Article Text

Abstract
Improvements in patient safety result primarily from organisational and individual learning. This paper discusses the learning that can take place within organisations and the cultural change necessary to encourage it. It focuses on teams and team leaders as potentially powerful forces for bringing about the management of patient safety and better quality of care.
- patient safety
- teamwork
- learning
Statistics from Altmetric.com
Key messages
-
One route for improving safety is to ensure individuals, organisations, and the teams within them learn from the errors they make, but cultures must exist to make this process safe and therefore successful.
-
Organisational and, in particular, team cultures are the most appropriate and efficient places for this learning to take place.
-
Various routes for enhancing team cultures in terms of safety are discussed and ways to evaluate teams are considered.
Organisations are a dynamic balance between the authority and autonomy of the individual, the control that exists in formal structures, and the cooperation that takes place within and between teams.1 In order to improve patient safety, organisational cultures are needed which enable learning to take place at every level, particularly learning which arises from occasions where errors occur or care could be improved.
Individual learning
Risky behaviours are easiest to perceive at the sharp end of care—where the health professional and patient interact. This is the most readily apparent place for allocating responsibility, and many internal reviews of untoward incidents focus on this end—seeing problems in terms of the lack of skills of health workers and poor communication with others, or their affective state such as depression which may impair their decision making.2 This focus is not surprising: patient safety and its failures are most easily visualised and analysed at this level; moreover, it creates the smallest possible sense of ownership for the rest of the organisation. Responsibility for such a task as ensuring the safety of so many people in such potentially dangerous situations is bound to create anxiety at a level that most of us would strive to defend against, so it is not a surprise that this responsibility is frequently located in the smallest possible organisational unit—the staff member at the sharp end of the transaction. The shift in recent years towards making safety the legal responsibility of the chief executive is therefore essential if things are to change.
Learning by the individual health worker seen as responsible may be very long lasting; certainly, early mistakes are a powerful part of memories for doctors.3 4 However, the learning involved may not always be appropriate as their clinical care may become inappropriately defensive in the future. Janoff-Bulman5 has described the process of change that takes place in individuals faced with crises: first the confrontation with an experience which does not fit their previous assumptions about themselves; next resistance by means of ignoring or reinterpreting the incident; followed by validation where the truth is recognised; and finally integration which allows the previous and new knowledge about themselves to be synthesised and new learning and behaviours to take place. These steps, if completed, represent a healthy progression and could equally apply to organisations faced with serious safety problems. Even if the individual responsible for a serious mistake goes through these processes successfully, the learning for the rest of the organisation is likely to be negligible unless it can move forward in similar ways.
Behavioural change after negative events has been shown to be quite narrowly focused on the person or persons most closely involved and on the behaviours most obviously connected with the event.6 If we do not personally experience a negative event for ourselves, our sense of control over our future events is almost magical. Based on their lives thus far, many of those who live under the volcano tragically underestimate the chance that it might erupt! This optimism may be particularly problematic where confidence is already high—for example, in the case of medicine, students and doctors are often chosen for their high confidence.
Both individual and organisational learning about safety will also be influenced by the training and education that precedes taking formal responsibility. All healthcare staff may need encouragement to see that error and learning are intimately connected, and given ways to help themselves and others learn from their mistakes. Achieving this balance needs to continue throughout training for all healthcare workers—for example, by encouraging the reporting of errors while doing whatever possible to remove the shame and fear that so often follow them.7
Organisational learning and cultural change
There are numerous examples within management literature of why organisational learning so often fails to occur.8–10 These include bureaucracy, a lack of clear purpose or feedback mechanisms, poor communication, and cultural issues around a lack of openness, centralised authority, and blame where errors are seen as indicating incompetence.11 On the other hand, there is a useful body of literature building up around what are termed “high reliability organisations” (HROs) which are nearly error free despite operating in highly hazardous fields.12 13 In particular, these include the ability to react to unexpected sequences of events through constant training, and “redundancy” where there is more staff and equipment than appear to be needed—a rare event in health care.
EMOTIONAL AND SOCIAL CONTEXTS OF HEALTH CARE
In tackling clinical risk by changing culture we need to take note of the literature from other sectors,10 but also to appreciate the special emotional and social context in which this change will take place; this is an arena in which mistakes can actually cause physical harm to those we intend to help. As Leape et al14 have said: “ . . . patients and physicians . . . live and interact in a culture characterized by anger, blame, guilt, fear, frustration, and distrust regarding health care errors. The public has responded by escalating the punishment for error. Clinicians and some health care organizations generally have responded by suppression, stonewalling, and cover-up.”
This emotional context needs to be worked with rather than ignored or denied. Apart from existing in its own right, it is a contributing factor to the high stress levels that health workers experience.15 16Stress and error are intimately linked; for example, Houston and Allt17 found that insomnia and stress increased alongside errors as junior doctors began a new post. Since resistance to change is greater when people are demoralised or under unreasonable pressure, a failure to acknowledge the very real emotional context of health care and high stress levels is likely to make any attempts at real cultural change impossible.
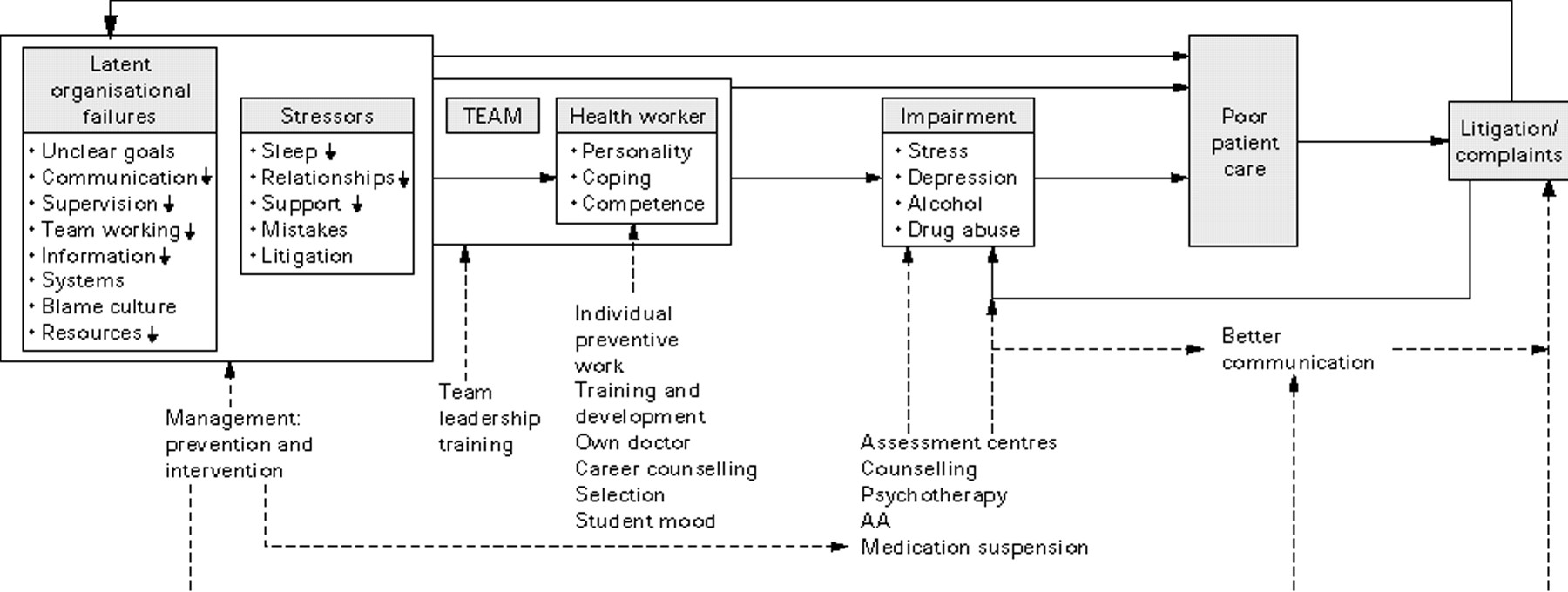
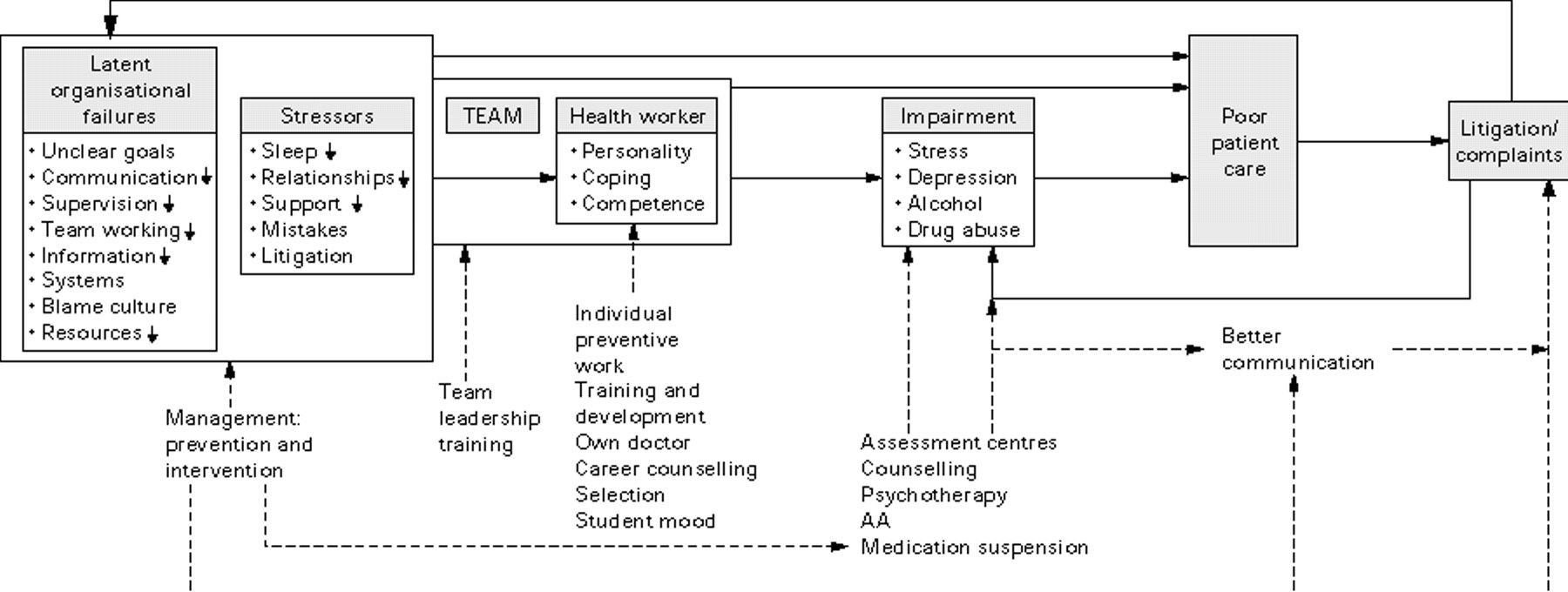
The relationship between stress and error is made more serious because findings consistently show that health professionals—particularly doctors, nurses, and managers—are considerably more stressed than other British workers. Wall et al15 found that 28% of health staff overall were above the threshold on the General Health Questionnaire compared with 18% of workers in the British Household Panel Survey of 1993. Nevertheless, there was wide variation between trusts (17–33%), indicating that work factors, including management practices, are influential in causing or lowering the stress of staff. Bringing together these findings suggests strongly that one way that management can improve patient safety is by lowering the stress levels of staff. A supportive organisational culture which benefits both quality and staff wellbeing is illustrated by the research into “magnet” hospitals19 and from results of the largest patient satisfaction survey ever conducted which showed the highest correlations were with the cheerfulness, friendliness, and sensitivity of staff.20 The way that the health of organisations and their individual staff can affect patient safety is set out in fig 1,21 which also shows that, so long as management commitment is assured, a number of means exist to enable organisations to reduce staff stress and so improve care.21–27
{kind=link}
A systems approach to the causes of poor patient care. Reproduced with permission of the publishers from Firth-Cozens.21
In terms of the social context, humans in all situations make alliances which can be both productive and disruptive.28 Wherever possible we tend to forgive those within our alliance for making the mistakes—we don't want to cause them the emotional pain that is associated with blame and criticism,23 29perhaps deciding that all will be remedied by some extra training.30 So some staff may have their mistakes or their behaviour ignored over time or reinterpreted or forgiven, so long as they are within the alliance; or be scapegoated if they are outside it,31 as can happen to a junior doctor or a nurse who is cast out through blame, or to patients or other staff groups who were outsiders from the beginning. Whistle blowers will also be cast out32 since disloyalty to the alliance is seen as a very serious crime, reflecting our national culture that forbids the “telling of tales”. By defending colleagues within the alliance and casting aside those outside it, learning throughout the alliance or the organisation as a whole becomes much more difficult. This makes the structural tying in of clinical teams to management particularly important.
ORGANISATIONAL CULTURE AS A TARGET FOR CHANGE
There is no doubt from what has been said above that organisational culture and the practices that underpin it are essential targets for change towards greater patient safety—in particular, the necessary cultural change towards openness and accountability. This will be a culture where reporting of mistakes, including near misses, is routine, and where this and demonstrations of learning from mistakes are the behaviours which are most clearly valued and rewarded—a culture which has made air transport safer.33 It will provide real rather than ambivalent support to whistle blowers and to patients who report that all is not well.34 Competition between groups is natural and in such an organisation this competition will be used to drive the goal of patient safety, rather than merely those of efficiency or technological advances. Making safety “sexy” rather than dull is essential, and for this reason risk management within the organisation should be given particularly charismatic leadership to help break the mould of its being a split off, tedious, and reactive concept.35
A systems approach to risk36 is essential in terms of cultural change in that it has the effect of spreading responsibility throughout all levels of the organisation. So long as the acceptance of responsibility at managerial levels is seen to be taken seriously, this will help to negate an authoritarian “top down” culture. Just as importantly, this sharing of responsibility will reduce the level of emotional response that takes place at the sharp end, which should allow learning to occur more readily and more appropriately.
However, an organisation-wide approach cannot solve everything. Various writers have described how the most successful organisations are small to middle size family businesses of not more than 150 members,28 very different from most British health trusts. Moreover, stress levels are higher in larger hospitals.15 It may be that the particular size and complexity of healthcare establishments means that they do not lend themselves so well to attempts to intervene directly at the organisational level, other than by creating the appropriate culture and structures to enable smaller groups such as directorates and, particularly, teams to bring about safer care themselves.
Using teams to tackle patient safety
The benefits of teams in reducing errors and improving the quality of patient care have been recognised in a number of studies.37–39 For example, Reith,37 looking at lessons from mental health inquiries, found four major themes that recurred throughout: (1) thoroughness and attention to detail; (2) “real” teamwork including inter-agency cooperation and effective liaison; (3) listening to all members of the clinical team; and (4) listening to carers, relatives, and patients. Similarly, Adorian et al39 demonstrated that regular team discussions and feedback significantly improved detection, treatment, and follow up of patients with hypertension. Teams clearly play a major role in creating safer patient care.
Outside health care the importance of the team was apparent in a study of flight crews which considered the effects of fatigue on errors.40 Crews in the fatigue condition who had flown together for several days were found to make significantly fewer errors, looking at overall team scores, than crews who were rested but who had not worked together long. It was not that those within the fatigued team made fewer errors—individually they made more, just as expected—but the team was able to compensate for them. This lower rate of errors will be partly due to team attributes such as being able to recognise and acknowledge failures, coordinate and compensate better, or through the influence of good teams in lowering stress levels.41 Fatigue does not necessarily lead to stress,42 and it may be that the increased support which teams are able to give, the greater awareness of each other's ways of working that they allow, and the greater chance of coordination act together to reduce stress levels.
Teams also matter because there is evidence that good teamwork appears to be associated with lower stress levels. Those in “real” teams—ones with clearly defined roles whose members work together to achieve them, with different roles for different members, and recognised externally as a functional team—have lower stress levels than those in teams which do not meet these criteria, while these in turn have lower scores than those in no team at all.41 We are social beings but also ones who want individual recognition. Good supportive teams allow our ideas and participation to gain the essential acceptance and valuing which make up that recognition, from our peers and beyond, and so become an essential part of reducing stress and containing the emotional context of health care.
WHAT MAKES A GOOD TEAM AND HOW CAN IT BE MEASURED?
There have been various evaluations of the elements that lead to team effectiveness.38 41 43–46 One of the most important in terms of patient safety is that the teams should ensure that they are able to hear the voices of those staff with the most experience of what can go or has gone wrong in patient care, whether or not they are of lower rank than their colleagues. Morgan's work on naval teams47 is useful in this context. He found that in effective teams:
-
members monitored each other's performance and stepped in to help out—trust was an implicit part of this;
-
giving and receiving feedback was the norm for all team members and seen as part of their role—understanding each other's role is an important part of this and one that does not happen frequently in health services48 49;
-
communication was made real—senders checked that messages were received as intended. However, there is a fundamental problem in assessing the effectiveness of teams and, indeed, of organisations in terms of safety and its failures—namely that, at least in the early days of monitoring, a team with a culture of openness and reporting is likely to produce more accidents and near misses than one in which errors are linked to incompetence and hidden where possible, such as in those with authoritarian team leaders.50 Measuring effectiveness is therefore not always easy unless you concentrate on the large scale incidents which are difficult to miss or where you have in place precision monitoring systems such as in aircraft.40 One way around this would be to measure as outcomes attitudes about risk and safety, and evidence of change being accomplished. Another useful route would be to develop systems to capture near misses. This is a relatively rare source of information in the health services, though air travel has used it as a principal route to increasing safety. Near misses have the advantage of carrying less emotional debris and so defences against seeing and addressing them are likely to be lower. Nevertheless, they will never be as salient to staff as real errors, so the importance of reporting them will need to be constantly reiterated. Hackman51 considers three essential ways to capture team performance: (1) elements of the task itself, which would include accidents and near misses as well as other indices of care; (2) measures of the team members' ability to work together; and (3) measures of team members' wellbeing and development.
ENHANCING TEAM EFFECTIVENESS
There are a number of ways to improve the effectiveness of teams—for example, regular meeting, good communication, valuing of diversity, real participation, adaptability, etc.38 The broader concepts which underlie these are discussed below.
Improving decision making
Although many of the routine procedures come from previous training, guidelines and protocols, there will be other areas within the work which should be tackled through the establishment of habit, and the team is an appropriate organisational unit to decide what these are and how they should be tackled using evidence or guidelines where they exist. Equally, it can periodically horizon gaze in order to anticipate potential changes and new risks and to share these with the wider organisation.52 The importance of diversity in teams has been stated frequently.38 52 53 A multidisciplinary approach to decision making creates a broader knowledge and so increases the ability of the team to address its tasks well, so long as all the members feel able to participate fully.22 54 55 Moreover, multidisciplinary teams are likely to provide a wider range of support to less experienced staff and so reduce stress levels.
In order to enhance patient safety, decision making at both the team and the individual levels can habitually include questions such as those suggested by Snowden56 with reference to psychiatric care:
-
Do we know what the risks are and do we have all the necessary information?
-
Are we cutting corners and setting aside enough time for all involved to come to a decision?
-
Do we need to take this risk now?
-
What is it hoped will be achieved and what might happen?
-
Are there discrepancies between the decision and the observation of others?
-
Do we have a rigorous formulation of the case?
Listening to patients
To aid decision making further, clinical teams need to include all those people who can usefully provide information about the patient; but could patients themselves ever be seen as team members? This need not involve the same type of membership that health staff have, but it would be a means of listening to their views and their concerns in ways that do not always take place now. Certainly, their presence has been found useful within audit groups.57
In reality, patients are very much outside any of the alliances within health care; in fact, they have been written about as “the enemy”.58 Menzies-Lyth59 suggests that we keep them outside because we cannot bear to identify with their suffering, disease, humiliation, and so on; worse still, in terms of error, that we may play any part in it. This is one of the reasons patients and carers are not listened to properly; another is that they sometimes bear bad news; and a third is that health staff genuinely have less and less time to listen as fewer of them are expected to do so much more.60 61
Most mental health enquiries show that staff have not heard or sought the views of carers or other relatives who may have much greater knowledge of patients than they do.37 Perhaps thinking of them as team members would put an impossible strain on individual health care staff; however, providing the means whereby the team itself can listen to, share, and act upon information from patients or carers is essential.
Rewarding teams
Good teamwork is still not common in health care62 but its importance makes it imperative that we consider how its performance is managed and how good team working is rewarded, not just through one individual member but for the team as a whole.63
Encouraging innovative solutions
Within health care individual solutions will depend upon local problems and local circumstances. Multidisciplinary teams are often the units best able to identify and tackle such problems—for example, to create work patterns that minimise sleep deprivation by looking at the whole context of patient care.64 This may involve getting many of the tasks in patient care at night done by staff other than the doctors who have worked through the day, or organising rotas and on-call commitments in the context of the daily activity of the team while outpatient clinics and routine surgery can be scheduled to ensure they do not coincide with a team's responsibilities for emergency care.64 65 Finally, work patterns need to respond to the experience (or inexperience) of team members—for example, consultants may need to adjust clinic lists in order to support the new preregistration house officers when they begin their first postgraduate job.64
Autonomy and accountability
Teams within health care correspond well with descriptions of “self-managed teams” regarded in the management literature as reflecting a good organisational structure. Such teams are autonomous in taking operational decisions, are responsible for achieving their performance goals, and are usually multidisciplinary to allow cross-fertilisation of ideas among members.66 Despite the benefits perceived in such teams, it is essential that they are tied into the management structure and goals of the organisation. As stated earlier, the strength of an alliance can be a barrier to quality as well as benefit.
In terms of the accountability of such teams, Brittain and Langill67 have described how one health organisation tackled the vagueness of working relationships between clinical teams and senior management, and the lack of clarity around their accountability and authority. Just the process of doing this is likely to be as crucial as the type of framework finally agreed upon.
Leadership
Finally, none of this will happen without good team leadership and, if we want this, then we must hold people accountable to bring it about and ensure that the relevant resources to allow its development are provided.
TEAM WORKING AND TEAM LEADERSHIP
Good teams do not just develop on their own; where the team experience is poor, individual competitiveness is a very real alternative.46 Good team leadership is essential. Nevertheless, for clinical staff, team leadership training is lacking.68 Without such development, teams may experience various phenomena that are peculiar to groups. For example, working in uncertain situations can be subject to the psychological phenomenon of groupthink69 where members tend to reinforce each other's assumptions rather than test them out or go outside for help. In addition, teams that are not functioning well can be destructive of individuals,31 just as a good team can support and develop those within it. Organisational studies over the last half century have shown that 60–75% of employees in any type of organisation find the most stressful aspect of their job is their immediate boss.70 71 Much of the credit for a well functioning team or responsibility for one that distresses its members goes to its leadership.72
We humans are hierarchical creatures28 and the structures we create inevitably and by necessity reflect this, so leadership cannot be avoided. Teams need leaders to pull them together, to provide them with a common purpose, and to develop their skills, expectations, and patterns of learning. Leadership skills involve getting things done through others, being adaptable but persistent, breaking down barriers, and inspiring and helping their members to succeed. Leadership is not domination but persuasion, and a large number of studies have shown that certain leadership characteristics are related to enhanced team performance on the one hand, or to teamwork that negatively affects safety on the other—for example, those who are over-competitive, dictatorial, or paranoiac.70–73 Nevertheless, there is evidence that even those whose traits are less conducive to producing the best teams can be changed through interventions74 including developing ways to allow juniors to question decisions made by more senior staff,75 a strategy which has greatly enhanced the safety of air travel.76
Conclusions
Although individual and organisational learning must take place for health care to increase patient safety, the outline above indicates that it is likely to do this best within the context of a well functioning team. Nevertheless, such teams need to be tied into the management structure in ways which allow their accountability to be clearly recognised by everyone. Good teams will be those which are open to learning from their mistakes as well as their successes, but this is unlikely to take place unless the culture of both the team and the organisation can shift towards welcoming such openness and monitoring the changes that result. Good team leaders will be essential to this process, which means that their development across the organisation will be a vital but not inexpensive step in managing risk. Extra resources are essential to do this, but also are needed to provide “redundant” or back-up equipment and personnel to avoid crises, as well as to ensure that sufficient staff are available so that patients and carers can be properly heard.
References
Footnotes
-
↵* Adaptation of a chapter in Vincent C, ed. Clinical Risk Management. London: BMJ Books, 2000.