Article Text

Abstract
Objectives To determine the proportion of hip fracture patients who experience long-term disability and to re-estimate the resulting burden of disease associated with hip fractures in Australia in 2003.
Methods A literature review of the functional outcome following a hip fracture (keywords: morbidity, treatment outcome, disability, quality of life, recovery of function, hip fractures, and femoral neck fractures) was carried out using PubMed and Ovid MEDLINE.
Results A range of scales and outcome measures are used to evaluate recovery following a hip fracture. Based on the available evidence on restrictions in activities of daily living, 29% of hip fracture cases in the elderly do not reach their pre-fracture levels 1 year post-fracture. Those who do recover tend to reach their pre-fracture levels of functioning at around 6 months. These new assumptions result in 8251 years lived with disability for hip fractures in Australia in 2003, a 4.5-fold increase compared with the previous calculation based on Global Burden of Disease assumptions that only 5% of hip fractures lead to long-term disability and that the duration of short-term disability is just 51 days.
Conclusions The original assumptions used in burden of disease studies grossly underestimate the long-term disability from hip fractures. The long-term consequences of other injuries may similarly have been underestimated and need to be re-examined. This has important implications for modelling the cost-effectiveness of preventive interventions where disability-adjusted life years are used as a measure of health outcome.
- Hip fracture
- burden of disease
- quality of life
- disability
- fracture
- public health
Statistics from Altmetric.com
Introduction
Expenditure on health in Australia, as is the case in most countries, is increasing at a faster pace than other sectors of the economy.1 As a consequence, there is a growing emphasis on providing medical care that provides the best value for money. Burden of disease and cost-effectiveness of health interventions are important elements of the evidence base to support priority setting. Accurate information on the fatal and non-fatal consequences of diseases and injuries is essential.
Hip fractures occur predominantly in the elderly population but they can be prevented through interventions that prevent falls and osteoporosis. To evaluate the cost-effectiveness of interventions to prevent hip fractures it is necessary to estimate the health outcomes associated with hip fractures. The non-fatal component of burden of disease is calculated in years lived with disability (YLD). This metric was developed as part of the disability adjusted life year (DALY) measure for the Global Burden of Disease study (GBD) in the early 1990s.2 The GBD was developed as a way of measuring disease burden attributed to 190 conditions using a consistent measurement to enable comparisons. Essentially, YLD combines the number of incident cases (I) with the average duration of a disease (D) and a measure of severity, the disability weight (DW) using the equation YLD=I × D × DW.
In previous versions of the GBD and the Australian Burden of Disease and Injury study, all hip fracture cases are given a disability weight of 0.372 (ie, a 37.2% decrement in health) for an initial period of 51 days for treated cases and 88 days for untreated cases.2 3 It is assumed that 5% of treated and 50% of untreated fractured femur cases have lifelong disability at a disability weight of 0.272. The estimate of the proportion of cases experiencing long-term disability is based on expert opinion rather than empirical evidence. The long-term rather than the short-term health consequences determine much of the disability estimated for hip fractures.
The aim of this research was to find evidence to evaluate the key assumption that 5% of hip fracture cases experience lifelong disability used in burden of disease studies in Australia, where all hip fracture cases are assumed to receive treatment, in preparation for an economic evaluation study of osteoporosis preventive treatments (in which health benefits are expressed in disability adjusted life years).
Methods
Literature review
A review of the literature was conducted to locate follow-up studies of injury cohorts that report on the long-term disabling sequelae of hip fractures. Computerised searches of MEDLINE and PubMed from 1990 to March 2006 were undertaken. This timeframe was chosen to account for advances in fracture surgery, treatment, and rehabilitation that improved outcomes from 1990 onwards.4–6 Keywords and subject headings in the searches included: morbidity, treatment outcome, disability, quality of life, recovery of function, hip fractures, and femoral neck fractures. Studies published in foreign language journals and unpublished dissertations and theses were not included. There were no restrictions placed on publication type, although it was anticipated that the majority of included publications would be cohort or case–control studies in the general population. Studies were excluded if they reported on only one specific treatment such as cementing, internal fixation, or hemi-arthroplasty as this is not representative of the current treatment pattern of incident fractures.7 Studies were also excluded if they only included a subgroup of patients such as those with a mental disorder. Studies were only included if duration of follow-up was ≥1 year.
All studies reporting similar outcomes were combined regardless of participants' age or sex. As most studies did not report on outcomes by age and as the studies included only small numbers of patients they were under-powered to present age–sex specific results.
Burden of disease estimation
The 2003 Australian Burden of Disease and Injury Study estimated the morbidity associated with hip fractures in terms of the total YLD.3 This required estimation of the number of incident hip fracture cases during 2003. This information was sourced from the Australian Institute of Health and Welfare National Hospital Morbidity Database. It was assumed that all hip fractures were treated in hospitals and those that were treated outside the hospital system did not result in significant disability. For each incident case the total YLD was obtained by multiplying the average duration of the condition by a disability weight. A discount rate of 3% was applied which was consistent with the measurement of health outcomes in cost-effectiveness analyses. The formula used for calculating YLD is shown in equation 1:
YLD estimates were based on the GBD assumptions. All hip fracture cases were assumed to have an initial disability lasting 51 days with a disability weight of 0.372, and 5% of cases were assumed to suffer lifelong disability with a disability weight of 0.272. New YLD estimates using equation 1 were calculated based on results of the literature review. In particular the proportion of patients experiencing lifelong disability and the average short-term duration were varied for incident hip fracture patients aged 60 years and over.
Results
Functional outcome
Figure 1 shows the results of the search strategy, including source of the studies and subsequent culling. Twenty-five studies were selected from the literature review and included in the analysis. Length of follow-up was predominantly 1–2 years and subjects were mostly aged 50 years and over. The study with the largest number of hip fracture patients included 1169 patients from Japan.8

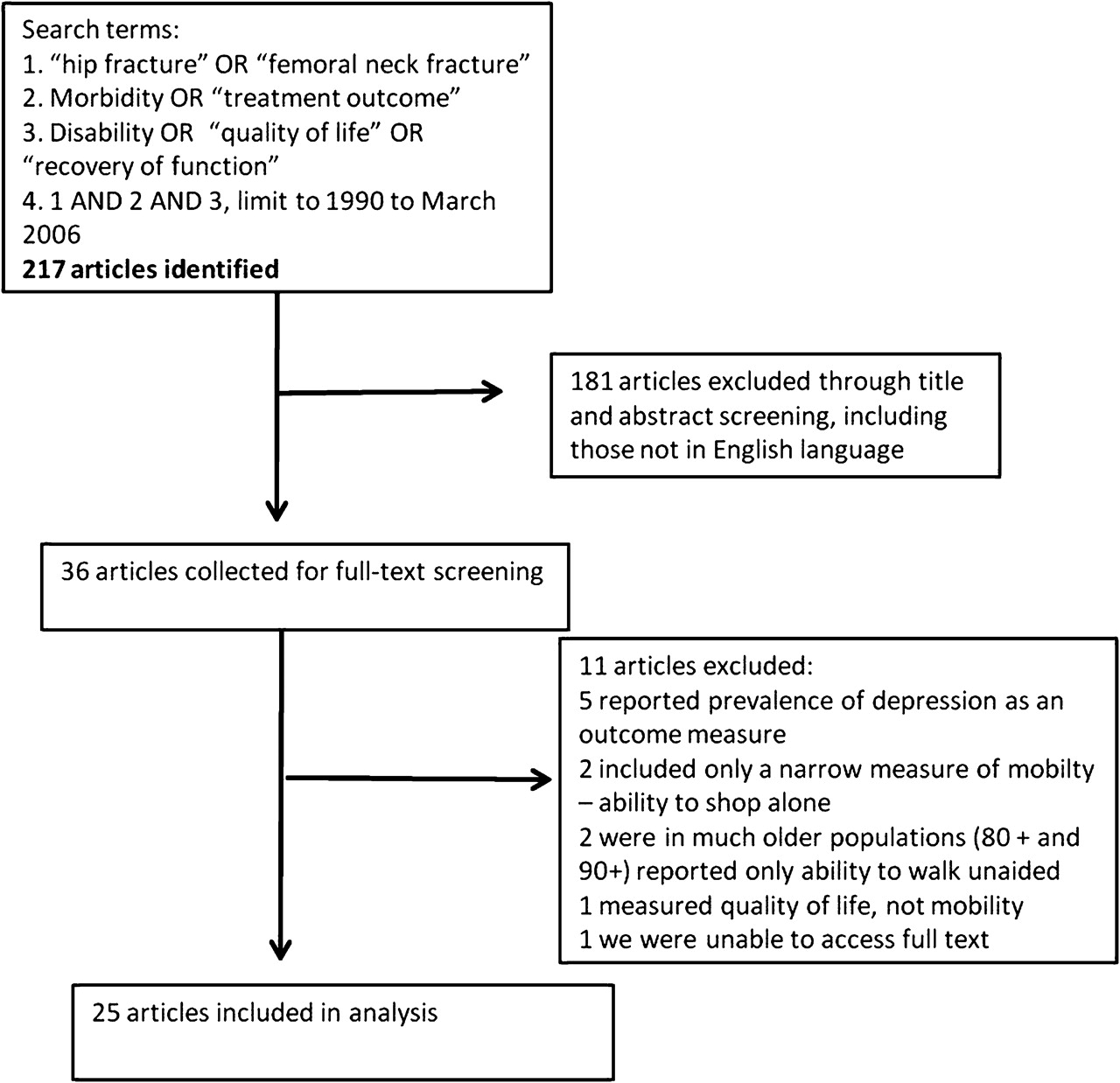{kind=link}
Flow diagram (selection strategy) of included studies.
There was a wide range of scales and scoring systems used to measure the quality of life and functional and mental recovery after a hip fracture. Some measures were generic and could be applied to a range of diseases. Others were specific to osteoporosis as low bone mineral density is a risk factor for hip fractures. Scales and ratings that were used to assess health outcomes included:
Short Form 36 (SF-36)
Cummings hip scale
Rapid Disability Rating Scale version 2 (RDRS-2) questionnaire
Mini-Osteoporosis quality of life questionnaire
Osteoporosis Assessment Questionnaire (OPAQ)
Short Form 12 (SF-12)
Quality of life questionnaire of the International Osteoporosis Foundation (QUALEFFO)
QUALIOST® (QUAlity of Life questionnaire In OSTeoporosis)
Miltner's rating scale
EQ-5D questionnaire
Katz index of independence in activities of daily living
Lawton instrumental activities of daily living scales
Mobility Social Care Living (MSCL) score
Chinese Barthel Index (CBI)
Lawton and Brody's Instrumental Activities of Daily Living dependency scale
Groningen activity restriction scale
Commonly reported outcomes were mobility, pain, activities of daily living, and living situation. For each prospective study the difference between the proportion of patients with disability pre-fracture and post-fracture was calculated and the difference was attributed directly to the hip fracture. For case–control studies the difference between those with fracture and those without fracture was attributed to the hip fracture. A weighted average (weight=sample size) was calculated for each of the commonly reported outcomes to determine the proportion of cases with long-term disability as a result of a hip fracture. As the studies did not all report on each outcome, not all studies are included in each weighted average.
Twenty-five studies (table 1) were included in the analysis of the proportion of hip fracture patients suffering from long-term disability problems. Based on a weighted average of relevant studies, 20% of subjects with a fracture were no longer able to shop independently as a result of the fracture13 27 28 and 42% of patients with a fracture had not returned to their pre-fracture mobility levels after 1 year.8 15 16 18 26 29 Thirty-five per cent of hip fracture patients were unable to walk independently as a result of the fracture 14 20–22 24 27 and 14% were no longer able to climb stairs independently.20 27 28
Included studies for long-term disability measures after hip fracture
Assuming no pain prior to a hip fracture, 47% of patients reported pain one or more years post-fracture.11 18 23 24 27 Approximately 23% reported mild pain, 24% moderate pain, and 2% severe pain.
After one or more years, 71% of hip fracture patients regained their pre-fracture level of activities of daily living14 17 31 and 29% went on to experience lifelong disability. Studies reported large variations in terms of functional recovery with a weighted average of the percentage of people recovering after 1 year of 68%.15 17 18
In terms of residency, 23% of hip fracture patients moved to a more dependent state of living and remained in that state at least 1 year after a hip fracture. These were predominantly community dwelling residents prior to a fracture moving into residential care.9 10 12–14 16 19 22 25 27 30 32–34 Based on three case–control studies the probability of moving from community to a more dependent state was 16–22% greater for hip fracture patients compared with controls.10 14 19
Burden of hip fractures
Based on the literature review we conclude that the GBD assumption that 5% of incident hip fracture cases have lifelong disability underestimates the true disability impact of hip fractures. Increasing the proportion of people aged 60 years or above with long-term disability from a hip fracture from 5% to 29% (the proportion not regaining their pre-fracture levels of activities of daily living) results in a 3.6-fold increase (from 1831 to 6667) in the YLD for hip fractures in Australia in 2003.
We also found evidence that functional recovery after a hip fracture may take up to 4–6 months.15 16 30 35 This suggests that the GBD assumption of 51 days duration for short-term disability may also be an underestimate. Applying a short-term duration of 6 months and assuming that 29% of hip fracture cases aged 60 years and older experience lifelong disability results in a 4.5-fold increase in YLD (from 1831 to 8251 YLD) compared to the previous estimate using GBD assumptions. If we conservatively assume that only the 23% who move to a higher dependency state of living, which is the only outcome measure reported in all 14 studies, have long-term disability, this would result in a 3.6-fold increase (from 1831 to 6723 YLD), whereas if we assume all of the 42% who did not recover full mobility to have long-term disability, this increases the YLD 6.9-fold (1831 to 12 646 YLD). This increase is largely due to the changed assumption on the proportion suffering long-term disability and only slightly dependent on the change in duration of those suffering short-term disability. We have not considered a change to the DW of long-term hip fracture. Future work should consider this as a change to this disability weight may significantly alter the conclusions again.
Discussion
In 1996, the GBD study reported that ‘the literature on the disabling sequelae of injuries is very limited’.2 This review found that there currently is a large published literature base reporting on the long-term outcomes associated with hip fractures. Although a review of disability following hip fractures was carried out in the early 1990s,36 this is the first review to include a pooled estimate for each of the commonly reported outcomes to determine the proportion of cases with long-term disability as a result of a hip fracture. There exists scope to further expand this research to other fracture types and injury categories.
In addition to duration and incidence, another important aspect of measuring YLD is the utility value or disability weight that is assigned to each health state. The GBD study assigns a disability weight of 0.372 to short-term cases of fractured femur and 0.272 to cases with lifelong disability. There is also a large amount of published literature on the health state utility values for hip fractures (note that utility weights value ‘remaining health’ and disability weights value ‘health loss’; thus a utility value compares with the complement to one of a disability weight). Brazier et al conducted a systematic review and found a wide range of utility estimates for hip fracture between 0.28 and 0.72.37 Studies are also being conducted in Australia to evaluate how well instruments measure the impact of injury on health-related quality of life. Watson et al administered the Assessment of Quality of Life (AQoL) and the SF-36 to 221 admitted injury patients in Victoria. They conclude that the AQoL could be useful for estimating the burden of disease associated with injuries and for use in the evaluation of treatment and rehabilitation interventions.38 Updating disability weights also has the potential to make a valuable contribution to the burden of disease associated with injuries.
The long-term disability weight of 0.272 is relatively high; in effect a person loses 27% of their health for the remainder of their life. This is akin to the disability weight that is used in stroke survivors and congestive heart failure. Given the potential loss of function from a hip fracture, and the range of utility estimates presented in the literature, we continued to use this weight. Further research into quantifying the severity of long-term disability from hip fractures would make results more accurate. This research is being undertaken within the current global burden of disease project for 2005.39
Defining the length of time post-fracture that can be classified as ‘long-term’ is important. If this period of time is too short, one would overestimate long-term disability as recovery is still not complete. If the length of time is too long this too will overestimate the disability associated with fractures due to a decline in health status from other causes. As hip fractures predominantly occur after the age of 60 years, subjects are elderly at the time of the fracture and their general health status is likely to deteriorate over time even without a fracture. It is therefore difficult to determine to what extent the decline in physical and mental function is directly related to the hip fracture or to other co-morbid conditions.
Based on the available evidence, maximum recovery from hip fracture is achieved by 1 year and possibly even by 6 months. Koot et al report that the chance of a patient with a hip fracture making any further recovery after 4 months is minimal.15 Magaziner et al report that functional status improves over the first year post-fracture but the time to recovery varies by functional domain. Recuperation from depressive symptoms takes 4 months compared with just over 11 months for lower extremity function.35 This is supported by Shyu et al who report that it took more time for patients to recover to pre-fracture level of function for the more difficult and complex activities and that most functional improvement occurs in the first 6 months following hospital discharge.29 Other studies report that recovery is nearly complete at 6 months with little change in the proportion not recovered between 6 months and 1 year.16 40
Thus by restricting this review to studies that had a follow-up of ≥1 year ensures that the disability from the hip fracture reported is long-term. Follow-up in most studies was between 1 and 2 years, a short enough period to suggest that the measured disability is directly as a result of the hip fracture rather than due to co-morbid conditions. Given that the estimates obtained come from the international literature, the estimate that 29% of hip fractures result in long-term disability is applicable to other burden of disease studies in high income countries where all hip fractures are treated. As most of these studies were undertaken in high income countries, care should be taken in applying the result in low and middle income countries as lack of access to healthcare could cause a higher proportion of people to suffer long-term consequences. Conversely, given the younger age structure of populations in low and middle income countries and the strong link between age and the cause of hip fractures, it could also be argued that a lower percentage of people in those countries may go on to long-term disability.
A limitation of this study is that estimates are not age and sex specific. This assumes that there are no statistically significant differences in outcomes between men and women or by age. This is supported by Endo et al who report that 1 year post-fracture there were no statistically significant gender differences in residential status, help level, or functional recovery (reaching pre-fracture levels of ambulation, basic activities of daily living, and instrumental activities of daily living).41 Parker and Palmer report that although there are no significant differences in rehabilitation post-hip fracture between men and women, age is a significant predictor.42 Although the study populations were homogeneous in that they included elderly men and women (aged 50 years or above) there is still likely to be significant heterogeneity in terms of pre-fracture residential status, cognitive status, physical function, and pre-existing medical conditions. These factors have been shown to be associated with recovery after a hip fracture.16 43 44
Conclusion
Estimating the long-term disability associated with hip fractures is not straightforward as there are a variety of scales and outcome measures used to measure quality of life. This review found that there is a large published literature base on the disabling sequelae of hip fractures and some common outcomes exist between studies. Results from the studies can be combined together to provide more reliable estimates of the long-term health outcomes associated with hip fractures.
Based on a review of the literature the 5% estimate of long-term disability used in burden of disease studies appears to underestimate the true extent of long-term disability due to hip fractures. Varying the short-term duration and the percentage of patients with lifelong disability based on this review results in a 4- to 7-fold increase in YLD due to hip fractures in Australia in 2003. This new information should also be incorporated into economic evaluations of interventions to prevent hip fractures. This review provides more robust estimates for cost-effectiveness analyses as a greater amount of health gain would be expected from falls prevention and fracture treatment interventions.
What is already known on this subject
Hip fractures are associated with increased mortality and impaired function.
The non-fatal burden of disease associated with hip fractures can be estimated using years lived with disability (YLD).
Previous estimates of the YLD for hip fractures have assumed low rates of long-term disability.
What this study adds
The burden of disease associated with hip fractures is much higher than current estimates suggest.
The long-term consequences of hip fractures contribute 76% to the overall YLD.
Interventions to prevent hip fractures (eg, falls prevention) will yield greater health benefits than previously thought.
References
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.