Article Text

Abstract
Background Emergency department (ED) physicians and nurses frequently interact with emotionally evocative patients, which can impact clinical decision-making and behaviour. This study introduces well-established methods from social psychology to investigate ED providers’ reported emotional experiences and engagement in their own recent patient encounters, as well as perceived effects of emotion on patient care.
Methods Ninety-four experienced ED providers (50 physicians and 44 nurses) vividly recalled and wrote about three recent patient encounters (qualitative data): one that elicited anger/frustration/irritation (angry encounter), one that elicited happiness/satisfaction/appreciation (positive encounter), and one with a patient with a mental health condition (mental health encounter). Providers rated their emotions and engagement in each encounter (quantitative data), and reported their perception of whether and how their emotions impacted their clinical decision-making and behaviour (qualitative data).
Results Providers generated 282 encounter descriptions. Emotions reported in angry and mental health encounters were remarkably similar, highly negative, and associated with reports of low provider engagement compared with positive encounters. Providers reported their emotions influenced their clinical decision-making and behaviour most frequently in angry encounters, followed by mental health and then positive encounters. Emotions in angry and mental health encounters were associated with increased perceptions of patient safety risks; emotions in positive encounters were associated with perceptions of higher quality care.
Conclusions Positive and negative emotions can influence clinical decision-making and impact patient safety. Findings underscore the need for (1) education and training initiatives to promote awareness of emotional influences and to consider strategies for managing these influences, and (2) a comprehensive research agenda to facilitate discovery of evidence-based interventions to mitigate emotion-induced patient safety risks. The current work lays the foundation for testing novel interventions.
- emergency department
- attitudes
- diagnostic errors
- mental health
- patient safety
Statistics from Altmetric.com
Introduction
Despite widespread awareness that patients can elicit significant emotions in healthcare providers,1–4 and that providers’ emotions may play an important role in patient safety,1 4–9 the role of emotions remains a rarely explored ‘blind spot’.5 6 10 Yet a substantial body of research in social cognitive and affective science demonstrates that emotions such as anger and happiness reliably and profoundly influence how people think,11–15 including the extent to which individuals process information in a heuristic, abstract, and superficial manner versus a more careful, detailed, and analytical manner (ie, system 1 vs system 216). This can have important implications for clinical decision-making and patient safety.6 7 17
A small body of literature has identified characteristics of ‘difficult patients’ (eg, demanding)18 19 and suggests that they may elicit negative emotions in providers,1–3 20 which may reduce diagnostic accuracy among medical residents.21 22 While two recent vignette studies21 22 found that describing a patient as ‘difficult’ reduced diagnostic accuracy, it is unclear whether this was due to negative emotions. Such descriptions might have activated stereotypes (ie, beliefs) about a patient rather than triggering ‘felt’ emotions. In contrast to beliefs, emotions are psychological states that include subjective experience (ie, feelings) and may also include expressive behaviour and physiological reactions.11 23 24 Given this, interventions to reduce adverse influences of emotions on clinical decision-making and behaviour will necessarily be different than those needed to combat negative beliefs about a patient.6
Using a valid, reliable, and commonly used emotion elicitation method (ie, vivid autobiographical recall) from psychological research,25 26 the current research systematically assessed healthcare providers’ reported emotions in response to their own recent patient encounters. Given that diagnostic errors, patient safety events, and emotions are particularly prevalent in emergency medicine4 27–29 due to unique challenges in the emergency department (ED; eg, unpredictability, stress, overcrowding, interruptions30), we conducted our investigation in this context.
In addition to focusing on patients who trigger anger or frustration, we examined two patient populations that are rarely studied in patient safety research: patients who elicit positive emotions and patients with mental health conditions. This latter population is particularly vulnerable. That is, these patients are considered ‘difficult’,18 19 are subject to considerable stigma in the ED31 and elsewhere,32 33 suffer a broad range of healthcare disparities,34–37 are at increased risk for diagnostic error,38 experience greater morbidity and mortality,39–41 and represent a sizeable and growing proportion of ED patients.42 43
Drawing on the emotion, social cognition, and patient safety literatures, the purpose of this interdisciplinary investigation was to (1) assess the range and types of emotions ED physicians and nurses report in response to their own recent emotionally evocative patient encounters, (2) identify themes and emotional triggers in these encounters, and (3) explore providers’ perceptions of their engagement with these patients and whether and how emotions influenced their clinical reasoning and behaviour.
Methods
Participants
Participants were recruited via invitations sent to ED physicians and nurses in the USA between August and October 2018, using hospital and other ED mailing lists. The invitation indicated that we were studying physicians’ and nurses’ experiences with different types of patients, and no information concerning our interest in emotional experiences was given. Interested providers were instructed to send a note to a university-based email address. Eligible providers were then sent an individualised, one-time-use link to complete the study and were given 2 weeks before the link expired. Near the end of this period, reminders were sent to providers who had not accessed the study, and they were offered a new link and an additional week to complete the study. In accordance with the average hourly rate for ED physicians in the USA at the time,44 physicians were compensated US$200.00 for completing the study. Nurses were compensated US$100.00.
Design
This study was hosted on the Qualtrics platform. Participants were asked to vividly recall and write about three recent patient encounters, including an angry encounter, a positive encounter, and one involving a patient with a mental health condition. Using the randomiser option in Qualtrics, physicians and nurses completed these tasks in one of two orders, with all participants describing the mental health encounter last. This study is a 3 (patient encounter type) × 2 (physician vs nurse) × 2 (patient description order) quasi-experiment, with the first factor within subjects and the second two between subjects. This quasi-experiment took place within the framework of a convergent mixed methods study, which allowed us to use qualitative data to add greater depth to our quantitative results.45 (See online supplementary figure S1 for study design and flow.)
Supplemental material
Materials and procedure
This study consisted of two phases. In phase 1, we adapted a highly reliable and valid emotion elicitation method (vivid autobiographical memory recall) commonly used in the affect literature25 26 46–48 to elicit emotions. For the first two patient encounters, participants were instructed to think about their last few months working in the ED, including some of the patients they saw during that time. They were then asked to choose one patient experience that led them to feel irritated, frustrated or angry (vs happy, appreciated or pleased), and continued to make them feel this way when they thought about it now. Providers were prompted to describe the patients and their experience vividly and in detail by typing in a text box. Instructions for the third encounter were similar, except participants were instructed to describe an experience with a patient with a mental health condition. Complete instructions appear in the online supplementary material.
Following each description, participants completed emotion and engagement measures that assessed the extent to which they felt (1) angry (angry, frustrated, annoyed, irritated; Cronbach’s alpha=0.90), (2) sad (sad, down, discouraged; Cronbach’s alpha=0.71), (3) anxious (anxious, uneasy, nervous, uncertain, at ease, calm, relieved; Cronbach’s alpha=0.80), (4) fatigued (fatigued, exhausted; Cronbach’s alpha=0.86), (5) happy (satisfied, happy, pleased; Cronbach’s alpha=0.85), (6) self-assured (proud, self-assured, confident; Cronbach’s alpha=0.74) and (7) engaged (empathic, engaged, attentive; Cronbach’s alpha=0.70) during the encounter. These scale items were chosen based on findings from (1) an extensive review of emotion scales used in psychological research, and (2) a subsample of ED physicians (n=18) and nurses (n=14) who participated in a separate interview study (with LMI) in which providers described their emotions in the ED.4 Participants responded to each item using continuous unnumbered sliding scales. Based on where participants moved the slider, a value between 1.00 (not at all) and 5.00 (very much) was recorded. Mean scale scores were computed separately for each participant for each encounter.
In phase 2, which immediately followed, participants were presented with each encounter they described in phase 1 in random order. A subset of participants (77%; n=72; 42 physicians and 30 nurses) was asked, ‘Do you think the emotions that you experienced while treating this patient may have influenced your clinical reasoning and decision-making in this case?’ Participants who responded ‘yes’ or ‘uncertain’ were prompted to describe the influence. These questions were added following feedback we received after collecting data from 22 participants (8 physicians and 14 nurses). For each encounter, all participants made several judgements about the patient, and reported patient demographic information and information about the ED during the encounter. These questions, which were included for descriptive and exploratory purposes only, are reported in the online supplementary material along with relevant analyses (see tables S3-S5 and figure S2 in the online supplement). Finally, participants provided personal information (see table 1).
Sample characteristics
Sample size
Based on an a priori power analysis using G*Power (V.3.1),49 we aimed to recruit 84 participants (42 physicians and 42 nurses) to achieve 80% power to detect differences in emotion and engagement profiles for different patient encounters and between physicians and nurses, assuming a medium effect size (f=0.25).
Analysis
Quantitative data
Quantitative data were analysed using SPSS V.23.
To examine whether ED providers’ emotions varied by patient encounter and to explore whether such variation was dependent on participant profession (physician vs nurse) or encounter order, we subjected participants’ scores on the emotion and engagement scales to a three-way mixed multivariate analysis of variance with patient encounter as a within-subjects factor, and participant profession (physician vs nurse) and encounter order as between-subjects factors. As described in the online supplementary material, we also conducted quantitative linguistic text analysis to examine the emotional tone in providers’ written encounter descriptions.50–55
We applied Bonferroni correction to all pairwise comparisons to ensure the family-wise error rate did not go beyond 0.05.56 We used correlations to assess associations between continuous variables, and χ2 tests to examine differences in categorical variables.
Qualitative data
To identify main themes in (1) providers’ patient encounter descriptions and (2) providers’ perceptions of the influence of emotions on their clinical decision-making and behaviour, we employed inductive content analysis. Text responses were coded using Microsoft Excel V.16.23. The coding structure was determined via an iterative process. The original codebooks for each of the two coding tasks were developed by two undergraduate research assistants (RAs) and two research coordinators (JT and KB). All four individuals read all qualitative responses and worked collaboratively to create a codebook for each of the two coding tasks. The RAs individually coded all qualitative data and disagreements were resolved by research coordinators. Following this process, research coordinators read all open-ended descriptions a second time and worked together to refine the codebooks for greater specificity. They then individually coded approximately half of the patient encounter descriptions each and communicated as needed. They also independently coded all of the emotional influence data and discussed disagreements until they reached consensus.
Results
Sample characteristics
Ninety-five providers (50 physicians and 45 nurses) participated, however one nurse was excluded from analysis for not describing any patient encounters, leaving a sample of 94 providers from 29 EDs. This sample includes 75% of the 127 eligible providers (66 physicians and 61 nurses) who responded to our email invitation and requested a study link. Sample characteristics appear in table 1. The gender distribution of participants is consistent with the distribution of nurses57 and ED physicians in the USA,58 and the distribution of race among our physicians is consistent with national data58; however, our nurses were disproportionately Caucasian.57
Emotion and engagement profiles
Ninety-four ED providers produced 282 patient encounter descriptions. Participants’ reports of their emotional experiences and engagement in these encounters varied depending on encounter type, F(14, 332)=40.20, p<0.001, η2 p =0.63, and this effect was independent of participant profession (physician vs nurse), encounter order, and their interaction, F(14, 332)=1.57, p=0.09.
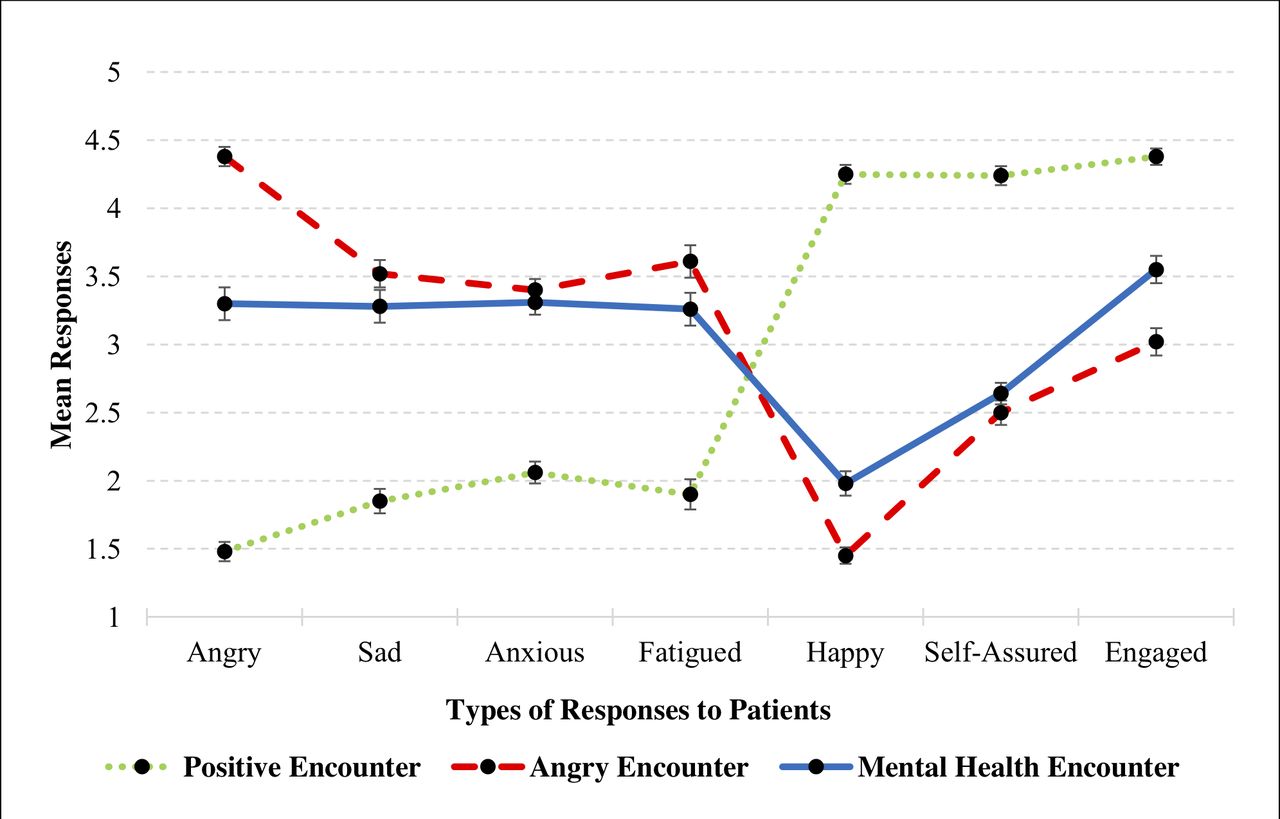
As shown in figure 1, the overall pattern of reactions to angry patients and to those with mental health conditions is similar. Providers reported feeling similarly sad (3.52 vs 3.28; p=0.18), anxious (3.40 vs 3.31; p=0.99) and low in self-assurance (2.50 vs 2.64; p=0.68). Providers also reported high levels of fatigue and anger, and low levels of happiness and engagement in response to both types of patients; however, they reported feeling more fatigue (3.61 vs 3.26; p=0.04; Cohen’s d=0.32), more anger (4.38 vs 3.30; p<0.001; Cohen’s d=1.17), less happiness (1.45 vs 1.98; p<0.001; Cohen’s d=0.72) and less engagement during angry encounters (3.02 vs 3.55; p<0.001; Cohen’s d=0.55).

{kind=link}
Providers’ emotional reactions and engagement during different patient encounters. (Note: Sliding scales range from 1.00 (not at all) to 5.00 (very much). Error bars represent plus/minus one standard error. Lines in the graph are not intended to suggest a linear relationship)
Positive encounters were marked by relatively high levels of self-reported engagement, self-assurance, and happiness, and low levels of negative emotions. To illustrate the magnitude of such differences, we collapsed providers’ reported responses in angry and mental health encounters and compared them to responses in positive encounters. Providers reported feeling significantly more engagement (4.38 vs 3.29; p<0.001; Cohen’s d=1.41), self-assurance (4.24 vs 2.57; p<0.001; Cohen’s d=2.34) and happiness (4.25 vs 1.72; p<0.001; Cohen’s d=3.51), and less anger (1.48 vs 3.84; p<0.001; Cohen’s d=−2.89), sadness (1.85 vs 3.40; p<0.001; Cohen’s d=−1.68), anxiety (2.06 vs 3.36; p<0.001; Cohen’s d=−1.73) and fatigue (1.90 vs 3.44; p<0.001; Cohen’s d=−1.46) during positive encounters compared with angry and mental health encounters. (See the online supplementary material for analyses of emotional tone in providers’ written encounter descriptions using quantitative linguistic text analysis, which converge with findings reported here.)
Relationship between reported provider engagement and emotional experiences
Reported self-assurance was associated with greater perceived engagement in positive (r=0.431; p<0.01), angry (r=0.355; p<0.01), and mental health (r=0.222; p<0.05) encounters. Reported anger was associated with lower perceived engagement in angry (r=−0.290; p<0.01) and mental health encounters (r=−0.367; p<0.01). In positive and angry encounters, reported happiness was associated with greater perceived engagement (r=0.258; p<0.05 and r=0.351; p<0.01). In angry encounters, reported anxiety and fatigue were also associated with lower perceived engagement (r=−0.241; p<0.05 and r=−0.204; p<0.05). (See online supplementary table S1 for correlations among scales.)
Patient encounters: major themes
Table 2 provides a summary of the main themes that emerged in different encounter types and their frequencies (see online supplementary table S2 for redacted examples of encounter descriptions).
Frequency of main themes in provider-generated descriptions of their (A) angry, (B) positive and (C) mental health encounters
The most prominent theme involved healthcare providers’ perceptions of patient behaviours, which differed markedly depending on encounter type. For positive encounters, the majority of encounters included gratitude from patients, whereas in angry encounters, the majority included behaviours that providers perceived to be demanding, entitled, or manipulative (53%; n=50), with a large percentage involving perceived verbal or physical abuse (36%; n=34), frequent/high utilisers (37%; n=35), and unrealistic patient expectations (24%; n=23). In mental health encounters, behaviours that providers perceived to be demanding, entitled, or manipulative similarly emerged in 52% of encounters (n=49), with a sizeable proportion involving perceived verbal or physical abuse (32%; n=30). Despite the general negativity in mental health encounters, a small proportion (23%; n=22) included patient behaviours perceived to be positive. Notably, hospital and system issues emerged as a theme most frequently in mental health (38%; n=36) and angry (26%; n=24) encounters, but not in positive encounters.
Given that somewhat more emotionally mixed themes emerged in mental health encounters, we examined provider emotions in these encounters. As shown in table 2, the most frequent emotion was anger (59%; n=55), followed by sadness, helplessness and empathy (35%; n=33), and fear/anxiety (13%; n=12). Positive emotions emerged in only 9% (n=8) of these encounters.
Emotional influences on clinical reasoning and decision-making
A majority of participants who completed the emotion influence questions (75%; n=54) perceived that their emotions influenced their clinical decision-making in at least one encounter, with this increasing to 82% (n=59) when including those who indicated uncertainty in at least one case. Participants were most likely to endorse (or indicate uncertainty) that emotions influenced them in angry encounters (63%; n=45), followed by mental health (47%; n=34), and positive encounters (39%; n=28) (p=0.02; χ2 test). No differences emerged between physicians and nurses, all p>0.33.
Themes that emerged from qualitative analysis of providers’ reports of how their emotions influenced them, along with representative quotes from providers, appear in tables 3–5. These data demonstrate that emotions experienced in angry encounters were associated with reports of detrimental behaviours that likely reduced quality of care (table 3). In contrast, emotions experienced in positive encounters led providers to report behaviours that likely resulted in better care and possibly less error (table 4). Emotions experienced in mental health encounters resulted in providers reporting behaviours that likely had both detrimental and beneficial effects (table 5), depending on specific cases and individual providers.
Self-reported impact of emotions in angry encounters and representative quotes (for participants who indicated their emotions influenced their clinical reasoning and decision-making in their angry encounter)*
Self-reported impact of emotions in positive encounters and representative quotes (for participants who indicated their emotions influenced their clinical reasoning and decision-making in their positive encounter)*
Self-reported impact of emotions in mental health encounters and representative quotes (for participants who indicated their emotions influenced their clinical reasoning and decision-making in their mental health encounter)*
Discussion
Our findings document the broad range of emotions that ED providers reported experiencing during their own recent patient encounters, including those that elicited positive emotions, negative emotions, and involved patients with mental health conditions. The emotion profiles demonstrate that providers experience a mix of discrete emotions—a finding that parallels those in the emotion literature.59 60 Notably, providers’ emotion profiles in angry and mental health encounters are strikingly similar, reflecting high levels of negative emotion.
Providers also reported significantly lower engagement in their recent encounters with patients who elicited anger or had a mental health condition compared with encounters with patients who elicited positive emotions. Further, a large majority of providers reported that their emotions influenced their clinical decision-making and behaviour in at least one encounter. Encounters that elicited anger resulted in the lowest reported quality of care. This finding, coupled with research demonstrating that anger can trigger superficial and hasty information processing (eg, stereotype use61–63), further highlights the importance of investigating the effects of frustration and anger on providers’ clinical decision-making.
Patients with mental illness are a particularly vulnerable population who experience significant healthcare disparities,34–37 contributing to a mortality gap of 15–20 years between those with and without mental illnesses.39 40 While patients with mental health conditions were found to elicit strong negative emotions, which can adversely influence providers and increase risks to patients, we also uncovered evidence of positive influences among a subset of providers. These providers reported greater empathy, spending more time with these patients, and advocating for them. Further, providers who reported greater self-assurance in mental health encounters also reported greater engagement with these patients. Together, these findings suggest that strategies that cultivate greater empathy and self-assurance among providers may hold promise for improving care for this vulnerable population.
Patients who elicit positive emotions have been a somewhat neglected subject of inquiry. Providers reported being more engaged with and providing what they perceived to be higher quality care to these patients, a finding consistent with research demonstrating that positive affect can facilitate flexible and integrative processing.64 65 In vignette studies, for example, positive affect led medical students to identify lung cancer in a patient more quickly,66 and residents to consider the correct diagnosis for a patient with liver disease sooner.67 Importantly, although positive emotions may improve patient care and safety, this may not always be the case. Positive feelings towards patients may lead providers to overtest and overtreat patients, which could expose patients to unnecessary risks. Alternatively, positive emotions may reduce a provider’s belief that a patient has a serious illness, which may result in adverse outcomes. Consistent with this possibility, research demonstrates that positive emotions are associated with predictions of positive (non-serious) outcomes.68 Future work is needed to articulate the conditions in which positive emotions are helpful versus harmful to clinical decision-making.
Using different research methods and samples of ED providers, these results converge with those from a recent large-scale qualitative interview-based investigation of physicians’ and nurses’ emotional experiences in the ED.4 Both studies reveal that providers perceive negative emotions to influence patient care both when discussing this issue in general4 and when reflecting on their own specific patient encounters. Although many providers in the interview study reported actively employing strategies to reduce the likelihood that their emotions would adversely impact clinical decision-making and patient care, results from the current study suggest that such efforts are not always successful.
In providing additional evidence that emotions can and do influence healthcare providers’ clinical reasoning and behaviour,6–9 the current findings underscore the urgency for additional education, training, and interventions to reduce adverse influences. Given that our sample consisted of experienced ED physicians and nurses, our results demonstrate that the problems of emotional influences on clinical reasoning and behaviour are not necessarily concentrated among trainees, but are more widespread. This is of concern, as experienced providers often serve in teaching and training roles and may unknowingly transmit their own emotional biases to trainees. More generally, efforts to further build emotional intelligence skills among healthcare providers will serve to increase awareness of emotions and promote effective emotion regulation strategies, and should be more fully integrated into clinical training and education, as suggested by others.4–6 8 9
At least two cognitive interventions might be considered for reducing adverse effects of emotion on healthcare providers. The first includes changing emotional experiences (via specific emotion regulation strategies); the second involves changing the effects of emotions on clinical decision-making. Research demonstrates that cognitive reappraisal—thinking about different aspects of an emotionally evocative situation—can effectively change one’s emotions.69–72 For example, rather than focusing on frustrating aspects of an encounter with an intoxicated patient, providers may direct their thoughts to other aspects of the situation, such as staff who are helping to care for the patient. By changing one’s focus of attention in this way, emotions change, and changes to clinical decision-making should follow (ie, reducing or eliminating anger should reduce or eliminate the deleterious effects of anger).
Another cognitive intervention that is well supported by social psychological research focuses on changing the effects of emotion, rather than actual emotional experience. That is, simply changing what an emotion is about changes the effects of those feelings on judgements and information processing.13 46 73–78 For example, if a clinician attributes their frustration during an encounter with an intoxicated patient to something external to the patient (eg, lack of funding for community-based detox programmes), those feelings should no longer influence clinical decision-making for that patient. Thus, the simple act of attributing one’s feelings to something other than the task at hand changes the relevance of those feelings to the task, and thereby changes their influence on the task.
Although research is needed to determine the efficacy of cognitive interventions in clinical contexts, the current investigation provides methodological and theoretical advances to the study of emotional influences on clinical decision-making. To assess the causal impact of both emotions and cognitive interventions, it is essential to have methodological tools that allow researchers to conduct randomised controlled experiments in which emotions can be elicited and effects of cognitive interventions can be studied. By adopting approaches that have long been central in social cognitive and affective science, the current study provides a means to do so and lays the foundation for a more comprehensive and systematic investigation of the role of emotions in patient safety.
Limitations
Our study has several limitations. First, we asked providers to vividly recall and describe specific patient encounters and then report their emotions and engagement during those encounters. Ideally, emotions would be measured during encounters; however, this presents practical problems given the high patient volume in many EDs and the possibility that such assessments could distract providers and adversely affect patients. Although emotions elicited during our experimental task are not identical to those that were experienced during the actual patient encounters recalled, considerable evidence (including a meta-analysis of 136 studies25) supports vivid autobiographical recall as a means to re-elicit emotions representative of those experienced during an earlier event.25 26 Moreover, a meta-analysis of 162 neuroimaging studies found that emotions experienced while recalling a past event and those experienced during an ongoing event activate the same cortical and subcortical brain regions, suggesting both share the same brain mechanisms.79–81 Thus, this method represents one effective way to capture emotional experiences, yet it produces less intense emotions than those experienced at the time of an event and is subject to recall biases.
Second, by focusing on emotional experiences in the context of recent patient encounters, this study did not capture the complexity of clinical practice. As a recent qualitative study found, providers can experience a wide array of emotions from many sources (eg, patients, hospital and system factors) during clinical practice4 and these emotions change over time. As noted earlier, this can have beneficial effects, particularly if emotions shift away from those that can adversely impact clinical decision-making. This study was not designed to assess this, but future research is encouraged.
Third, this investigation lacks objective measures of providers’ actual patient care and relied on self-reported care as a proxy. As with all self-report data, these data are potentially subject to recall biases and self-presentation concerns; thus, it is possible that self-reported care may not map onto actual care provided. However, it is more likely that some providers may have altered responses to appear more socially desirable. To the extent that this occurred, our findings may underestimate the influence of providers’ negative emotions on patients, and may overestimate the influence of providers’ positive emotions on patients.
Finally, our use of a convenience sample may reduce the generalisability of our findings. However, in contrast to much prior research that has relied on residents and medical students,82 we purposefully focused on experienced ED providers. Such providers have a broader range of patient experiences, and understanding these experiences is particularly important as researchers move forward to design and test interventions to reduce adverse impacts of emotions on patient safety.
Conclusion
The current study sheds light on a long-neglected ‘blind spot’ in the patient safety literature.5 6 10 The findings demonstrate the ubiquity and variety of emotions experienced by healthcare providers during different patient encounters, and bring much-needed attention to the possible effects of these emotions on clinical decision-making, engagement, and patient care. These findings underscore the need for education and training initiatives to promote awareness of emotional influences and to consider strategies to combat adverse effects. Importantly, the development of evidence-based interventions to mitigate emotion-induced risks to patients will require a systematic and sustained programme of research. By introducing well-established methods from social psychology, the current work paves the way for developing and testing novel interventions.
Acknowledgments
We thank Pat Croskerry and Mark L Graber for their valuable feedback and contributions to this manuscript during the review process. We also thank Ezekiel Kimball for providing helpful feedback on the qualitative aspects of this research, and Hannah Chimowitz and Nathan Huff for thoughtful comments on earlier drafts of this manuscript.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors LMI designed and managed the project. GL developed the Qualtrics program for data collection. Quantitative data were analysed by LMI and GL. All authors analysed the qualitative data; coding of qualitative data was led by JT and KB. LMI drafted the manuscript and all authors contributed to revising, editing and finalising the manuscript. All authors approved the final version of the manuscript.
Funding This project was funded by the Agency for Healthcare Research and Quality (AHRQ; grant number R01HS025752), US Department of Health and Human Services (HHS) awarded to LMI.
Disclaimer The authors are solely responsible for this document’s contents, findings and conclusions, which do not necessarily represent the views of the AHRQ. Readers should not interpret any statement in this report as an official position of AHRQ or of HHS.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The Institutional Review Board at the University of Massachusetts Amherst approved this study (protocol number 2016-3291).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. Data generated for this study include confidential and sensitive information in the form of written patient encounter descriptions and reports of clinical behaviours. These data are not available for sharing.