Article Text

Abstract
Apgar scores are universally recorded, but they should no longer be used to guide resuscitation; thus, some authorities have suggested that the scores should be abandoned. However, the physiological relationships underlying the elements of the Apgar scoring system can be conceptualised as a cycle, wherein the five functions are linked by cardiorespiratory reflexes and metabolically supported by the oxygen pathway. Respiratory effort represents both the main input into the system and its functional output (sustained respirations). The progressive deterioration of functions during asphyxia, and their recovery during resuscitation, are readily understood within the sequence. This depiction helps in learning concepts such as primary and secondary apnoea and bradycardia. The visual model harmonises the pedagogical and practical values of the Apgar scoring system, by placing the rapid assessment of respirations, heart rate and colour during neonatal resuscitation (as taught in the Neonatal Resuscitation Program) in its broader physiological context. The understanding imparted by the Apgar cycle may directly enhance patient care during resuscitation, apart from the attribution of numerical scores.
Statistics from Altmetric.com
Since its conception in 1949 and publication in 1953, the Apgar scoring system has become universally adopted as a numeric assessment of the post-partum condition of newly born infants.
Dr Virginia Apgar originally developed the score to quantify the physiological status of newborn infants through simple observation; this would enable comparison of the results of obstetric practices and evaluation of the effects of maternal anaesthesia and neonatal resuscitation.1 In the next decade, she applied the score to judge which neonates needed resuscitative measures,2 while advocating the use of immediate artificial ventilation, “preferably within the first minute”, if the infant was severely depressed.3 Dr Apgar found the method to be a valuable guide in teaching resuscitation and a predictor of the probability of survival (although not for individual babies).3
Over the subsequent four decades, the association of the 5 min Apgar score with mortality and, to a lesser extent, with neurological disability was repeatedly confirmed in population studies.4–6 The Apgar score is an important variable for statistical risk adjustment and a useful adjunct to neonatal severity of illness scores.7
Nevertheless, concerns have arisen about interuser variability in Apgar scoring8–10 and over clinical and legal misuse of the scores.11–13 Clinical usefulness of the scoring has also been questioned. In the delivery room, newborns who appear significantly depressed should be immediately resuscitated; indeed, the Neonatal Resuscitation Program states that “…the Apgar score is not used to determine the need for resuscitation, what resuscitation steps are necessary, or when to use them”.14 Rather, the Program espouses rapid cycles (∼30 s each) wherein respirations, heart rate and colour are evaluated, followed by a decision on intervention and the corresponding actions.14 This approach simplifies and expedites implementation of the fundamental resuscitation steps.
What is already known on this topic
Apgar scores are routinely recorded, although they should not be used to guide neonatal resuscitations.
The Apgar scoring system is usually taught in a tabular format.
What this study adds
The five signs in the Apgar system can be conceptualised as a cycle, highlighting the physiological interdependencies of these functions.
Understanding the physiological foundations of the Apgar system has pedagogic value, and it may improve clinical decision-making during neonatal resuscitation.
A more serious concern about attributing Apgar scores while resuscitating arises from the need for the resuscitator to pause for about 15 s to assess and sum the scores, thereby diverting attention from the flow and teamwork of modern resuscitation. Medical students witnessing their first neonatal resuscitations are surprised to observe that Apgar scores are usually attributed in retrospect, after the baby has been stabilised and the clinician has completed the hands-on tasks (ie, thermoregulation, ventilation, intubation, surfactant administration, application of identification bands, and ocular and vitamin K prophylaxis). O’Donnell et al10 have also speculated, on the basis of video recording of resuscitations, that Apgar scores are often assigned retrospectively. This practice may be appropriate, as at present the assignment of Apgar scores has no obvious direct benefit to either the clinician or the individual baby. There is no evidence from randomised trials suggesting improvement in outcomes by the attribution of Apgar scores during resuscitation or demonstrating the safety of the practice. Furthermore, it is difficult to justify the routine need for an additional team member whose primary functions would be observing the resuscitation, documentation and attribution of Apgar scores in real time.
Some have suggested that the use of the Apgar score as a clinical tool should be abandoned,15–17 although it remains a useful numeric index for documenting the newborn’s general condition and response to resuscitation.18 It has recently been proposed that Apgar scores should be recorded in conjunction with resuscitative interventions, using an expanded documentation form.13
Regardless of its direct effect on individual babies, the Apgar scoring system has drawn the attention of clinicians and researchers to newborn resuscitation, thereby improving our understanding of neonatal transition, and probably contributing substantially to the secular improvement in neonatal survival within defined populations. This value and the epidemiological usefulness of Apgar scores justify their continued use—even if attributed retrospectively or by an independent observer, as is current practice.
With this premise, I believe that the pedagogical and clinical value of the Apgar scoring system could be enhanced. Apgar scores are commonly presented to students as a table, most useful for facilitating documentation of scores at delivery, or as the APGAR acronym (a mnemonic for appearance, pulse, grimace, activity, respiratory effort).19 Neither of these formats conveys the physiological foundations of the scoring system.
Dr Apgar derived the constellation of five clinical signs empirically, not from statistical analyses of patient data. In response to a question from a medical student during breakfast in the hospital cafeteria,20 she drew on her practice experience in obstetric anaesthesiology, and adapted clinical monitoring signs that were usable in neonates; she then proceeded to evaluate the system in newborns at delivery. Experimental evidence on the progressive deterioration and recovery of physiological measures during asphyxia and resuscitation at birth was obtained primarily by Dawes,21whose classic work in rhesus monkeys and other animal models is the basis for most of our inferences about the pathophysiology of asphyxia in human newborns. By placing Apgar’s five signs in the experimental context of Dawes’ asphyxiated monkeys and related work,21–23 a conceptual model emerges wherein the five clinical signs may be interpreted, simplistically, as physiological steps in the oxygen transport pathway.
The construct shown in fig 1 is intended to emphasise the sequential physiological relationships among the elements in the Apgar scoring system. The initial postnatal step entails respiratory effort, which inflates the lungs, thereby effecting gas exchange and directly derepressing heart rate23; subsequent delivery of oxygen to the heart supports cardiac metabolism and sustains heart rate. As oxygenated blood is pumped to the periphery, skin colour becomes pink. Functionally, peripheral oxygen delivery supports neuromuscular metabolism, which manifests as age-appropriate muscle tone and responsiveness to external stimuli (eg, reflex irritability).21 As normal neural and muscular function sustain respiratory effort, this vital cycle is perpetuated. Thus depicted, respiratory effort represents both the mechanical input to the Apgar cycle and its functional outcome, as a sustained respiratory drive reflects adequate performance of the entire system.

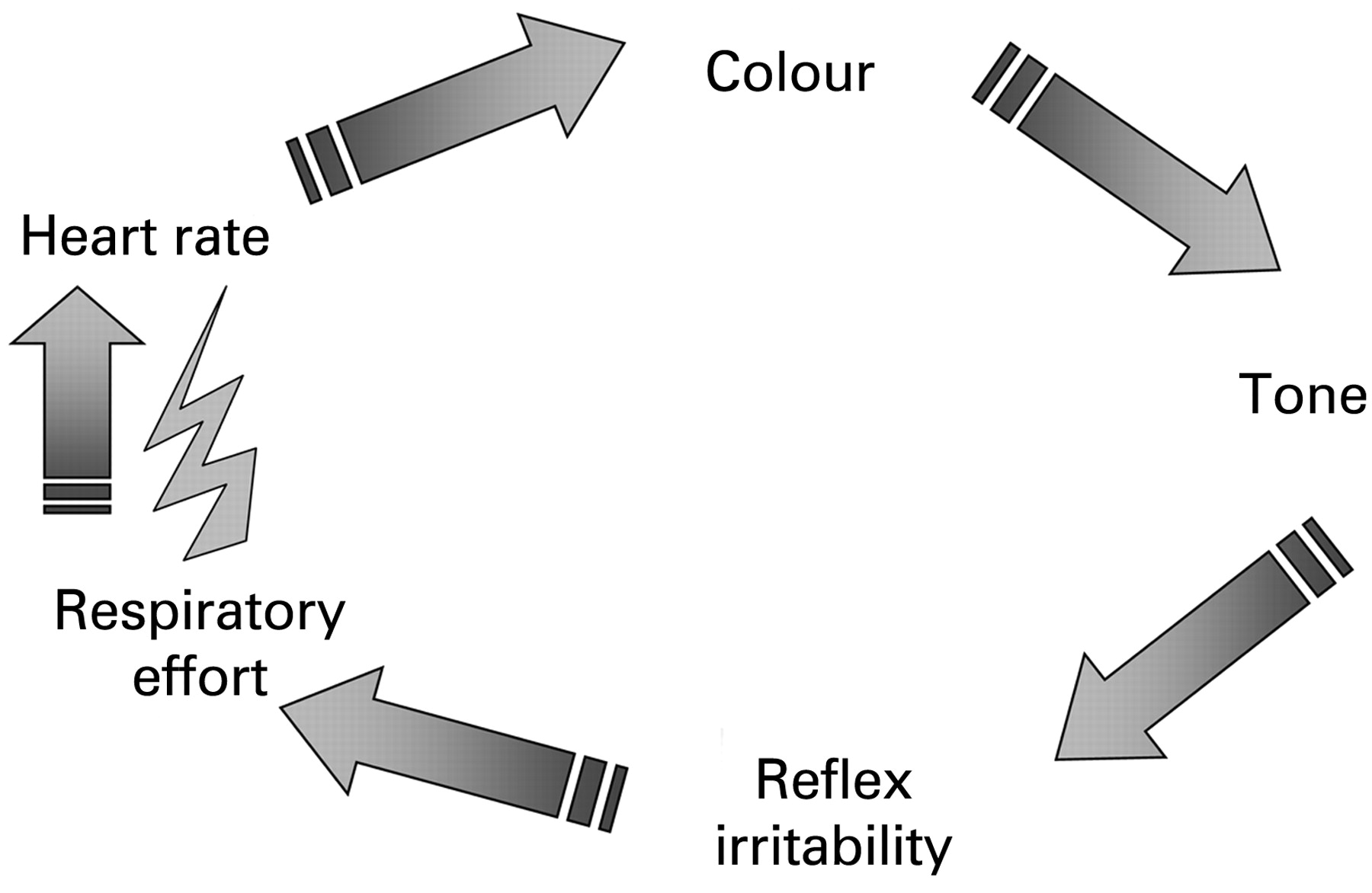{kind=link}
Numerous factors, including maternal medication, hypoxia–ischaemia and intrinsic fetal neuromuscular abnormalities, can affect the elements of the Apgar cycle. Most conditions that depress fetal cardiorespiratory or neurological function, during or immediately after birth, cause primary apnoea and hypoventilation in the newly born. With failure of lung inflation, aeration and oxygenation, a predictable sequence of events ensues. Increased vagal tone immediately induces “primary” (reflex) bradycardia,21–23 a mechanism denoted by the lightning bolt. Hypoxia then progresses, promoting gradual loss of neuromuscular function. The hypoxic spiral will eventually cause metabolic dysfunction at the muscular and central neurological levels, culminating in secondary apnoea, with concurrent lack of responsiveness to stimuli.2 Only after severe, prolonged hypoxia does asystole develop.2 21
Resuscitation with positive pressure ventilation before the onset of asystole results in a sequence of re-acquisition of functions that is “qualitatively similar in all species”.21 Heart rate increases rapidly because of the vagolytic effect of lung inflation,22 23 peripheral oxygenation returns, and there is gradual recovery of neuromuscular function, including sustained breathing. The time course of recovery of neuromuscular functions is less well characterised and somewhat variable, depending on the severity of asphyxia (particularly the duration of secondary apnoea before resuscitation), but also on species21 and, probably, on the specific neuromuscular reflex studied21 and the method of observation.
Using the proposed diagram, students easily learn to differentiate primary (reflex) apnoea and bradycardia from secondary (metabolic) effects of sustained hypoxia. Over the past 18 years, medical students and residents have appreciated the insight imparted by this visual display of the Apgar scoring system. They understand the usefulness of tone and reflex irritability, even as they are taught rapid-cycle assessment of respirations, heart rate and colour, in the Neonatal Resuscitation Program.14 In this framework, conditions of the newly born not related to hypoxia are also readily understood by students and practitioners, which may facilitate their appropriate management. Consider, for example, a vigorous, pink, crying, well-appearing infant, who is noted to have a heart rate of 60 beats/min during routine auscultation at 1 min after an elective caesarean section. The heart rate remains between 50 and 60 beats/min, despite appropriate basic support and even if assisted ventilation is provided. Simply following guidelines, clinicians would be tempted to inappropriately escalate the resuscitation. With contextual understanding, students readily realise that there is an anomaly of the heart rate in particular that does not fit the physiology underlying the Apgar cycle. Some even arrive at a diagnosis of congenital heart block, and suggest appropriate management, which would not involve cardiorespiratory resuscitation. Exceptional conditions affecting the other individual signs can likewise be easily interpreted.
This visual representation of the Apgar scoring system emphasises physiological interdependencies between the clinical signs, and it may facilitate learning the biological and therapeutic processes involved in neonatal resuscitation. The gradual progression and recovery of abnormalities implicit in the model is more flexible than the assumption of a rigid order of disappearance and reappearance of each Apgar sign, which varies among authors,24 25 and which depends partly on the technique by which a given sign (whether colour or reflex irritability) is assessed in practice. The cycle format de-emphasises numerical scoring during the actual resuscitation, which is congruent with Dr Apgar’s intention that the evaluation should be performed “…without interfering with the care of the infant…”.1 More importantly, enhanced understanding of the physiology of resuscitation could expedite accurate decision-making during the procedure, with potential immediate benefits to each affected infant. In this manner, the Apgar system directly adds value to each neonatal resuscitation.
Acknowledgments
I thank the many medical students, residents and clinicians whose comments have encouraged the continued use and evolution of this visual aid, over the past 18 years.
REFERENCES
Footnotes
Competing interests: None.