of front-line staff affect implementation?) adding depth to understanding. Finally, rather than having a priori hypotheses, inclusion of qualitative studies allows for inductive generation of themes (summary concepts based on data) to identify novel aspects related to performance.17
We sought to specifically identify characteristics and barriers that may impede improvement efforts and/or result in poor patient outcomes at struggling healthcare organisations. Therefore, in contrast to studies of ‘positive deviants', we studied such ‘negative deviants’ to identify unique barriers that may not be present in average or high-performing organisations, thus informing efforts directly applicable to such organisations.22
Inclusion criteria
Qualitative studies were eligible for inclusion if they evaluated organisational or cultural characteristics in the context of struggling healthcare organisations. ‘Healthcare organisations’ included ambulatory, subacute, acute, emergency or intensive care settings in any private or public institution. We identified a facility as ‘struggling’ when below-average performance in patient outcomes (eg, mortality) or quality of care (eg, Patient Safety Indicators (PSI-90) Score) was reported. Studies that reported compliance with an intervention or financial performance without associated patient outcomes or quality of care were excluded. Three authors (VV, JA, SW) independently determined eligibility with disagreements resolved through consensus.
Search strategy
Between November 2016 and February 2018, a medical librarian (WT) performed serial literature searches from database inception through February 8 2018 in the following databases: MEDLINE (via Ovid), EMBASE, Cochrane Library, CINAHL and Web of Science. Searches designed for each database included controlled vocabulary terms (Medical Subject Headings) when available, combined with keywords to represent concepts such as ‘low performer,’ ‘laggard’ (online supplementary appendix). Additional studies of interest were found through hand searches of bibliographies and discussion with content experts.
Supplemental material
Data extraction
Data were extracted from included studies independently and in duplicate by 3 authors (VV, JA, SW) on a template adapted from the Cochrane Collaboration.23 Data included definitions for performance, number and role of interviewees, method for sampling (eg, snowball), data collection (eg, interviews) and analysis, and main findings.
We specifically abstracted the following data for analysis: (1) Primary quotes from interviewees (eg, '‘I would like to see more collaboration…’-Director of Performance'),24 (2) Summary quotes (eg, ‘Participants also indicated an inadequate emphasis on learning',24 and (3) Author interpretations of study data (eg, ‘The lack of congruence between … mission[s] created tension'.25 Author interpretations were collected primarily from the results section of manuscripts, however (consistent with other reviews),16 26 interpretations from the discussion were abstracted when supported by data.26 When studies also included high performers, we abstracted data contrasting these 2 categories.
Creation of domains
Abstracted data were analysed using framework-based synthesis—a robust method of pragmatically combining themes from qualitative studies.18 19 This methodology involved a two-step process.18 19 27 First, a framework relevant to the study question was identified a priori. Given its comprehensiveness, widespread applicability and focus on systematically assessing organisational context, we chose the Consolidated Framework for Implementation Research (CFIR).9 CFIR spans 39 constructs consolidated from implementation frameworks to systematically assess contextual factors that influence practice and change efforts. Using CFIR constructs, we created a codebook for identifying organisational characteristics including CFIR domains such as ‘Outer Setting’ and ‘Process'.9 Given that many CFIR constructs are positive or focus on project implementation, not all domains were applicable (eg, ‘innovation characteristics’) and we modified some domains to the negative (eg, ‘leadership engagement’ to ‘disconnected leadership’; online supplementary table 1). Each manuscript underwent line by line coding independently and in duplicate by 3 authors. We paid particular attention to data that contradicted potential underlying assumptions (eg, struggling institutions with exemplary leadership) and report the frequency of supportive versus contradictory references for domains.28 All coding was performed using QSR International’s NVivo V.11.
The second step of framework-based thematic synthesis involved iteratively updating, modifying, refining and creating codes and definitions to describe emerging concepts. We met weekly to compare independently coded manuscripts for consistency to determine whether codes should be revised, removed or added. This approach encouraged generation of new ideas, while incorporating robust theory from prior research.26 27 29 For example, the code ‘hierarchical culture’ (defined by CFIR as ‘clear lines of authority over organisational processes’)9 remained consistent. Conversely, when ideas emerged that were not related to CFIR constructs, we created novel codes. For example, ‘major scandals’—a negative public relations event that detracted from daily operations—emerged inductively.
After aggregating codes into themes,305 overarching domains that distinguish struggling healthcare organisations were identified. Some codes (eg, mergers) remained as stand-alone themes. Finally, we examined whether representation of domains varied by definition of ‘struggling.’ For this purpose, definitions included: (1) Overall performance metrics (any global hospital rating, eg, star rating), (2) Composite metrics (combined outcomes from at least two diseases, such as PSI-90), or (3) Disease-specific metrics (included either a single disease or outcome, such as central line-association bloodstream infection (CLABSI) rates).
Quality assessment
Study risk of bias was assessed using the Critical Appraisal Skills Program (CASP) checklist,31 which is recommended by the Cochrane Collaboration for qualitative literature.32 The CASP tool consists of 10 questions: 9 addressing quality and 1 addressing ‘value’ (contribution to existing literature). For studies with multiple publications, risk of bias was assessed for the earliest. Three reviewers (VV, JA, SW) assessed each study independently and in duplicate with disagreements resolved through consensus. In accordance with other qualitative reviews, studies were not excluded or stratified by risk of bias.16 26 33 Rather, we assessed relative contribution of low-quality and high-quality studies in defining our domains.27
Results
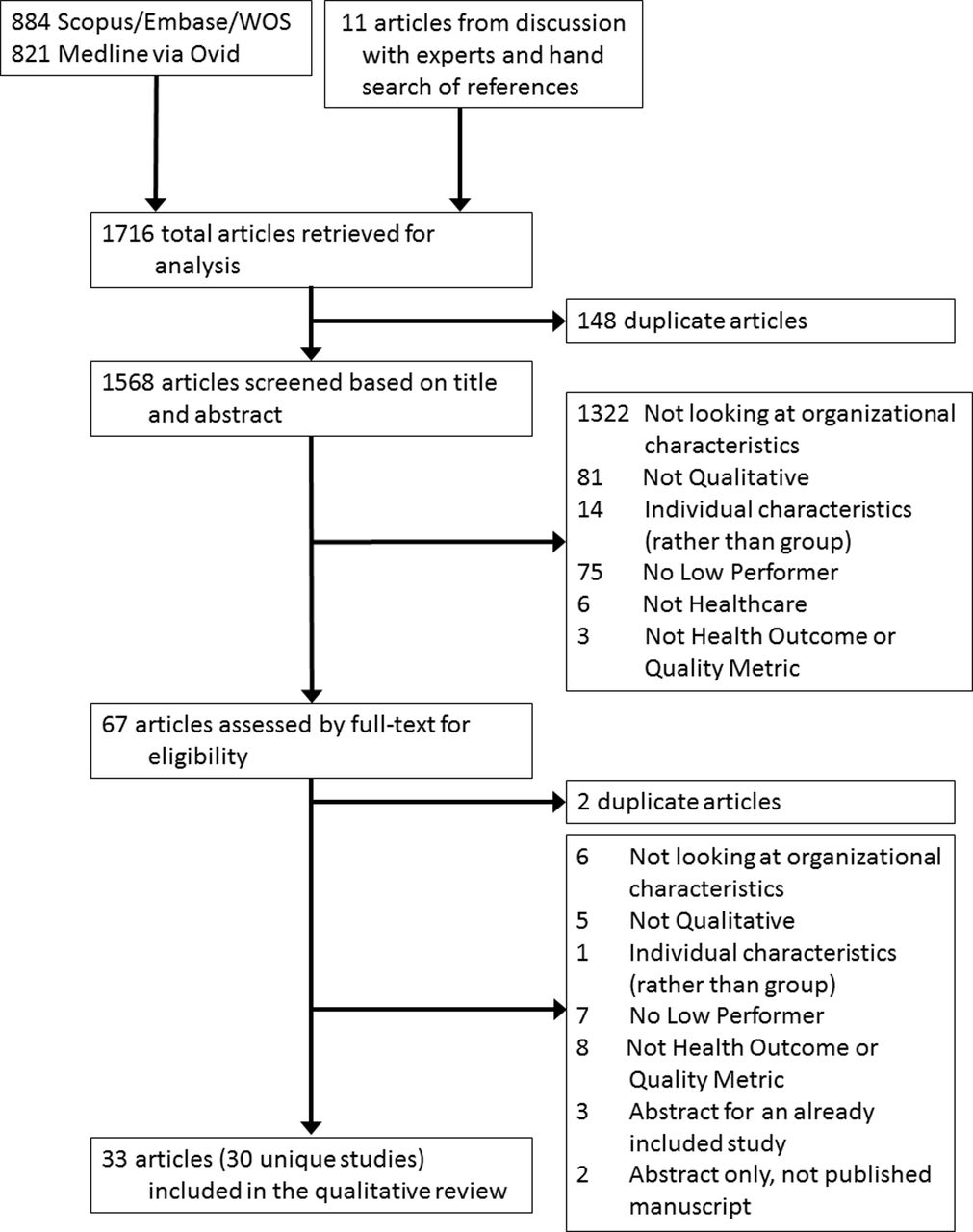
The search yielded 30 unique qualitative studies (33 articles) from various countries (figure 1).24 25 34–64 Studies included adult (12 studies)24 34 35 40 41 45 47 48 53 54 57 64 or paediatric (1 study)63 acute-care hospitals, emergency rooms (1 study),39 nursing homes (3 studies),25 52 60 outpatient primary (7 studies)38 43 44 49 58 61 62 or specialty clinics (1 study),51 primary health systems (1 study),37 accountable care organisations (1 study),36 hospital units (2 studies),55 56 or residential treatment programmes (1 study),59and a diverse range of study participants, including healthcare employees in administrative, clinical and leadership roles. Study sample sizes ranged from 17 to 194 and all but 1 study50 had a high-performing comparator group. Two studies had a mid-performing comparison group.44 63 Criteria for defining performance varied: 4 studies used overall performance metrics,36 46 50 61 12 used composite metrics25 35 37 41 43 52 53 55 57 and 14 used disease-specific metrics (online supplementary table 2).4 24 34 38–40 44 48 49 51 56 58 59 63

Flow diagram of study selection. WOS, Web of Science.
Domains characterising struggling healthcare organisations
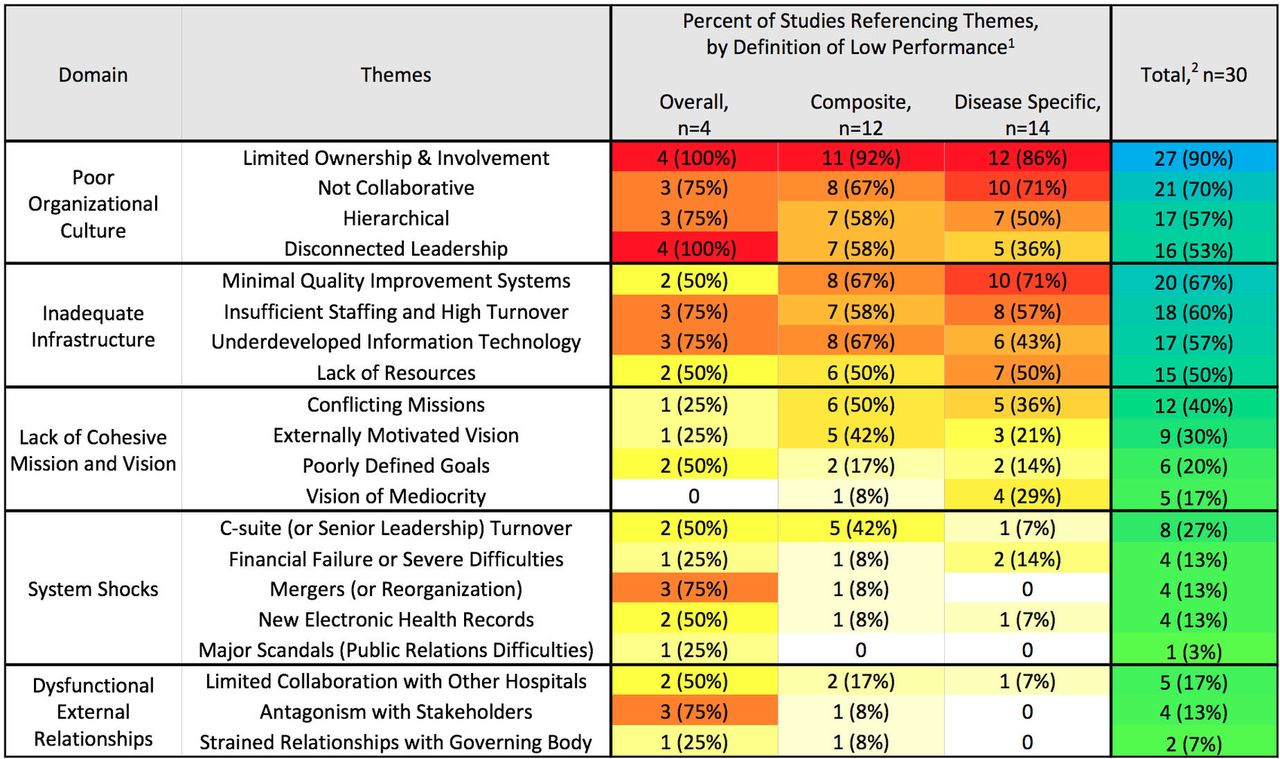
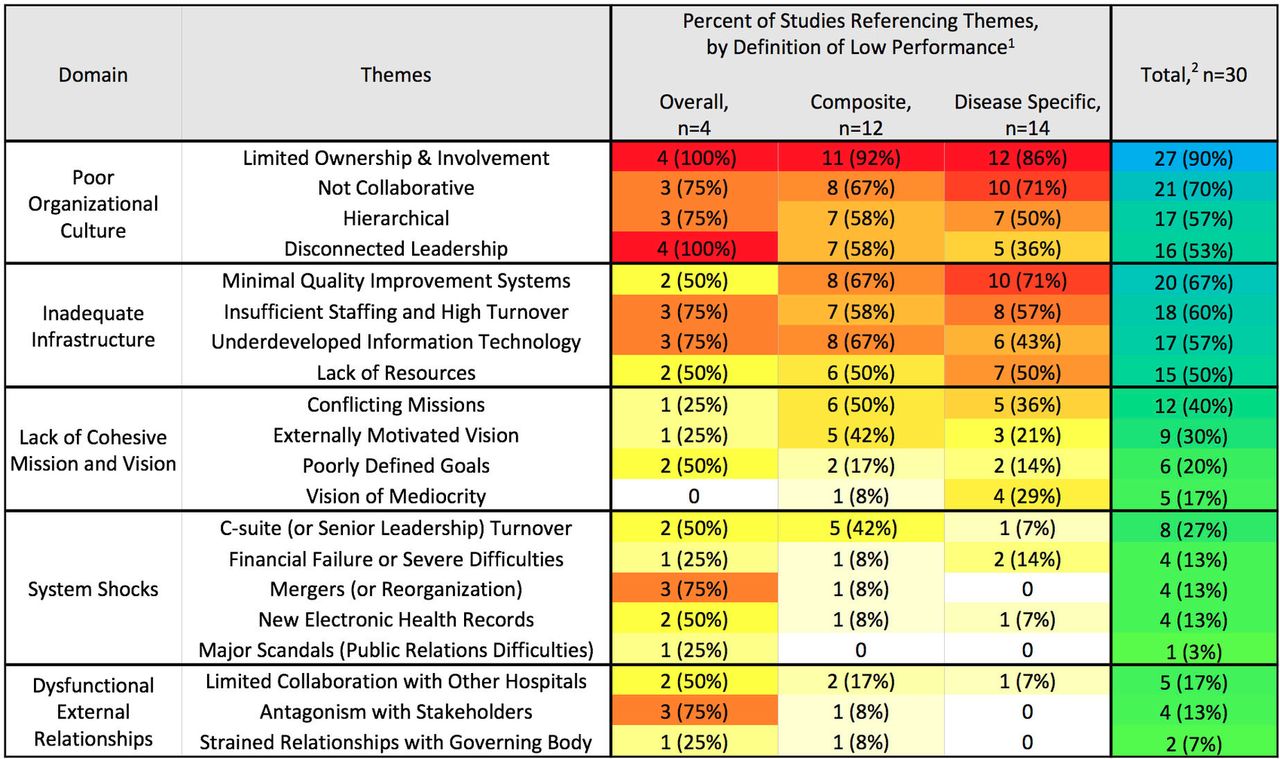
Five domains (figure 2) consistently characterised struggling healthcare organisations, including: (1) Poor organisational culture, (2) Inadequate infrastructure, (3) Lack of a cohesive mission and vision, (4) System shocks and (5) Dysfunctional external relations. Domain definitions, themes, frequency of reporting, contrary findings and representative quotes are reported in table 1.
{kind=link}
{kind=link}
Heat map by percentage of studies referencing each theme. The percentage of studies that included codes for each theme are shown. Studies are separated by method of defining low performance into: (a) overall metrics (eg, star ratings), (b) composite metrics (eg, readmission rates for multiple diseases), or (c) disease-specific metrics (eg, 30-day mortality for acute myocardial infarction)). 1Colour scale for studies by method of defining performance: white=no studies, yellow=least studies to red=most studies.2Colour scale for all studies combined: green-least studies to blue-most studies.
Domains characterising struggling healthcare organisations
Poor organisational culture
All 30 studies described poor organisational culture within struggling healthcare organisations (figure 2) that could be further classified into themes. The most frequent theme, limited involvement and ownership, was found in 27 studies.24 25 34–38 40–44 46 48–52 55–63 This included lack of established responsibility or consequences (16 studies)24 25 34 36–38 41 46 48–50 52 55–57 61 and front-line employees who lacked a sense of ownership (4 studies)50 58 60 61 or self-efficacy (3 studies)24 34 48 60 with many interviewees blaming patient factors for failure (9 studies).34 36 40 48 50 58–60 62 The second theme, a non-collaborative environment (21 studies),4 24 25 35 36 38–40 42 44 48 50–53 55–57 61–63 manifested with employees who: did not feel connected to each other or their institution (8 studies),4 25 38 42 48 52 61 62 operated in silos (7 studies),24 25 35 36 44 48 55 or suffered from low morale (6 studies).25 50–52 61 62 The third theme (17 studies)4 24 25 35–38 44 46 48 50 52 53 55 56 58 60 was hierarchical orientation (‘clear lines of authority of organisational processes').9 Hierarchy was often used to explain why middle managers and champions lacked empowerment (3 studies)46 50 60 and nurses and staff felt undervalued (10 studies).4 24 25 36 38 44 48 50 52 53 55 56 58 Interviewees noted that physician autonomy appeared to trump patient safety (3 studies)36 55 60 and approaches to problems were punitive (7 studies).4 24 25 35 50 55 60 This type of negative hierarchy reportedly resulted in anxiety and fear (5 studies).4 25 37 48 50 The final theme involved disconnected leaders (16 studies)24 25 36–38 40 41 46 48 50 52 53 56 57 61 62 who were blamed for the organisation’s poor culture, thus interviewees linked poor leadership to poor culture. Leaders were described as unsupportive (7 studies),37 48 52 53 57 61 62 underdeveloped (3 studies)34 41 57 or non-transparent (6 studies).36 37 46 50 52 61
Inadequate infrastructure
All but 3 studies52 58 61 reported inadequate infrastructure in struggling healthcare organisations. Examples included inadequate QI infrastructure and processes (20 studies),4 24 25 34 36–42 44 48–50 53 55–57 62 insufficient staffing or high turnover (18 studies), 4 24 25 35 36 38 39 41 42 44 46 49–51 55 59 60 62 poor information technology services (17 studies)24 35–38 41–43 46 48–51 55 57 62 63 and general lack of resources (15 studies).24 36 37 43 44 48–51 53 59 60 62 63 65 Despite the emphasis placed on infrastructure in struggling sites, 18 studies4 24 34 35 37 39–42 48 51 53 57 58 60–63 also reported inadequate infrastructure in high-performing organisations (eg, ‘all sites lacked guidelines …and [had limited staffing] at night';39 ‘all sites… had inadequate computer facilities')42 or that infrastructure alone appeared insufficient to create high performance: ‘The electronic record (EHR) was viewed as a useful tool…but efforts to rely on electronic documentation did not necessarily guarantee improvement'.40
Lack of cohesive mission and vision
Twenty-one of the 30 studies noted that struggling healthcare organisations lacked a cohesive mission or vision.24 25 35 36 38 40–43 48–50 52 53 55 56 58 60–63 Instead, struggling organisations perceived their mission as: (1) conflicting with other stated missions (12 studies),25 38 40 42 48 50 53 55 58 60 62 63 (2) externally motivated (eg, by finances/penalties, 9 studies),24 25 35 40 41 48 50 52 53 (3) poorly defined (6 studies)25 36 38 48 61 62 or (4) reflecting a ‘vision of mediocrity’ (ie, set low expectations; 5 studies).24 43 48 49 56 Trouble identifying with the organisation’s mission demotivated staff, as noted in 1 study: ‘financial gain did not (supply purpose), the implication for…leaders…is that the perception of economic viability as an end-all may be counterproductive'.25
System shocks
System shocks—or an organisation-wide event that detracts from day-to-day operations—represented an inductively derived domain from 12 studies.24 25 36 38 41 42 46 48 50 53 60 62 Such shocks often occurred as the result of planned institutional change, such as when organisations implemented a new electronic health record (4 studies)36 38 50 62 or underwent restructuring (4 studies).36 46 50 62 However, shocks were also due to unplanned events, such as unanticipated leadership turnover (8 studies),24 25 41 46 50 53 60 62 imminent financial failure (4 studies)38 42 48 50 or scandals (1 study).50 When these events occurred, they overwhelmed the organisation’s energy and resources and became the dominating concern (eg, ‘We found that widespread concerns about finances…eclipsed attention paid to patient safety').64 Shocks often negatively affected other domains (eg, ‘An explosive level of turnover made connectivity almost impossible';25 ‘Sporadic involvement of senior management was common…in part because of frequent turnover').24
Notably, some system shocks were transient, or a consequence of attempts to improve, as noted in accountable care organisations trying to improve cost and quality: ‘changes aimed at improving established organisations often caused an initial decrement in their performance as a result of the substantial reorganisations'.36 Regardless of the cause, the effects of system shocks were reported to linger: ‘(Struggling) organisations (had) fragmented systems of accountability…a legacy of recent mergers'.46
Dysfunctional external relations
Seven studies24 35–37 46 50 61 highlighted how dysfunctional external relationships with other healthcare facilities (5 studies),24 35–37 61 stakeholders (4 studies)37 46 50 61 or governing bodies (2 studies)37 50 were associated with dire consequences. Notably, community and patient engagement by low-performing facilities was also limited (3 studies).37 46 61 Failure in this domain was prominent in facilities where financial performance was dependent on external collaboration: ‘In one (accountable care organization)…local hospitals viewed the group as a threat and refused to cooperate in providing patient information'.36
Domain prevalence by how performance was defined
Although many domains were applicable to all struggling healthcare organisations, some differences were observed based on how performance was defined. For example, organisations struggling on a single disease (eg, CLABSI) noted difficulties with infrastructure—particularly QI infrastructure (10/14 studies)—more than external relations (1/14 studies). Healthcare organisations struggling on composite metrics—such as postoperative complications—were more concerned about their mission (10/12 studies) than other organisations (11/18 studies). For organisations struggling on overall performance (eg, star ratings), system shocks and dysfunctional external relationships were defining domains (3/4 and 4/4 studies, respectively; figure 2).
Quality assessment
Study quality was moderate–high with 6 studies scoring 9/1025 40 48 51 53 57 (online supplementary tables 2 and 3). Most studies were rated as ‘valuable’ (19 studies).24 25 35 38 41 46 49–51 53 55–63 Only 6 studies considered the relationship between researchers and participants (CASP question 6).4 25 40 42 61 63 Studies with higher quality (score ≥9) contributed more data (average 3 domains, 8 themes, 42 references) than lower-quality (score ≤6) studies (average 3 domains, 7 themes, 21 references).
Discussion
In this systematic review of 30 international studies, we found 5 distinct domains typified struggling healthcare organisations: (1) Poor organisational culture, (2) Inadequate infrastructure, (3) Lack of a cohesive mission and vision, (4) System shocks and (5) Dysfunctional external relations. Organisations often struggled in multiple domains simultaneously and nearly half of studies reported a recent system shock which appeared to worsen difficulties in other domains. While most domains had a clear, negative effect on organisations, infrastructure was not always linked to outcomes. Taken together, these domains represent a starting place to evaluate and diagnose low performance.
Many characteristics shared by struggling organisations were counter to characteristics associated with high-performing organisations. For example, while disconnected leaders and non-collaborative environments were frequently found in struggling organisations, engaged leadership and a collaborative organisational culture are associated with high performance.12–16 Furthermore, a ‘flat’ or team-based approach to problems is often associated with high performance,12–16 whereas we found hierarchical culture described in 17 studies of struggling organisations. Employees at struggling organisations also described poor self-efficacy and often perseverated on patient factors (eg, ‘difficult patients’) as barriers that could not be overcome, rather than being motivated—as high performers often are—to facilitate communication or provide additional resources to patients most in need. This view of patients as barriers was linked to a general sense that leadership at struggling organisations was motivated by penalties and finances, rather than by a patient-centred mission, which is associated with improved patient experience, physician satisfaction and quality of care.66–68 Finally, struggling hospitals had antagonistic external relationships and poor IT infrastructure, whereas positive external, community and patient relationships, and well-integrated IT systems are associated with improved healthcare organisation performance.15 16 46 69
Not all themes readily contrasted with high performers. While most struggling hospitals reported poor infrastructure, this complaint was not unique to struggling organisations. Rather, employees believed they could benefit from additional staff and resources, regardless of performance or resource availability. Although it was not possible to assess differences in resource availability in low-performing versus high-performing organisations, 3 studies noted that there were no significant differences in performance based on resources.34 60 61 Additionally, improving infrastructure in struggling hospitals did not appear to guarantee improved performance. One explanation offered was that efforts to improve infrastructure frequently diverted resources and disrupted existing care pathways, thus causing a decrement in performance (or leading to a system shock) for the short term.
‘System shocks’ was a domain unique to struggling organisations. Although not all change necessarily causes disruption, being unprepared or unrealistic about the effort required can demotivate and anger staff.70 It is also possible that struggling organisations had underlying problems with disconnected leadership or poor organisational culture that led staff to be less tolerant and responsive to change.11–16 These underlying factors may be further exacerbated when system shocks occur, overwhelming struggling organisations and causing difficulties in other domains. As noted previously, many system shocks were caused by efforts to improve care in the long term and thus may not be completely avoidable. To prevent disastrous consequences, shocks must be anticipated and addressed. When shocks cannot be anticipated, leaders may directly address shocks to reduce negative consequences and potentially create positive change. Examples of using disruptive events as the impetus for culture change abound in business, with examples such as Delta Airlines, Ecolab and Novartis, who all used financial difficulties or scandals to improve their companies.71 Parallel possibilities in healthcare can be found in the dramatic organisational changes that may follow sentinel events.72 73
How may these domains inform efforts to improve quality of care? One approach may be to diagnose which domain(s) is the problem. This may be difficult for organisations, as measurement requires understanding employee perceptions and not all domains have validated measures. Furthermore, many of these domains are interlinked and may be hard to disentangle.74 75 Although multiple tools exist for evaluating organisational or patient-safety culture (eg, Hospital Survey on Patient Safety Culture), use of differing instruments with varying validity make longitudinal assessments and comparisons between hospitals difficult.74 75 Given these difficulties, using the identified domains to facilitate conversation with front-line staff may be the first step.
After diagnosis, comes intervention. Although no easy fix exists for any domain, some studies may guide improvement. For example, a recent study of 10 US hospitals demonstrated that a multimodal intervention that involved creating ‘guiding coalitions’ (multidisciplinary intervention team) improved both organisational culture and outcomes.76 77 Similarly, to reduce CLABSI, empowering nurses to speak up when providers break sterility is important.78 Even within hierarchical cultures, empowerment can be improved by using checklists, ensuring supervisory support, and framing instances of nurses speaking up as patient safety issues rather than power or political ones.78 For struggling organisations, these small changes may be both easier to perform and more sustainable, potentially leading to culture change over time.79 80 To address concerns over organisational motivation, struggling facilities may have more success if they recognise that nurses may view the extra burden of improvement as financially motivated, and reframe in terms of benefit to patients.81 82 Struggling organisations that are poorly networked could begin to improve relations by, for example, joining a quality collaborative—providing access to shared expertise and QI infrastructure and promoting positive culture change.65 83–85 Finally, to capitalise on the opportunity provided by a system shock, hospital leadership may prepare for change by centering on a salient mission to galvanise employees. For example, during and after mergers, leadership must unify to prevent an ‘us vs them’ mentality that can destroy collaboration and morale.86 During financial difficulties, leadership must be transparent regarding budgeting decisions. For example, one hospital turned around their financial crisis through transparency, using town halls to discuss financial problems and brainstorm solutions. In response, senior physicians united and donated money to prevent staff lay-offs.87
Our study has strengths. It is among the first to summarise and codify organisation features that characterise struggling healthcare organisations. Use of framework-based thematic synthesis allowed us to apply a combination of inductive and deductive reasoning to generate novel domains that align with conceptual frameworks and identify ways to improve status quo. In addition, we synthesised our findings into 5 concrete, potentially measurable and modifiable domains, thus enabling organisations to identify barriers to inform future improvement. We followed a rigorous approach including an explicit, published protocol, a comprehensive literature search, and review and qualitative coding by three reviewers. Finally, we unearthed an important domain—system shocks—and identify how it may create critical, system-wide barriers for improvement.
Our study also has limitations. First, qualitative studies by nature have a small sample size with limited number of individuals and scenarios. However, qualitative data provide greater depth and detail to understand underlying issues in context—which was our goal. Second, to avoid making incorrect assumptions, we reported language used by interviewees even if inconsistent with organisational science literature. Third, as with all systematic reviews, we were only able to assess reported results and quotations. Fourth, the quality of included studies varied and methodological stuy details were often lacking, reducing our ability to evaluate quality. Finally, whether these domains cause—or result from—organisational struggle, cannot be determined from this work. Rather than infer causality, we focused on identifying characteristics of struggling organisations that may reflect barriers to improvement.
Our study has important implications. First, our findings suggest that health systems preparing for large-scale organisational change should adequately prepare in order to prevent system shocks, which, counterintuitively, may impede change. Second, our study underscores the importance of context, organisational climate and related factors in determining hospital performance. Third, we continue to require validated methods of measuring and improving organisational domains, such as those found in this study. In the interim, leaders should engage front-line staff to help identify and address problem domains.
Healthcare value and quality matter now more than ever. We found struggling healthcare organisations have unique characteristics that may hinder their ability to meet quality challenges. The domains delineated in this review provide a starting point for addressing performance. The next step is to design high-quality interventions that help struggling hospitals improve.
References
Footnotes
Contributors As first author of this study, I take responsibility for the integrity of this work as a whole. We certify that all authors have seen and approved the manuscript. Each author has contributed significantly to it.
Funding This study was supported by Centers for Disease Control and Prevention (Contract Number: 200-2015-88275).
Disclaimer The findings and conclusions in this manuscript are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention or the Department of Veterans Affairs.
Competing interests SS has received fees for serving on advisory boards for Doximity and Jvion. JM has received honoraria for lectures and teaching related to prevention and value-based purchasing policies involving catheter-associated urinary tract infection and hospital-acquired pressure ulcers. She has also received honoraria from RAND Corporation/AHRQ for preparation of an AHRQ Chapter update on prevention of catheter-associated UTI.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Coding data from this qualitative review are available upon request to the corresponding author, VMV, at valmv@umich.edu.