Article Text

Statistics from Altmetric.com
Overprescribing of antibiotics in primary care is one of the important drivers of antimicrobial resistance (AMR) internationally.1 Previous studies estimated that one-fifth to one-third of UK antibiotic prescriptions in primary care are unnecessary or inappropriate.2 The study by van Staa and colleagues3 published in this issue of BMJ Quality & Safety delivers additional insights into prescribing practices by primary care physicians (general practitioners, GPs) in the UK. Analysing data from more than 6000 GPs in 466 general practices between 2012 and 2017, they found large variability in prescribing practices as measured, for example, by the overall antibiotic prescribing rate per consultation, the percentage of patients receiving repeat prescriptions and the use of broad-spectrum antibiotics. The percentage of repeat prescriptions (ie, antibiotics that were prescribed within 30 days of another antibiotic prescription) ranged from 13.1% to 34.3%, with a mean of 23.2%. They also found that patients prescribed an antibiotic during the study period had a mean of 8.9 antibiotic prescriptions (SD=6.1) in the 3 years prior to the study, indicating that regular antibiotic use is common for a substantial group of patients.
The authors highlight considerable variability in case mix, with some clinicians facing greater challenges due to the high baseline risk of microbial infection among their patients. Using Poisson generalised additive mixed effect models, it is proposed that the largest potential reduction in antibiotic prescribing could be achieved through risk-based prescribing, especially for patients receiving repeat prescriptions. It is also suggested that reducing repeat antibiotic courses to the prescribing habit of a median clinician would save 21 813 antibiotic prescriptions per 1000 clinicians per year. If this was further reduced to the lowest 25th percentile, this would result in 38 871 fewer antibiotic prescriptions per 1000 clinicians per year.
van Staa and colleagues’3 repeat prescription rates are higher than those from a 2002–2017 UK cohort study,4 which reported a median percentage of 10% of antibiotics being repeat prescriptions. However, the mean figure of 23.2% is still lower than the results from a study on UK care home prescribing,5 which suggested that 30% of antibiotic prescriptions met the definition of repeats. In the UK care home study, the antibiotics that were most frequently repeated for long durations were azithromycin, cephalexin, nitrofurantoin and trimethoprim. These medicines were usually recommended for use as prophylaxis for chronic obstructive pulmonary disease and urinary tract infections. A different UK study showed that most repeat antibiotic prescriptions occurred in the absence of a specific coded clinical condition, suggesting that repeat prescriptions were potentially used as treatment in cases of clinical uncertainty.6
Defining repeat prescriptions
One problem with discussing the role of repeat prescribing in the context of antibiotic overuse is the difficulty of defining repeat prescriptions. van Staa and colleagues’3 definition includes any antibiotic prescribed within 30 days of a previous prescription for the same drug. Other studies used different durations (eg, 35 days5) or different definitions altogether (eg, any antibiotic prescription—other than the first—that occurred in a sequence of prescriptions for the same drug4 6). The different definitions may account for some of the variation observed in the statistics around repeat prescriptions. Additionally, existing definitions appear to confound two different types of repeat prescribing. The first type refers to long-term repeat prescriptions for chronic conditions taken continuously with little or no break. The second type refers to short-term repeat prescriptions for acute problems that have not resolved after a single course of antibiotics or are due to additional infections occurring within a set period.
In the UK, long-term repeat prescriptions are preauthorised prescriptions for medications that patients can request without the need for consultation each time. They are typically offered to patients who require medications for long-term use as part of management of chronic illnesses. Long-term use of antibiotics may occur as part of prophylaxis for infection. Short-term repeat prescriptions, on the other hand, refer to repeated courses of antibiotics that are prescribed following patients’ reconsultations for the same or different infections within a specific time period, such as 6 months.
Most GP prescribers follow the guidelines of 28-day prescription courses, meaning that long-term repeat prescriptions get reissued each month.7 Consequently, previous study definitions are unlikely to allow for a more nuanced analysis and comparison of antibiotic overuse based on long-term versus short-term repeat prescriptions. For the purpose of this editorial, we will therefore consider both types, jointly referring to them as ‘repeat’ prescriptions.
GPs in the UK use electronic systems to manage repeat prescriptions, but previous research has highlighted problems with electronic prescribing that can increase the risk of inappropriate ongoing medication use.8 These problems linked to the automation of prescription approvals can lead to deficiencies in appropriate authorisation and review procedures. Recent studies suggest that long-term antibiotic use holds little benefit for most patients.9 In fact, repeat prescriptions for antibiotics appear to predict higher long-term risks of infection-related hospitalisation,9 and this may be due to biological mechanisms of dysbiosis (ie, disruption to the gut microbiota). In addition, the negative impact of the COVID-19 pandemic on judicious antimicrobial prescribing has been reported. For example, GPs reported lower thresholds for antibiotic use for respiratory symptoms, especially at the start of the pandemic.10
In the context of previously identified challenges with repeat antibiotic prescriptions, which may have been further aggravated by the recent pandemic, 'findings by van Staa and colleagues3 highlight the necessity to reduce repeat antibiotic prescribing as part of a menu of options to tackle AMR.
The psychology of repeat prescriptions
To change prescribing behaviour it is essential to consider possible psychosocial drivers of current treatment practice. Several interdependent psychological factors are likely to play a role.
Decision biases
Research from behavioural sciences has repeatedly demonstrated the power of cognitive biases that affect decision-making in a systematic way. Indeed, a recent editorial highlighted specific biases resulting from diagnostic uncertainty in the context of antibiotic prescribing for acute medical patients in secondary care.11 In the context of repeat prescriptions by GPs, slightly different cognitive mechanisms are likely to play a role. This includes the ‘status quo bias’, which describes a human tendency to maintain the status quo as a default, even if a strategy change could have preferable outcomes. It is closely related to ‘omission bias’, which refers to an irrational preference for errors that are based on omission as opposed to active choices. Previous research has highlighted that both patients and doctors are susceptible to these biases.12 Qualitative data from secondary care indicate a hesitancy to de-escalate or discontinue antibiotic courses even when patients were improving, with common reasons including reluctance to ‘change a winning team’.13 It is likely that similar motivations underpin the hesitancy to discontinue repeat prescriptions in primary care, particularly if the antibiotic was initiated in secondary care.
Decision inertia
The status quo bias is also linked to ‘decision inertia’, which refers to a tendency to prefer decisions associated with lower cognitive effort. Critical reviews of repeat prescriptions can be considered time-consuming and require more effort than choosing to maintain the status quo. Given time constraints in general practice, pressures exist to minimise workload and this may contribute to patient prescriptions not being reviewed.8 Previous research provided evidence that limited time and cognitive resources may shape antibiotic treatment choices, with hospital doctors describing antibiotic prescribing as an ‘easy’ option, especially out of hours.14 Cognitive effort is likely to be even further reduced when choosing to continue a previous course of medication in general practice.
Social norms
It is commonly recognised that the culture of a healthcare environment affects the prescribing habits of local doctors. Indeed, previous research identified dominant prescribing etiquettes, often shaped by social and professional hierarchies, that influence antibiotic prescribing choices.15 For example, professional culture may reduce the likelihood to query another clinician’s choice for a repeat prescription, especially if the initial prescriber is perceived to be senior or perhaps a specialist, either in terms of professional experience or level of training or education. Furthermore, contradicting a colleague and communicating inconsistent advice to patients may be considered bad practice that could contribute to undermining other healthcare colleagues.16
Diffusion of responsibility
Another psychological factor promoting the overuse of repeat prescriptions may be diffusion of responsibility. A passive decision to continue treatment initiated by a previous prescriber is likely to reduce the current clinician’s perceived responsibility for any associated outcomes. In the event of an adverse outcome, the original prescriber is likely to bear the burden of consequent complaints or investigations. Indeed, previous research has highlighted the fear of litigation to be an important driver of antibiotic decision-making in secondary care,17 and similar factors may play a role in repeat prescribing choices in general practice.
Strategies for reducing/avoiding inappropriate repeat antibiotic prescriptions
To address the problem of repeat antimicrobial prescribing and promote behaviour change, we propose that psychosocial drivers of repeat prescribing be considered when designing control mechanisms or interventions (figure 1). To reduce the effects of status quo and omission biases, the electronic environment of existing prescribing systems may need to be adapted. Care must be taken not to highlight the continuation of a repeat prescription as a default. This could be achieved by introducing system barriers that prompt more thorough reviews and increase cognitive resources invested into the process of authorising repeat courses of antibiotics. Some relevant success has been reported by an Australian study, which found that the removal of system defaults resulted in dramatic changes to antimicrobial prescribing.18 Additionally, UK tools such as the national TARGET (Treat Antibiotics Responsibly, Guidance, Education and Tools) antibiotic toolkit19 or the structured medication review,20 which requires an investigation of patients’ experience of repeated antimicrobial prescribing, offer opportunities for improvement.
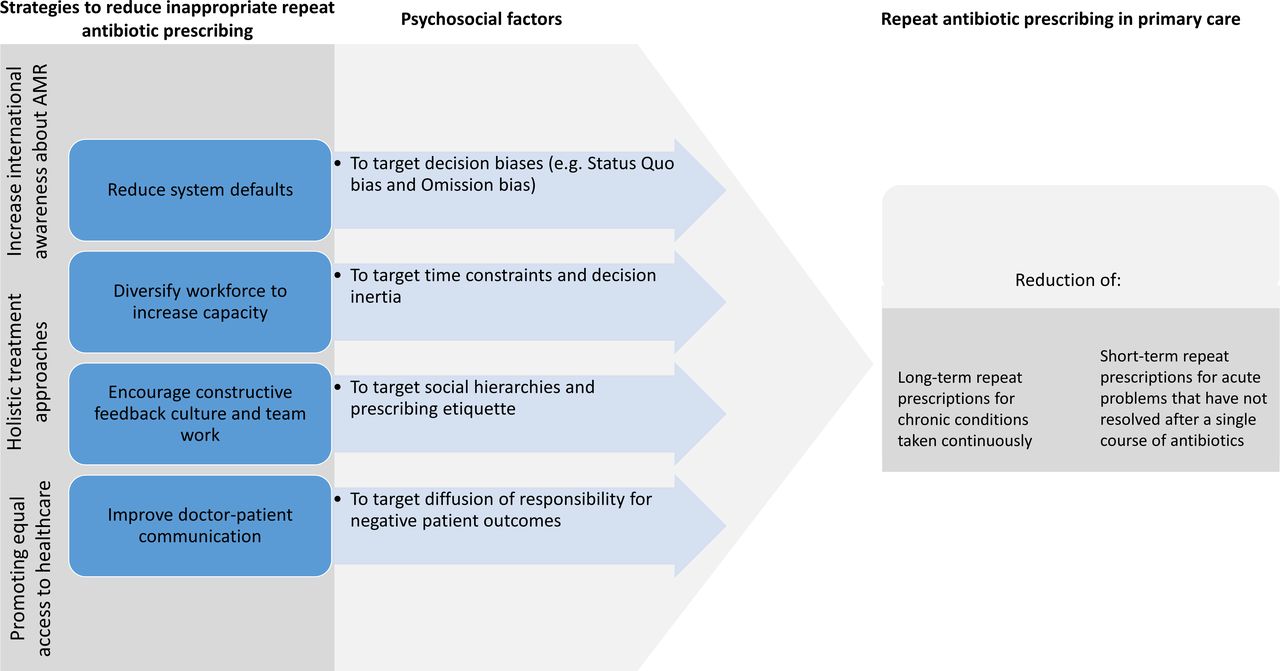
{kind=link}
Strategies to reduce inappropriate long-term and short-term repeat antibiotic prescribing.
Tackling time constraints and related issues of decision inertia may require a review and extension of traditional prescriber roles. Initial advances have been made in this regard. Primary care workforce variation is ongoing globally, especially in Canada, USA, Australia and the UK. With the role of pharmacists rapidly developing within general practice, there is significant opportunity for their input. Increasing the confidence for general practice and community pharmacists to review patients on repeat antibiotics through continuous training and availability of specialised toolkits would be important. With longer appointment times and specialised toolkits available to aid clinical review, pharmacists can be considered well positioned to address some of the barriers.21
Shifting existing social norms and establishing a critical but constructive feedback culture across different healthcare professions are long-term challenges that may be aided through enabling more group-based decision-making approaches11 and creating habits of collegial reviews. Repeat antibiotics can occur through a variety of avenues in general practice and it is important to identify how social norms may affect these different pathways and contribute to acute prescriptions becoming long term. One option might be to introduce routine reviews of discharge summaries from secondary care physicians through the primary care team (pharmacists, nurses and doctors). This could prevent inappropriate hospital prescriptions from being added to the patient’s repeat medication list.
The psychological drive to diffuse responsibility by continuing antimicrobial prescriptions of other physicians is often linked to a fear of patient complaints and litigation. Research has highlighted that general practices with antibiotic prescription rates below the national mean had lower scores on patient satisfaction.22 On the other hand, studies also suggest that patient satisfaction results from patients’ better understanding of their infection, their doctors’ treatment choice and the overall context of AMR.23 Hence, unhelpful strategies of defensive medicine and overprescribing could be replaced with greater efforts to enhance doctor–patient communication and improve patient knowledge. These will need to be implemented alongside ongoing encouragement of ‘safety-netting’ for prescribers11 and continued efforts to increase healthcare staff and public awareness. National and international campaigns, such as Keep Antibiotics Working (UK), Be Antibiotics Aware (USA) and World Antimicrobial Awareness Week (WHO/Global), have sought to promote antimicrobial awareness. The ongoing international pledge-making Antibiotic Guardian campaign can contribute to behaviour change and impact individuals’ action to tackle the spread of AMR.24
It is worth noting that, in some cases, repeated courses of antibiotics or antibiotic prophylaxis are clinically warranted, for example for treatment of a chronic infection. Long-term prophylaxis with antibiotics is also critical for some, for example people who have undergone a splenectomy or have sickle cell disease. Clinical reviews of patients receiving repeat prescriptions of antibiotics should take a holistic approach to understand patient perspectives and goals. Shared decision-making should be encouraged and patients should be informed about alternatives to antibiotics (where available) and the potential harms of antibiotics, both in terms of adverse effects (eg, nitrofurantoin-induced hepatitis) and impact on microbiota, as well as risk of future infection with antibiotic-resistant pathogens.
Finally, whatever interventions are to be developed, it is important to consider health inequalities to avoid the risk of certain groups not benefiting from the same access to healthcare. Current examples include context-dependent underuse of antibiotics (eg, in the rural Maori population of New Zealand25).
Conclusions
Addressing inappropriate repeat antibiotic prescribing may have a strong potential to reduce antibiotic overprescribing in primary care. We highlight psychosocial drivers of repeat antibiotic prescriptions and propose mechanisms for considering these drivers when designing interventions. Based on our review of theory and relevant international research, we make actionable recommendations to incorporate new behaviours and enact positive change.
Further work is needed to understand the respective scales of long-term and short-term repeat antibiotic prescribing across different care sectors and to develop specific interventions to support the review of repeat antibiotics for the most common infections and frequently prescribed antibiotics.
Ethics statements
Patient consent for publication
Acknowledgments
Rachel Francis-Nweke, Clinical Pharmacist General Practice & The Ambulance Service is acknowledged for commenting on the article prior to submission.
References
Footnotes
Twitter @EM_Krockow, @E_J_Harvey, @DrDianeAshiru
Contributors DA-O and EMK conceived the paper. EMK, DA-O and EJH drafted the paper, modified the subsequent drafts and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests EMK is coinvestigator on a recently (January 2022) awarded PhD studentship by the Midlands Graduate School ESRC DTP and receives royalties for her online publications on Psychology Today.
Provenance and peer review Commissioned; internally peer reviewed.