Article Text

Abstract
Context Follow-up strategies after emergency department (ED) discharge, alias safety netting, is often based on the gut feeling of the attending physician.
Objective To systematically identify evaluated safety-netting strategies after ED discharge and to describe determinants of paediatric ED revisits.
Data sources MEDLINE, Embase, CINAHL, Cochrane central, OvidSP, Web of Science, Google Scholar, PubMed.
Study selection Studies of any design reporting on safety netting/follow-up after ED discharge and/or determinants of ED revisits for the total paediatric population or specifically for children with fever, dyspnoea and/or gastroenteritis. Outcomes included complicated course of disease after initial ED visit (eg, revisits, hospitalisation).
Data extraction Two reviewers independently assessed studies for eligibility and study quality. As meta-analysis was not possible due to heterogeneity of studies, we performed a narrative synthesis of study results. A best-evidence synthesis was used to identify the level of evidence.
Results We summarised 58 studies, 36% (21/58) were assessed as having low risk of bias. Limited evidence was observed for different strategies of safety netting, with educational interventions being mostly studied. Young children, a relevant medical history, infectious/respiratory symptoms or seizures and progression/persistence of symptoms were strongly associated with ED revisits. Gender, emergency crowding, physicians’ characteristics and diagnostic tests and/or therapeutic interventions at the index visit were not associated with revisits.
Conclusions Within the heterogeneous available evidence, we identified a set of strong determinants of revisits that identify high-risk groups in need for safety netting in paediatric emergency care being related to age and clinical symptoms. Gaps remain on intervention studies concerning specific application of a uniform safety-netting strategy and its included time frame.
- Evidence Based Medicine
- Accident & Emergency
- Epidemiology
- General Paediatrics
- Infectious Diseases
Statistics from Altmetric.com
What is already known on this topic
The importance of safety netting after emergency department (ED) discharge to monitor disease course is well recognised and applied.
Evidence-based approaches on this topic are underexposed in literature, since strategies are often based on the gut feeling of the ED physician.
What this study adds
It remains difficult to determine high-risk patient groups for whom safety netting is essential.
Studies concerning follow-up were mostly conflicting or with limited evidence.
Young children, medical history, infectious/respiratory symptoms, seizures and progression/persistence of symptoms were the strongest associated determinants of revisits.
Introduction
When patients are discharged from the emergency department (ED) without definite diagnosis, monitoring children's course of disease to rule out serious infections is mandatory.1 This theme is covered by the term ‘safety netting’, introduced to general practice in 2004 by Roger Neighbour who considered it a core component of general practice consultation.2 Safety netting can be described as a set of procedures or guidelines, which should be followed when a patient is discharged from the ED. This strategy is required in situations with increased risk for serious complications, either in the diagnosis itself (eg, dehydration in patients with gastroenteritis) or if individual patient characteristics are associated with a high risk of complications (eg, significant comorbidity or immunosuppressive therapy).1 Patients who revisit the ED may be regarded as the high-risk population of possible failure of this safety-netting strategy.
The importance of safety netting is increasingly recognised in emergency care and literature.3 Healthcare physicians lack standardised safety-netting methods since strategies are often based on the gut feeling of the ED physician,4 and key gaps are described in need of studies on methods and effects of safety netting.3 ,5 Therefore, we planned to systematically review the literature on this important topic.
Our first aim was to systematically summarise evaluated safety-netting strategies after ED discharge. Second, we identified children at risk for revisits to improve the identification of children prone to deteriorate after emergency discharge, by studying determinants of ED revisits. Both aims were studied in the total ED population or specifically for children with common illnesses as fever, dyspnoea and gastroenteritis.
Methods
Inclusion criteria
We considered all types of studies eligible if they reported about safety netting and/or their strategy after ED discharge and extended our search for determinants of ED revisits as a proxy of failing safety-netting strategies. We included studies on the total ED population or specific for children with fever, dyspnoea and gastroenteritis. Studies reporting data on adult and children together as well as studies in low-income countries, due to differences in healthcare organisation, were excluded. Two reviewers independently assessed inclusion (EdV-K and MW); discrepancies were resolved by a third reviewer (RO).
Outcome measures
Outcomes included complicated course of disease after initial ED visit, mainly dominated by revisits and hospitalisation.
Search strategy
We searched the following electronic databases: MEDLINE OvidSP, Embase (Excerpta Medica dataBASE), CINAHL (Cumulative Index to Nursing and Allied Health Literature), Cochrane central register of controlled trials, Web of Science, Google Scholar and PubMed as publisher (searches updated in January 2014) (see online supplementary information 1). We checked the reference list of these papers for additional articles that were not included in the initial computerised search.
Data extraction
We retrieved the full text copies of all articles identified as potentially relevant by reviewing the abstracts of search results. Two reviewers’ extracted data on the following: study design, disease/working diagnosis, study population, number of revisits, follow-up period and type of revisit. The determinants were grouped into: child characteristics, social/demographics, disease characteristics, physician and process characteristics. Finally, data on follow-up after ED discharge, including the follow-up strategy, were extracted.
Risk-of-bias assessment and best-evidence synthesis
Two authors (EdV-K/DHFG) independently assessed the potential risk of bias of the studies included using the MINORS, a methodological index for non-randomised studies,6 together with the presence of revisits as primary outcome measure and the number of events (see online supplementary information 2). Consensus was reached by the two reviewers (EdV-K/DHFG); otherwise, the independent opinion of a third reviewer was decisive (RO).
We performed two separate ‘best-evidence’ syntheses based on the study of van Tulder et al;7 one according to safety-netting strategies and one according to determinants of revisits as meta-analysis of results was not possible owing to heterogeneity in participants, interventions, outcome measures and methodological quality7 (see online supplementary information 2).
Results
Identification and selection of the literature
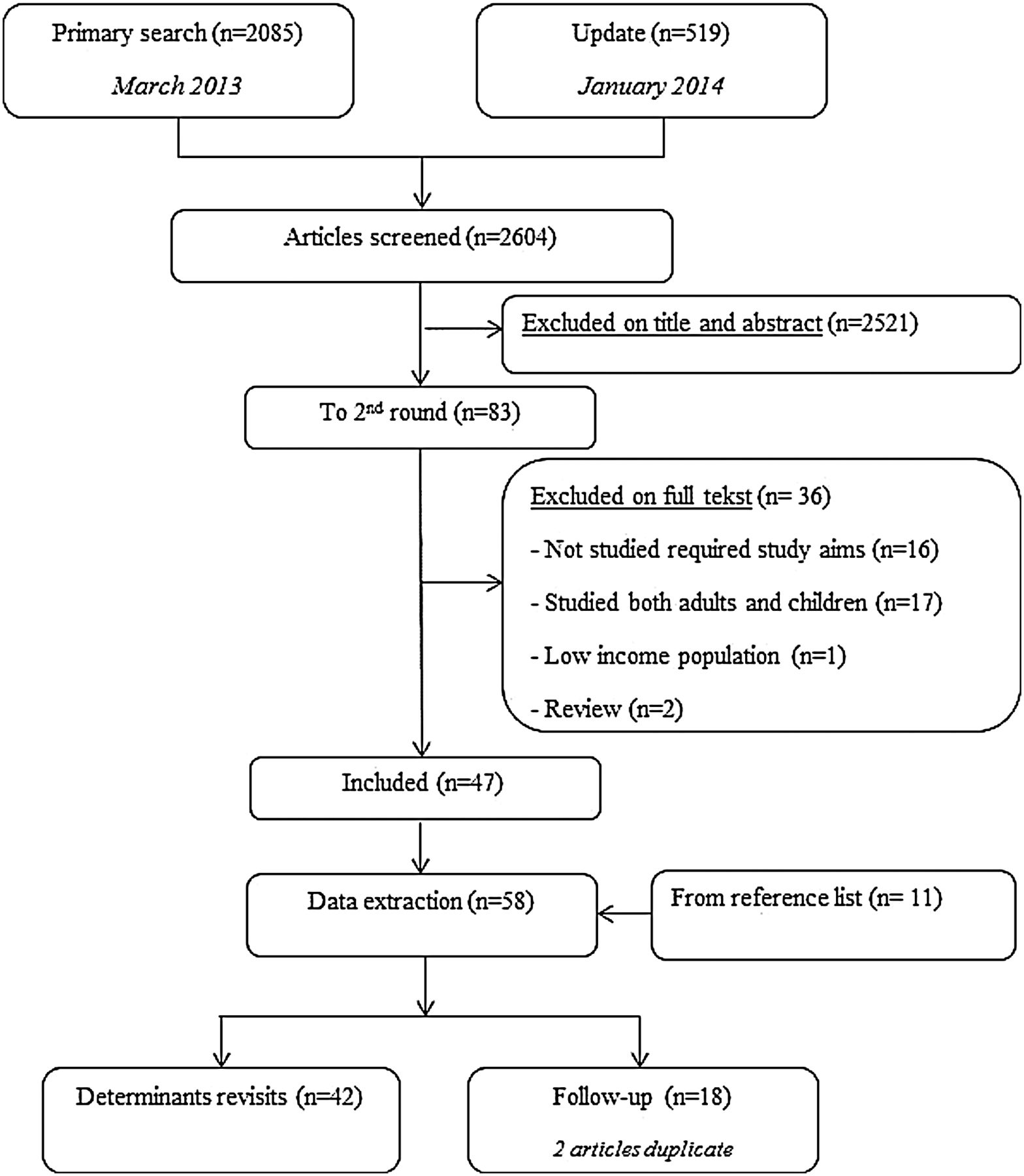
The literature search identified 2604 references (figure 1). Overall, 36 of 83 full text articles screened for eligibility were excluded on the basis of incorrect study aims, data on adult patients, reviews or low-income populations. Data extraction was performed for 58 articles, including 11 articles added from reference lists. Forty two articles described determinants of revisits, and 18 articles (2 articles duplicate) reported on follow-up after ED discharge (figure 1).

Flowchart of the study selection and exclusion stages during the systematic review process.
Description of included studies
Study characteristics are presented in tables 1 and 2. Included studies were mostly cohort studies (72%, n=42). Fifty two per cent (n=30) of the studies originated from the USA and 19% (n=11) from the UK. Year of publication varied between 1995 and 2013, with 33% (n=19) published in the last 2 years. Most studies (n=34) included all children presented to the ED or the most common paediatric illnesses; 14 studied febrile children and 10 studies reported specific diseases only (eg, gastroenteritis, influenza, respiratory tract infections). Study populations varied between 13 and 568 845 children (median: n=1371) and number of events (revisits or hospitalisation after revisit) varied between 9 and 36 734 (median: n=189). Follow-up period after ED discharge varied between 1 and 656 days (median: 3 days). Most studies (n=29, 50%) described scheduled and unscheduled revisits together; 19 (33%) only measured unscheduled revisits (tables 1 and 2).
Characteristics of included studies regarding the first study aim: safety-netting strategies after emergency department (ED) discharge
Characteristics of included studies regarding the second study aim: determinants of revisits
Risk-of-bias assessment
Online supplementary information 2 shows the potential risk of bias with 36% (n=21) of the studies having low risk of bias. For all studies, the reviewers achieved uniform bias assessment. Ten studies (17%) were scored as high risk of bias because only abstracts were available (nine Congress abstracts and one Spanish abstract). Initial disagreement on 55 out of 880 assessed items (6%) for opportunity of bias was solved by consensus reached by the two reviewers (EdV-K/DHFG) or by the decision of a third reviewer (RO).
Safety netting after discharge
Figure 2 presents an overview of the different safety-netting strategies evaluated in the included studies (n=18) and the corresponding level of evidence as identified by the colours of the plus/minus signs, according to the best-evidence synthesis (details in online supplementary information 3a and 3c).

Level of evidence safety-netting strategies according to the best-evidence synthesis.
Moderate/limited evidence
There was moderate evidence for the positive influence of a standardised follow-up programme (including, eg, a venue for handling calls after ED visits)8 on patient care and patient satisfaction.8 ,9 Limited evidence was found that clinical pathways at the ED resulted in a reduced admission rate, shortened length of stay and fewer revisits after discharge.10 We found limited evidence for risk factors associated with non-compliance of scheduled revisits; for example, parents’ perception that their child is not severely ill, parents’ age (<21 years) and ED physicians uncertainty about patients’ return.11
Conflicting evidence
We found conflicting evidence for the association between safety-netting advice and the reduction of revisits. According to four studies,9 ,12–14 revisits could be reduced by providing consistent verbal and written discharge information regarding the natural history of disease13 and temperature measurement/treatment.14 In contrast, other studies concluded that the provision of safety-net advice did not affect the number of revisits.15 ,16 We found conflicting evidence for the association between educational interventions at the ED and parental recall of discharge instructions or revisits.16–24 One study reported that video home management of fever improved caregiver's knowledge of fever, but did not decrease ED use.18 There was conflicting evidence about the role of telephone follow-up as safety-netting strategy. One study reported that this was an effective way of providing, for example, health information, managing remaining symptoms and recognising complications.25 In contrast, another study advocated caution in the implementation of telephone follow-up because of moderate success rate in reaching patients.26
Determinants of revisits
Figure 3 presents an overview of all determinants of revisits described in the included studies (n=42), their association with revisits and the corresponding level of evidence, according to the best-evidence synthesis (details in online supplementary information 3b and 3c).

{kind=link}
{kind=link}
{kind=link}
Level of evidence determinants of revisits according to the best-evidence synthesis.
Strong evidence
Child characteristics
We found strong evidence for the association of ED revisits with younger children, ranging from ≤12 months until <6 years.12 ,27–40 Moreover, for the association between medical history and revisits, although including heterogeneous definitions, we found strong evidence.12 ,28 ,35 ,37 ,41 ,42 Maquire et al12 concluded that history of illness in febrile children was one of the reasons for parental advice-seeking behaviour. However, for children with bronchiolitis, this association was conflicting.35 ,41 With strong evidence, no association was found between gender and revisits to the ED27 ,30 ,43 or revisits to the primary care provider.33 Gender was neither discriminating in the comparison of admitted children with the discharged ones after revisiting the ED nor a prognostic factor in safe discharge of children with bronchiolitis.35 ,41 ,44
Social and demographic characteristics
There was conflicting evidence that ED revisits were associated with ED crowding.27 ,29 ,42 Two studies were positively associated with revisits,39 ,45 and three other studies were even associated with lower ED crowding during late evening or night shifts.32 ,40 ,46
Disease characteristics
Strong evidence was found for the association of revisits of children with symptoms of infectious diseases9 ,29 ,31 ,33 ,35–37 ,39 ,43 ,45 ,47–50 or respiratory symptoms29 ,30 ,35 ,37 ,41 ,45 ,47–49 ,51 compared with all ED revisits. Strong evidence was found for the association between revisits and seizures or other nervous system diseases.27 ,37 ,39 Lastly, strong association was found between progression/persistence of symptoms and revisits.9 ,13 ,36 ,38 ,39 ,44 ,48 ,51–56
Limited/moderate evidence
Child characteristics
Mistry et al studied a health-related quality-of-life instrument (PedsQL). There was limited evidence for the association between lower changes in PedsQL scores and ED revisits, which implied less improved quality of life for the revisiting child.61
Process characteristics
No association was found between revisits and paediatric hospital at home service compared with conventional hospital care for children suffering from breathing difficulty, diarrhoea and vomiting, or fever.62 We found no association between revisits and children with acute gastroenteritis admitted to hospital compared with a comparable group of children managed at home.63
Conflicting evidence
Child characteristics
There was conflicting evidence for the association between ethnicity and revisits. In disease-specific studies (bronchiolitis and fever), ethnicity was not associated with revisits42 ,35 in contrast to studies including the total ED population.27 ,30 ,37
Social and demographic characteristics
There was conflicting evidence for the association between revisits and characteristics of caregivers. For example, caregiver's age, marital status and presence/age of other children were not associated with revisits in five studies.33 ,42–44 ,55 In contrast, other studies concluded that language spoken at home or single caregivers were associated with revisits.9 ,12 ,28 ,36 ,40 ,50 ,51 ,64 Next, we found conflicting evidence for the association between lower socioeconomic status and revisits.27 ,28 ,30 ,33 ,37 ,40 ,42 ,45
Discussion
Follow-up after discharge and determinants of revisits: main outcomes
Limited evidence was observed for different strategies of safety netting, with educational interventions being mostly studied. Identified determinants of children at risk for revisits included young children, relevant medical history, infectious/respiratory symptoms or seizures and progression/persistence of symptoms. No association with revisits was found for gender, emergency crowding, physicians’ characteristics and diagnostic tests and/or therapeutic interventions at the index ED. For other described determinants, no statement was possible due to conflicting evidence.
Strengths and weaknesses of this review
The development of evidence-based strategies of safety netting is a challenging new topic. Available studies describing revisits of the ED population and their characteristics vary in populations, study aims and methodology. The main strength of this systematic review is combining all information on determinants of revisits using a best-evidence synthesis. Most studies about safety netting are rather descriptive, and did not study their effectiveness.1 ,5 In our review, we summarised the literature that evaluated the clinical consequences of their safety-netting intervention.
This review has some limitations. Because of the heterogeneity of the studies, we could not perform a meta-analysis. This systematic review is limited to the provision of whether there is evidence for a significant association or not. This approach limits the interpretation and clinical relevance of the reported associations, but is a consequence of the large heterogeneity of present studies on this topic. Second, there is no standardised risk-of-bias assessment method for the variation of study designs and outcomes included in this systematic review. To overcome lack of general accepted thresholds determining the study's risk of bias, and to include relevance to the research question on the risk-of-bias criteria,65 we used the MINORS risk-of-bias criteria.6 We added two important items, which would be the most appropriate for our included studies. With this approach, we aimed to perform best available systematic risk-of-bias analysis. We classified determinants to ‘strong evidence’ on the presence of low risk-of-bias studies, although high risk-of-bias studies may also have studied the same determinants (see online supplementary information 2).
Furthermore, there are limitations embedded in the study design of the included studies itself. The majority of studies are analysed with univariable statistical approaches, with only 35% (20/58) of the studies using multivariable statistical analysis. It remains unknown to what extent the determinants are independently associated with revisits. Second, although we followed the focus of most studies by defining ‘revisits’ as proxy for high-risk populations of failed safety-netting strategies, hospitalisation after revisiting the ED is probably the most effective outcome to evaluate this topic. However, study of this outcome is limited due to its low prevalence. Third, some study characteristics increased heterogeneity between our different determinant categories. For example, determinants were not always specified, for example, ‘history of illnesses’ was not further described in the study of Maguire et al. Furthermore, outcome measures were not homogenous and included, for example, revisits or admission after revisit. Finally, study comparisons varied between revisits versus total ED population or subgroups of revisits (discharged vs admitted children).
Implications for clinical practice and future research
A content of safety-net advice, as included in the National Institute for Health and Care Excellence (NICE) guideline,66 has been published in relation to general practice where consensus was reached among general practitioners and paediatric ED consultants using a modified Delphi approach.1 ,4 Safety-netting advice should include: (1) the existence of uncertainty, (2) what exactly to look out for, (3) how exactly to seek further help, (4) what to expect about time course. Our systematic review shows that a variety of safety-netting techniques are used, but the effective components or the best way to perform remains unknown, as has been identified by others.1 ,5 Second, we generated answers on what determinants are associated with revisits, and those who are not. Moreover, the conclusions of our review can improve homogeneity in study design on follow-up strategies, and can add to progress in this research area. In essence, the importance of this knowledge should be combined with parent-related factors as their ability to understand and to comply with the designed safety-netting strategy.11 Lastly, one notable gap in safety-netting literature is its time frame strategy. The NICE fever guideline claims ‘to arrange a follow-up appointment at a certain time and place’.67 In future research, we need to study the (efficacy of) safety-netting strategies in which the aspect of time is taken into account.5 ,67
Conclusion
Determination of a high-risk group in need for safety-netting strategies in paediatric emergency care remains difficult. We identified a set of strongly associated determinants of revisits that could be used for this identification; being young children, relevant medical history, infectious/respiratory symptoms or seizures and progression/persistence of symptoms. Gaps remain on intervention studies concerning specific application of a uniform safety-netting strategy and its included time frame.
Acknowledgments
We gratefully acknowledge Wichor Bramer, medical librarian at the Erasmus University Rotterdam, for assisting us with the systematic literature search for this systematic review.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
- Data supplement 2 - Online supplement
- Data supplement 3 - Online supplement
Footnotes
Contributors EdV-K substantially contributed to the conception and design of the study. She participated in the literature search and assessed studies for eligibility. She undertook data extraction, risk-of-bias assessment and performed the best-evidence synthesis. She drafted the initial manuscript, and approved the final manuscript as submitted. DHFG substantially contributed to the conception and design of the study, and reviewed and revised the manuscript. She participated in the risk-of-bias assessment, and approved the final manuscript as submitted. MW participated in the literature search, and assessed studies for eligibility. She reviewed and revised the manuscript, and approved the final manuscript as submitted. HAM substantially contributed to the conception and design of the study. She reviewed and revised the manuscript. She participated in discussion about each step of the results, and approved the final manuscript as submitted. RO substantially contributed to the conception and design of the study. She reviewed and revised the manuscript, and approved the risk-of-bias assessment and best-evidence synthesis analyses. She participated and supervised the discussion about each step of the results, and approved the final manuscript as submitted.
Funding EdV-K is supported by ZonMW, a Dutch organisation for health research and development. The study sponsor had no role in study design; in the collection, analysis and interpretation of data; in the writing of the report or in the decision to submit the paper for publication.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.