Article Text

Abstract
Objectives To determine the incidence and nature of prescribing and medication administration errors in paediatric inpatients.
Design Prospective review of drug charts to identify prescribing errors and prospective observation of nurses preparing and administering drugs to identify medication administration errors. In addition, incident reports were collected for each ward studied.
Participants Paediatric patients admitted to hospitals and nurses administering medications to these patients.
Setting 11 wards (prescribing errors) and 10 wards (medication administration errors) across five hospitals (one specialist children’s teaching hospital, one nonteaching hospital and three teaching hospitals) in the London area (UK).
Main outcome measures Number, types and incidence of prescribing and medication administration errors, using practitioner-based definitions.
Results 391 prescribing errors were identified, giving an overall prescribing error rate of 13.2% of medication orders (95% CI 12.0 to 14.5). There was great variation in prescribing error rates between wards. Incomplete prescriptions were the most common type of prescribing error, and dosing errors the third most common. 429 medication administration errors were identified; giving an overall incidence of 19.1% (95% CI 17.5% to 20.7%) erroneous administrations. Errors in drug preparation were the most common, followed by incorrect rates of intravenous administration.
Conclusions Prescribing and medication administration errors are not uncommon in paediatrics, partly as a result of the extra challenges in prescribing and administering medication to this patient group. The causes and extent of these errors need to be explored locally and improvement strategies pursued.
Statistics from Altmetric.com
Introduction
Medical errors are a major issue in healthcare.1,–,5 Medication errors are probably one of the most common types of medical error, and include prescribing, dispensing and medication administration errors.6 7 In adults, it has been estimated that medication errors cause harm in 1–2% of patients admitted to UK and US hospitals.8 9
Limited evidence suggests that the prevalence of medication errors and corresponding harm could be higher in children than in adults.10 This may be because most drug doses in paediatric medication are calculated individually, based on the patient’s age, weight, body surface area and/or their clinical condition. Furthermore, the majority of drugs used in children are unlicensed or off-label.11 12 This may increase the potential for medication errors and risks associated with extemporaneous dispensing as adult dosage forms are used for paediatrics.13 14
In children, prescribing and medication administration error rates vary between studies depending on the definitions used and setting investigated.14 There have been two studies investigating paediatric prescribing errors in the UK, one showing an error rate of 5.3% and the other not reporting a rate.15 16 However, no large-scale study has investigated the current incidence of paediatric prescribing errors in the UK. Furthermore, we do not know the incidence of medication administration errors in paediatrics in the UK, as there have been only two small observation-based studies carried out. Each investigated medication administration errors in one hospital; the incidence varied between 1.2% and 5.1% of administrations.15 16 Other UK studies have collected incident reports to investigate the types and nature of paediatric medication errors in general;17,–,20 however, these studies will significantly underestimate their incidence.21 22
What is already known about this topic
Medication use in paediatrics is particularly prone to error.
Limited evidence from the US suggests that medication errors and corresponding harm could be higher in children than in adults.
There have been no large-scale studies to investigate the incidence of prescribing and medication administration errors in the UK; hence, the epidemiology of medication errors in the paediatric inpatient setting in the UK is unclear.
What this study adds
Prescribing errors are common in paediatric inpatients in the UK; around 13.2% of medication orders written contain an error.
Medication administration errors are also common in paediatric inpatients in the UK; these occurred in around 19.1% opportunities for errors.
The nature and the types of prescribing errors and medication administration errors in paediatrics are similar to those reported in previous research.
Although most errors detected were unlikely to cause serious harm, a small number of cases are potentially fatal; therefore, it is important to develop strategies in the UK to minimise paediatric medication errors.
The aim of this study was to investigate the incidence and nature of both prescribing and medication administration errors in paediatric inpatients across several different London hospitals in the UK.
Participants and methods
Ethical approval was obtained from a Multicentre Research Ethics Committee.
The study was conducted in the London area. At the time of this study, there were 23 hospitals in London that cared for paediatric inpatients. Of these, five were non-teaching, and 18 were teaching hospitals. It was decided to purposively select five hospitals based on the 4:1 ratio of teaching to non-teaching hospitals. The five hospitals selected were one specialist children’s teaching hospital (hospital A), three general teaching hospitals (hospitals B to D) and one non-teaching general hospital (hospital E). Wards within each hospital were chosen to obtain a wide range of settings representing surgical, medical and intensive care paediatric inpatients.
All five hospitals operated a typical British ward pharmacy service, in which doctors wrote prescriptions on formatted inpatient drug charts, which the nurses used to determine the drugs and doses due and record their administration. One hospital (hospital A) had a Centralised Intravenous Additive Service (CIVAS). At the time of the study, none of the hospitals employed any electronic prescribing or electronic decision support. Ward pharmacists reviewed drug charts on weekdays to check whether medication orders were clinically appropriate, clear and legal, and to initiate the supply of medications not stocked on the ward.
Identification of errors
Identification of prescribing errors
A practitioner-led definition was used:23
A clinically meaningful prescribing error occurs when, as a result of a prescribing decision or prescription writing process, there is an unintentional significant:
Reduction in the probability of treatment being timely and effective or
Increase in the risk of harm when compared with generally accepted practice.
This definition is accompanied by lists of scenarios that should be included and excluded as errors, was specifically adapted for use in paediatrics23 and has been used by the Department of Health.3 It has the advantage of referencing error to usual practice, and of not artificially inflating the error rate by including trivial incidents or breaches of inappropriate guidance.
We chose a prospective review of drug charts to collect data. The ward pharmacists for the study wards identified prescribing errors during their ward visits according to their normal clinical practice. Data collectors accompanied the pharmacists and documented any errors identified. To aid the reliability of data collection, pharmacists were given a 1 h training session on the prescribing error definition and events which should be included or excluded as errors; we focused on prescribing errors rather than pharmacists’ interventions.
Data were collected every week day for two consecutive weeks in each of the 11 wards at the five hospitals during 2004/2005.
There were five data collectors (including the principal investigator), and they shadowed a total of 10 pharmacists. All pharmacists were experienced in paediatrics. The data collectors were given training and advice from the principal investigator on the methods used and what information to collect. Each of the data collectors conducted a 3-day pilot study on each of the wards before the study’s start; this was to familiarise themselves with the method, ward and data-collection forms. These data were not included in the analysis.
Identification of administration errors
The following medication administration error definition was developed using the same approach used for the prescribing error definition:24
A medication administration error is the administration of a dose of medication that deviates from the prescription, as written on the patient medication chart, or from standard hospital policy and procedures. This includes errors in the preparation, and administration of intravenous medicines on the ward.
The clinical appropriateness of prescriptions was not assessed in this part of the study. Deviations from hospital procedure such as not checking patients’ identity bands or not labelling intravenous infusions were not in themselves considered as errors. Multiple errors could occur in each case of preparation and administration.
We chose a prospective undisguised observation-based method to collect data. This method has been shown to be valid.21 25 Each nurse gave written consent for observation.
The preparation and administration of regular, when required and once-only medications were included in the observation, in addition to intravenous medications. Parenteral and enteral nutrition was excluded.
An experienced observer (MG) accompanied nurses during drug administration. She recorded the preparation and administration of each drug on a standard form and intervened in a discreet and non-judgemental manner when she became aware of a potentially serious error; these incidents were included in the analysis.
Data were collected over 2 weeks on each of 10 wards at the five hospitals during 2004/2005. To be representative, the study included weekends and 8–12 h each day were selected for observation. A 3-day pilot study was conducted on each ward immediately prior to the actual data-collection period to reduce any potential behavioural changes among observed nurses. These data were excluded from analysis.
Incident reports
Incidents reports submitted to the risk-management department with each hospital were collected for each ward for the relevant study periods.
Analysis of data
Data were analysed using SPSS version 13.0 (SPSS, Chicago). Prescribing errors were classified according to type of prescribing error,23 and their incidence expressed as a percentage of medication orders screened by the ward pharmacists. Each medication order was counted only once, regardless of how many times it was seen by a pharmacist; each medication could be associated with more than one error.
Medication administration errors were classified according to type,24 and their incidence calculated. Previous medication administration error research uses the term ‘opportunity for error’ as a denominator; this is defined as ‘the sum of any doses given plus any doses prescribed but omitted.’21 26 This conventional approach has been used in numerous studies; however, in these studies, the main focus was oral medications (which do not generally involve any preparation). This is not always the case for intravenous medications; furthermore, in paediatric practice, many oral doses are also prepared extemporaneously before administration. Therefore, it was decided that there were two opportunities for error in each drug (intravenous or oral) that was prepared and administered. However, if one of the processes was missing (ie, no drug preparation required as the drug was supplied ready-for-administration) then there was only one opportunity of error. For example, if a nurse prepared 20 mg of prednisolone by dissolving four 5 mg tablets in 5 ml of water (preparation), then the drug was administered orally (administration), there were two opportunities for error. However, if a nurse withdrew 0.04 ml from 2 mg/ml of morphine elixir and administered the drug orally without any additional dilution, there was only one opportunity for error. One opportunity per error could have more than one error.
Results
Incidence and nature of prescribing errors
A total of 444 paediatric patients and 2955 medication orders were studied over 22 weeks. There were 391 prescribing errors, giving an overall prescribing error rate of 13.2% (95% CI 12.0% to 14.5%). Prescribing error rates varied between 5% (95% CI 2.2% to 7.8%) in one ward and 31.5 (95% CI 24.3 to 38.6) in another (figure 1). Incomplete prescriptions were the most common type of prescribing error, and dosing errors the third most common (table 1).

Prescribing error rates across the 11 wards in the five hospitals. A, surgical 1; B, medical 1; C, PICU 1; D, medical 2; E, NICU 1; F, PICU 2; G, general-medical ward 1; H, NICU 2; I, general-medical ward 2; J, Adolescent unit; K, general-medical ward 3. NTDGH, non-teaching district general hospital; SCH, specialist children’s hospital; TDGH, teaching district general hospital.* Error bars represent 95% CI.
Number and percentages of prescribing errors across all 11 wards studied
Incidence and nature of medication administration errors
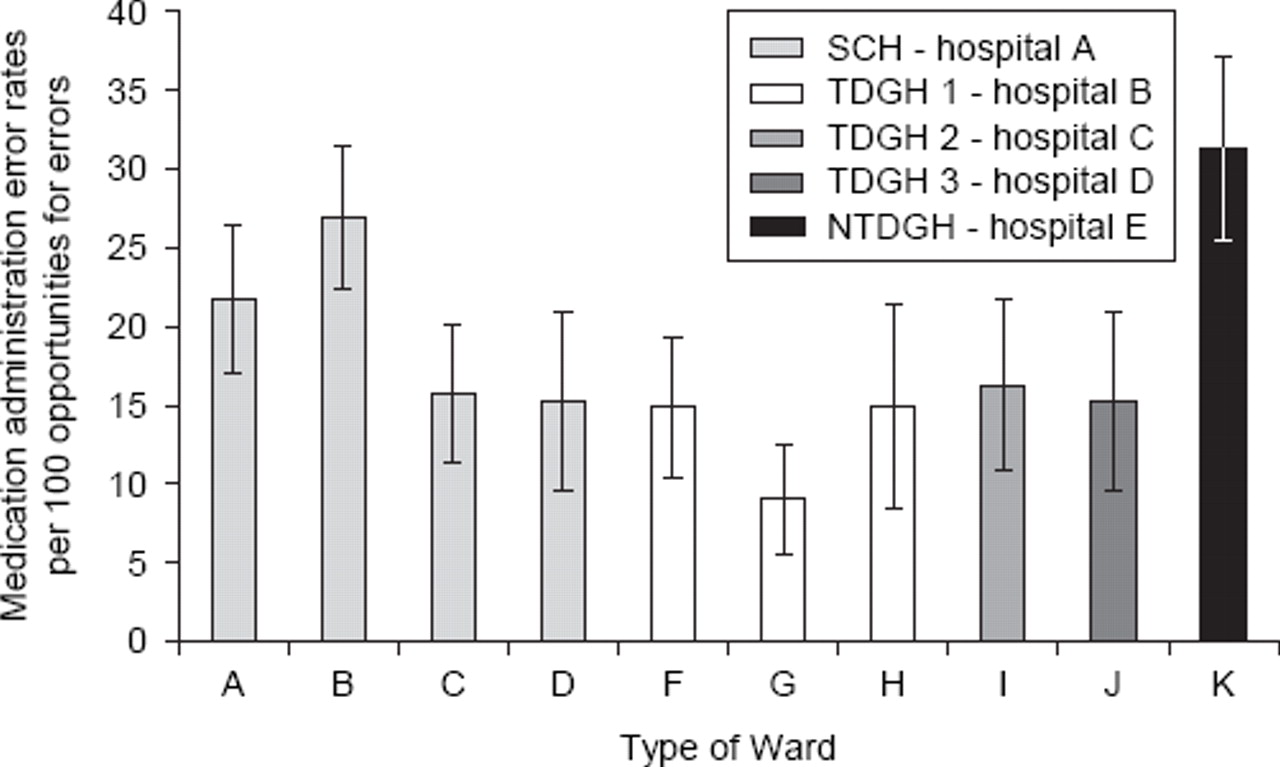
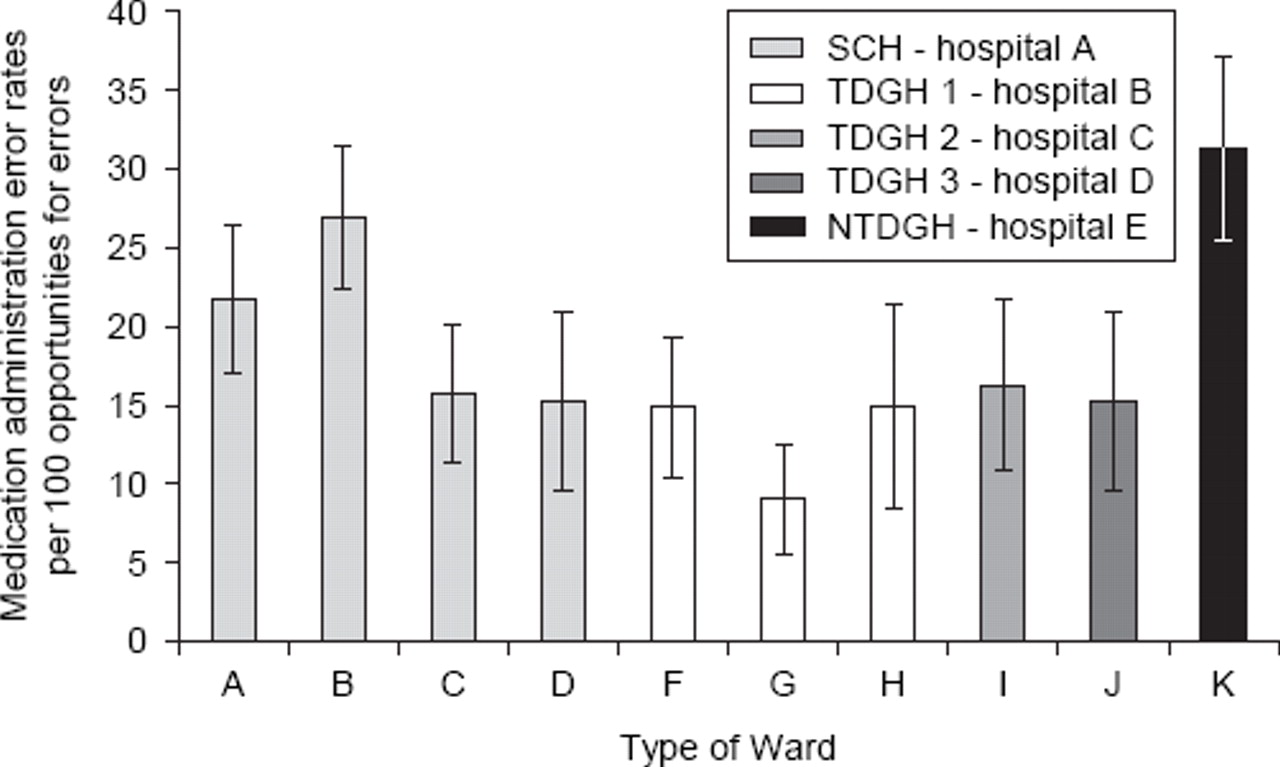
A total of 161 nurses of different grades were observed preparing and administering 1554 doses to 265 paediatric patients during 20 weeks of observation across the five UK hospitals. In total, 429 medication administration errors were identified in 2249 opportunities for error, giving an overall medication administration error rate of 19.1% of opportunities for error (95% CI 17.5% to 20.7%). Figure 2 shows the medication administration error rates across the different wards; these varied from 9.0% (95% CI 5.5% to 12.5%) on one general medical ward to 31.3% (95% CI 25.4% to 37.1%) on another.
{kind=link}
{kind=link}
Medication administration error rates and 95% CI across the 10 wards in the five hospitals. A, surgical 1; B, medical 1; C, PICU 1; D, NICU 1; F, PICU 2; G, general-medical ward 1; H, NICU 2; I, general-medical ward 2; J, Adolescent unit; K, general-medical ward 3. NTDGH, non-teaching district general hospital; SCH, specialist children’s hospital; TDGH, teaching district general hospital. *Error bars represent 95% CI.
Various types of medication administration error were identified (table 2); errors in drug preparation were the most common, accounting for 20.7% of the total. Wrong rates of intravenous administration were the second most common (19.8% of total). Dosing errors were also common (9.3% of all errors); some of these included doses which were inappropriate for administration—for example, a tenth of a suppository.
Number and percentage of various types of medication administration errors identified across all wards/hospitals
On five occasions, the researcher intervened to prevent the error reaching the patient. These were: preparing 300 mg clindamycin instead of 150 mg, administering 10 ml of sodium chloride 0.9% instead of 300 mg of benzyl penicillin in 10 ml sodium chloride, preparing diclofenac 75 mg in 40 ml sodium bicarbonate 8.4% instead of correct diluent 0.9% sodium chloride, administering 0.6 ml of diluent instead of oral drug ciprofloxacin and administering intravenous fluid (sodium chloride 0.9% plus dextrose 10% and 20 mmol potassium chloride) at 130 ml/h instead of prescribed rate 100 ml/h.
In some other cases, potentially serious errors occurred but were not identified until after administration.
Of the 391 prescribing errors identified, only one was reported to the risk-management department within the hospital. None of the 429 medication administration errors were reported, even those where the researcher intervened.
Discussion
We studied the incidence and nature of prescribing and medication administration errors across five different London hospitals. A prescribing error was identified in 13.2% of all medication orders written. The most common type of error was incomplete prescription (41.2% of all errors), and the third most common was dosing errors (11.3%). Medication administration errors occurred in 19.1% opportunities for error; errors in drug preparation and wrong rate of intravenous administration were the most common.
As far as we are aware, this is the only multicentre study in the UK that has studied both prescribing and administration errors in children. The study included different types of hospitals and wards, and the results are therefore likely to be generalisable to other UK clinical environments. Five of the 11 wards studied for prescribing errors and four of the 10 wards studied for medication administration errors were in a specialist children’s hospital.
The UK healthcare system is very different from the US system, and our research is not necessarily generalisable to other countries; nevertheless, previous studies published in the USA also show high rates of medication errors in children.9 12,–,17
Our study identified a higher prescribing error rate than that of 5.3% reported in a small-scale single-ward study in the UK.15 However, in the previous study, the prescribing error definition was not clear, and so it is impossible to compare the results directly. Furthermore, the prescribing error rate identified in our study is higher than that reported in similar work using similar error definitions in adults in the UK; in these studies the prescribing error incidence varied between 1.5% and 9.2%.27,–,30 This therefore supports the limited literature in the USA, which suggests that medication errors could be higher in children than adults.10 It may also be that our methods, which involved a separate data collector recording details of the errors identified, resulted in more comprehensive recording than in previous studies where ward pharmacists were asked to self-record the errors identified.
We also identified medication administration errors in 19.1% opportunities for error. However, in order to compare our results with previous research, we need to standardise the denominator. Using the conventional approach for calculating the incidence,21 the error rate in our study is 27.6% This is higher than a previous paediatric study on a single ward in the UK.15 The medication administration error rate we report is also higher than that reported in similar work in adults in the UK; these studies have reported medication administration error rates of 3.0–8.0% administrations for non-intravenous doses, and 49% for intravenous doses.31,–,33 The high medication administration error rate identified in our study could be because we included Intravenous medication, whereas most adult studies did not. Also, we included incorrect preparation errors such as not shaking a bottle of suspension, whereas some other studies did not.
Finally, in our study, comprehensive definitions of prescribing and medication administration errors were developed and used; this could have contributed to the high error rates.
There was great variation in the incidence of prescribing and medication administration errors between wards/hospitals, and it is not clear from the data as to why. It could be because of the differences in settings and hospitals. The variation in prescribing errors could also be related to the differential detection of errors by pharmacists or different actual error rates. Therefore, there is a need to explore the incidence and causes of errors on a local basis so that improvement strategies can be implemented.
We selected the most accurate methods to collect data; by doing this, we have minimised the risk of underestimation of medication errors. Consequently, our errors rates tend to be higher than those reported in the UK literature,17 18 but they are probably still an underestimation of the true incidence.21 22
Limitations
The study did not formally assess the clinical significance of errors; some errors such as dosing errors cited in table 1 are potentially fatal and more serious than the incomplete prescriptions.
We relied on clinical pharmacists in the identification of potential prescribing errors, and we cannot exclude the possibility of undetected medication errors, hence underestimating the incidence of medication errors. However, we also collected data from incidents reported to the hospitals and did not detect any further errors; this suggests that serious prescribing errors are unlikely to be under-reported by our method. This also highlights how few medication errors are reported to hospital incident reporting systems.21 34
The study relating to administration errors was conducted in 10 wards compared with the prescribing error part which was carried out in 11 wards across the five different hospitals. This was because of time constraints.
Furthermore, there was no test of interobserver reliability between pharmacists. However, all pharmacists were experienced in paediatrics.
Interpretation of the study
As paediatric medication errors were common in a range of hospitals and wards, it is essential for policymakers to develop strategies to minimise them. Electronic prescribing systems will be able to reduce errors of missing information and potentially reduce dosing errors.35 36 The UK government has committed to developing the electronic patient record and electronic prescribing systems; however, due to technical challenges, it is still ongoing, and paediatric electronic prescribing systems are unlikely to be available in the near future. Electronic systems can also introduce new errors. Clinicians should be vigilant in writing prescriptions; nurses and pharmacists should be vigilant in checking prescription before dispensing and administrating medications to children.14
Unanswered questions and future research
This study confirmed that medication errors in children are common; and the incidence could be higher than that in adults. However, the severity of these medication errors remains to be explored. Future research should concentrate on interventions to reduce medication errors in children.
Conclusion
Prescribing and medication administration errors are not uncommon in paediatrics, and there was great variation in the error rates across the five hospitals studied. The overall incidence of prescribing errors was 13.2% (95% CI 12.0% to 14.5%) of medication orders. This figure is higher than that reported in similar work in adults in the UK.28–29 The overall incidence of medication administration errors was 19.1% (95% CI 17.5% to 20.7%), which is higher than that reported in previous medication administration error research in paediatrics and adults in the UK.15 16 31 32
Acknowledgments
The authors would like to thank all individuals and hospitals that contributed to this research.
References
Footnotes
-
Funding MG was partly funded by the UK Overseas Research Scholarship. ICKW was funded by a UK Department of Health National Public Health Career Scientist Award at the time of the study. NB, BDF and ICKW have received funding from the UK Medical Research Council and UK Department of Health in the research of medication errors and the use of technology in their reduction. NB and IW also received funding from the First Databank Ltd and JAC in the research of the use of technology in their reduction in medication errors in children. The Centre for Medication Safety and Service Quality is affiliated with the Centre for Patient Safety and Service Quality at Imperial College Healthcare NHS Trust, which is funded by the National Institute of Health Research.
-
Competing interests None.
-
Ethics approval Ethics approval was provided by a Multicentre Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.