Article Text

Abstract
Introduction: Effective feedback from incident reporting systems in healthcare is essential if organisations are to learn from failures in the delivery of care. Despite the wide-scale development and implementation of incident reporting in healthcare, studies in the UK suggest that information concerning system vulnerabilities could be better applied to improve operational safety within organisations. In this article, the findings and implications of research to identify forms of effective feedback from incident reporting are discussed, to promote best practices in this area.
Methods: The research comprised a mixed methods review to investigate mechanisms of effective feedback for healthcare, drawing upon experience within established reporting programmes in high-risk industry and transport domains. Systematic searches of published literature were undertaken, and 23 case studies describing incident reporting programmes with feedback were identified for analysis from the international healthcare literature. Semistructured interviews were undertaken with 19 subject matter experts across a range of domains, including: civil aviation, maritime, energy, rail, offshore production and healthcare.
Results: In analysis, qualitative information from several sources was synthesised into practical requirements for developing effective feedback in healthcare. Both action and information feedback mechanisms were identified, serving safety awareness, improvement and motivational functions. The provision of actionable feedback that visibly improved systems was highlighted as important in promoting future reporting. Fifteen requirements for the design of effective feedback systems were identified, concerning: the role of leadership, the credibility and content of information, effective dissemination channels, the capacity for rapid action and the need for feedback at all levels of the organisation, among others. Above all, the safety-feedback cycle must be closed by ensuring that reporting, analysis and investigation result in timely corrective actions that effectively address vulnerabilities in existing work systems.
Conclusions: Limited research evidence exists concerning the issue of effective forms of safety feedback within healthcare. Much valuable operational knowledge resides in safety management communities within high-risk industries. Multiple means of feeding back recommended actions and safety information may be usefully employed to promote safety awareness, improve clinical processes and promote future reporting. Further work is needed to establish best practices for feedback systems in healthcare that effectively close the safety loop.
Statistics from Altmetric.com
Developing effective feedback from safety information systems is essential if healthcare organisations are to improve reliability and safety in care delivery processes. Several influential reports on patient safety have highlighted the importance of the development of effective systems for learning from failure to reduce the occurrence of preventable patient safety incidents.1–3 In international healthcare, implementation of incident reporting systems within organisations has been promoted as a means of addressing safety in service delivery, and to this end the WHO has begun work to develop guidelines for implementation of effective reporting systems.4 In England and Wales, reporting systems have been developed as part of individual trust risk-management systems, and a National Reporting and Learning System (NRLS) has been set up to analyse aggregated data by the National Patient Safety Agency.5
This paper focuses upon the process of using information from reported incidents to improve the safety of front-line clinical work systems, often referred to as “closing the safety feedback loop.”67 Incident reporting and learning processes originate in safety management systems developed within safety-critical industrial and transport sectors that achieve relatively high levels of operational safety, such as civil aviation.89 Analysis of reported incidents and their root causes can generate potentially useful information regarding systems problems and increase front-line awareness of safety issues in the delivery of care. Such analyses, based upon established human factors approaches, aim to go beyond the immediately apparent to identify the latent causes of systems failures.110 The identification of problem areas is, however, insufficient on its own. Feedback from incident reports must include corrective actions to improve safety and address specific vulnerabilities in care systems, if recurrent failures are to be prevented and the feedback loop closed. Reports in England from the National Audit Office and House of Commons Select Committee have highlighted failures in the capability of existing systems to achieve this and successfully embed learning from incidents in healthcare.1112 Lessons learnt from local incident reporting systems are not widely promulgated, either within or between NHS Trusts, and there is no clear system for monitoring that lessons are learnt or acted upon at the local level.12 National reporting has resulted in only limited feedback to trusts of evidence-based solutions and actions.12 At all levels, there is clearly a need to improve the feedback and sharing of patient safety lessons and solutions.
RESEARCH METHODS
The research described in this article comprised a scoping review that aimed to identify and investigate potentially effective forms of feedback from incident reporting systems for local-level healthcare organisations in the UK.13 The work was commissioned by the Department of Health Patient Safety Research Programme (PSRP). It comprised a multimethod review that aimed to synthesise several evidence sources to develop a framework for best practice that was informed by practical experience with incident reporting in healthcare, high-risk industries and transport sectors. The research comprised the following elements:
systematic scoping review of published policy and research, including review of the feedback capabilities of 23 reporting systems identified from the international healthcare literature;
semistructured interviews with 19 subject-matter experts from a range of industries in order to identify the requirements for effective safety feedback systems;
development of a prescriptive framework for future development of feedback processes in healthcare, based upon qualitative research synthesis and conclusions from a workshop for UK health professionals.
In the review, a mixed methods approach was adopted that combined qualitative research to complement more conventional systematic review methods, including systematic searches, screening of bibliographic records for relevance and use of standardised review criteria. The exploratory nature of the research question lent itself to qualitative investigation based upon elicitation of expert knowledge. In this sense, the research methodology follows recent developments towards more inclusive reviews that seek to synthesise broad sources of evidence in answering practical research questions.1415 The interviews with subject matter experts lasted in duration between 45 and 90 min and used a semistructured interview schedule that included several sections of open-ended questions. Topic areas included: descriptions of safety management systems within specific domains, processes for feedback of safety critical information and barriers/facilitators for effective feedback. Interviews were recorded with the participants permission, and sections were partially transcribed for qualitative analysis.
Literature searches of several online bibliographic databases were conducted using the Ovid and Web Of Science search interfaces. The databases were searched using keyword terms and included EMBASE, MEDLINE, PsycINFO, International Bibliography of the Social Sciences, the Science Citation Index Expanded, Social Sciences Citation Index and Arts and Humanities Citation Index. The search algorithm involved combining three facets to elicit bibliographic records that made reference to three concepts: (1) adverse events and safety-critical incidents (approx. 375 terms), (2) quality and safety improvement systems (approx. 125 terms) and (3) feedback of safety information (approx. 75 terms). A total of 2134 bibliographic records were identified by this search strategy, including 53 from preliminary and hand searches. All records were entered into bibliographic-management software and 132 duplicate records removed. The records were then screened for relevance to the review aims using specific inclusion and exclusion criteria.
All articles detailing organisational processes related to incident monitoring, theoretical and practical issues concerning organisational learning, use of feedback to improve safety and commentary upon the effects of a lack of feedback upon reporting, were included. Examples of excluded topic areas were analyses of specific types of incidents, descriptions of taxonomies for categorising incidents, human factors analysis techniques and legal issues concerning incident reporting, among other areas that did not provide useful information concerning safety feedback. Following screening, 193 records remained, and the characteristics of these sources were described using standardised criteria as part of the scoping review process. In order to investigate potential mechanisms for feedback from incident reporting systems in more detail, 29 articles that reported specific implementations of incident reporting in healthcare were selected from the 193. These articles collectively described 23 distinct systems and were identified on the basis of their inclusion of descriptions of how information from incident monitoring was used to improve operational safety, either through raising awareness or implementing action.
In order to synthesise findings from the different elements of the review into practical output, a framework-building approach was adopted. Subject-matter expertise was used to develop classificatory schemes for feedback processes that were applied and used to interpret the exemplar reporting systems identified from a review of the literature. Expert accounts of how reporting systems operated to improve safety were used by the researchers to understand the incident learning cycle. Specific requirements for the design of effective safety-feedback systems were identified from the research interviews. Based upon the rich qualitative and procedural information identified by the review, an integrative framework was defined to guide the implementation of comprehensive and coherent feedback processes for incident reporting in healthcare. In the sections that follow, the elements that form the output from this review are outlined and discussed.
INCIDENT REPORTING AND FEEDBACK IN THE HEALTHCARE LITERATURE
An incident reporting scheme represents one type of safety information system that relies on front-line staff submitting reports of errors, safety concerns, adverse events and “near misses” that occur within routine work situations. Human factors and safety sciences research has informed effective safety systems in high-risk industries such as chemical processing, offshore oil exploration and nuclear power, as well as transport sectors.1617 There is a growing body of research that describes implementation of incident reporting systems within healthcare organisations.18–30 Examples may now be found of established reporting and learning systems within the healthcare domain that operate at a national level and are designed to produce data on vulnerabilities and actionable information: for example, the Medical Event Reporting System (MERS) and Patient Safety Reporting System (PSRS) developed in the US and UK National Reporting and Learning System (NRLS).31–33 These systems and others were developed based upon expertise drawn from established and well-reported models in various high-risk domains.934
Incident reporting systems operate on the principle that reporting specific events, local investigation of incidents and analysis of aggregated incident data sets can generate useful information to address weaknesses in work systems and processes.35 Information concerning the root causes of failures and near misses can be fed back to the system in the form of corrective actions to prevent recurrence and improve safety. Additionally, information from incident reporting on the incidence of specific failure types and current safety performance can be widely disseminated to front-line staff in order to increase awareness of current operational risks and remedial measures. This current review adopts an inclusive definition of safety feedback as both information and action fed back to improve safety in front-line work systems from incident monitoring. Other authors have similarly made the distinction between feedback of information and follow-up of safety actions from patient safety programmes.7 While the success of an incident reporting system must depend upon the effectiveness of information and action outputs, it must also be understood that learning from reported incidents within an organisational context additionally depends upon the continuous input of incident data into the system through voluntary submission of reports by front-line operators.
Lack of feedback from incident reporting has been highlighted as inhibiting the willingness of staff to report incidents. Barriers that inhibit reporting have been the subject of considerable research in healthcare.36–41 Research has identified several factors that inhibit reporting, including fear of blame, time pressure, resource constraints, the perception that reporting is unnecessary and a lack of clear definitions as to what constitutes a reportable incident.40–42 For these reasons, reported incident rates may not reflect the underlying occurrence of errors and adverse events in practice due to variability in reporting.41 Lack of visible feedback or action arising from reporting, including further investigation of incidents, inhibits future reporting. Firth-Cozens et al found that the perceptions that management does not take action based upon submitted reports, and a lack of resulting changes, lead to apathy among doctors and nurses and reluctance to report incidents.37 Improving feedback in the form of newsletters and information dissemination at monthly departmental meetings has been found to increase reporting rates.43 The key characteristics of several major industry and transport reporting systems have been the subject of review from a healthcare perspective.34 It was found that all the systems reviewed provided some form of feedback to reporting communities, and the need for continuous, timely and meaningful feedback to all relevant stakeholders was emphasised.
From a review of published sources it is apparent that much of the available literature is of a non-experimental, descriptive type that reports case studies of locally implemented systems. Such a trend is not uncommon for research questions that address the effectiveness of organisational processes.44 Relatively little literature and guidance exists that directly addresses the safety action feedback loop, the process by which incident data are transformed into beneficial improvements in operational safety. Bradley et al report a qualitative interview study concerning the effectiveness of data feedback in supporting performance improvement efforts in eight US hospitals. Data quality, timeliness and credibility were identified as important factors for effective improvement, along with leadership and persistence in data feedback processes.45 In consideration of the utilisation of incident data for systems improvement, Kaplan and Fastman highlight two critical determinants for success: (1) timely, effective feedback and (2) demonstrable utility. Timely, effective feedback assures reporters that their reports are acted upon and do not end up in an administrative “black hole.” Demonstrating the local usefulness of incident data, in addition to the development of external reports, influences user adoption and compliance, and can improve reporting rates.46 Gandhi et al describe processes for feedback and follow-up from incident reporting, root cause analysis and executive leadership walkrounds at Brigham and Women’s Hospital Boston, US.7 The importance of assignment of responsibility for improvement to hospital leaders that can effect systems changes is emphasised. The authors comment that, generally, more emphasis needs to be placed upon what happens after a report is submitted and that robust systems must be established to ensure that appropriate follow-up and feedback occur.
In the current review of the international healthcare literature, articles relating to 23 incident reporting systems were identified from 29 separate articles that incorporated descriptions of feedback processes.718–3047–60 These systems represented a range of programme types, including voluntary, anonymous and multi-institutional-level initiatives. The specific feedback mechanisms employed within each system were recorded, including feedback of both action and information outputs from analysis of incident data and investigation of specific incidents. Examples of feedback mechanisms and processes identified from this analysis are included within table 1. The complete list of reporting systems and associated feedback processes identified by the review is reproduced in the online supplement.
The reporting systems reviewed employed a variety of mechanisms for feeding back lessons learnt from incidents, including a range of safety committee processes, publications, electronic dissemination, conferences, education and training means. Considerable variation existed in terms of the frequency of feedback and level of detail or information outputs, as well as the degree to which formal corrective action processes were defined and implemented. Broad workforce safety-awareness publications and email distribution were common.7182055 Related information feedback strategies included feedback notes for medical devices, staff bulletin board postings and the development of error-prevention manuals based upon lessons learnt.475159 Leadership walkrounds and peer ward rounds have been used to promote implementation of safety improvements and make staff aware of actions taken.753 Feedback varied in the degree to which it was adapted to specific user requirements, from generic newsletters to automated provision of individual performance data to the reporting clinician.4950 Best practices established through review of incident data were fed into staff training and education programmes linked to professional accreditation schemes.58 Considerable use of information generated from incident reports and investigations was made by local risk-management and quality-improvement programmes, including presentation at internal patient safety seminars, inter-departmental safety conferences, monthly risk-management meetings and quality reviews, and for safety committee improvement processes.75355
REQUIREMENTS FOR EFFECTIVE SAFETY-FEEDBACK SYSTEMS
In order to understand the characteristics of effective safety-feedback systems, 19 subject-matter experts were interviewed using a semistructured format with open-ended questions. The panel of experts consisted of individuals with safety-management expertise from civil aviation, maritime, energy, rail, offshore production and international healthcare sectors. Several well-established current and former incident reporting programmes were also represented, including: NASA Aviation Safety Reporting System (ASRS), UK NPSA National Reporting and Learning System (NRLS), UK Confidential Human Factors Incident Reporting Programmes (CHIRP) for both general aviation and maritime operations, the Australian Incident Monitoring System (AIMS), the UK Rail Confidential Incident Reporting and Analysis System (CIRAS) and the British Airways Safety Information System (BASIS). Through descriptions of the operation of these systems and thematic analysis of information from safety experts, the main functions of safety feedback were identified in a series of requirements, with rationale, for developing effective systems.
The findings, drawn from experience in incident reporting across multiple domains, show that safety feedback fulfils a number of functions and may be divided into several different modes. Five distinct modes are described within table 2, based upon descriptions of effective feedback processes in the reporting systems outlined above. Collectively, these feedback modes serve corrective, informational and motivational functions; timely feedback of advice to stimulate actions improves systems, while broad dissemination of incident rates and case reports promote awareness of vulnerabilities and correct procedures. Practical experience in established reporting programmes suggests that providing immediate responses and updates to reporters on the progress of a safety issue is important in demonstrating that reports are acted upon and that reporting can be instrumental in achieving visible local improvements. The expert panel suggested that maintaining a dialogue between risk-management systems and staff from local systems in which an incident has occurred is important, as it maintains the opportunity to obtain elaborated information concerning the circumstances of the incident that may not have been available in the initial report. Achievement of this aim was demonstrated in several of the reporting systems reviewed from the literature—for example, through follow-up interviews or debriefings.3059 Safety professionals in other industries understand that front-line staff may provide valuable insight into the causes of failures, how they might be addressed and how new recommendations will work and are best implemented. This contributes to the development of safety solutions and remedial actions that are practical, implementable and likely to be accepted in local work systems.
The modes of feedback outlined above were used to inform the analysis of the reporting systems identified from the review part of the study. All of the articles relating to these 23 reporting systems were selected for inclusion on the basis of descriptions contained within the articles of capability for mode E feedback, a capacity to actually improve clinical work systems using information from incident reports. Although all purported to have the capability to introduce beneficial changes to improve safety, 70% incorporated rapid mode B feedback capabilities for implementing an immediate or provisional response to a reported incident. Over 90% of reporting systems employed newsletters and generic safety awareness publications to disseminate information to front-line personnel regarding operational risks (mode C feedback). Of the 23 systems reviewed, 39% fed back reporter-specific information concerning incident outcome and safety issue progress directly to the original reporter (mode D feedback).
The expert panel interviewed for this study provided practical knowledge concerning the characteristics of effective safety feedback within industry and transport safety-management systems. A series of 15 requirements for the design of effective safety-feedback systems applicable to healthcare were identified from thematic analysis of the interviews. Table 3 lists these requirements along with the design rationale for these features, or how each factor may have a positive impact upon operational safety. Several of the requirements developed from this work bare similarity to the findings of other research in US healthcare, identified from the review part of the study, that addressed data feedback for quality-improvement, including the role of leadership, the credibility of data and continuity of feedback.62
Analysis of multi-domain expertise concerning the design of effective incident reporting systems offers considerable insight into how system requirements, such as those described in table 3, may be implemented to promote effective safety feedback. Multiple modes of feedback may be employed to ensure wide dissemination of operational safety information throughout the organisation to the various professional groups that may have differing information and practical requirements. Feedback processes can be usefully integrated within risk-management operations as part of a comprehensive and coherent safety information strategy. A continuous, repeatable feedback cycle and the capacity for rapid response to safety issues allows timely comprehension and correction of system vulnerabilities. Having an explicit definition of the safety feedback and improvement process provides a model that can itself be improved through continual review of its ability to reduce recurrent incident types and improve operational safety. Effective control of operational safety through feedback requires visible action which is actively supported by both senior management and local clinical leadership.
Appropriate feedback from clinical risk-management systems to the reporting community may reduce inadequacies in understanding of what constitutes a reportable event and provide important information to staff as to how reported incident data will be used.41 The potential therefore exists to improve the quality of the data input to centralised databases for future analyses, through feedback of educational and regular safety information to staff. An important requirement is that future reporting and risk-management systems are designed with both information and action feedback processes in mind. Review of the feedback capabilities of existing systems shows that there has been considerable development in computerised reporting systems that utilise hospital intranet and web-based technologies.53 Such technologies allow the possibility to automate aspects of the feedback process or even provide configurable feedback in the form of direct, ad hoc querying of the incident database and generation of customisable reports tailored to specific user requirements.2124
Safety-feedback processes within an organisation embody a recursive process of learning from operational experience.63 A key requirement emphasised by the safety experts interviewed is that this cyclical process is continuous and that the reporting loop is closed. This means that reporting incidents results in effective interventions and changes in work systems that reduce the likelihood of future harm. Such learning processes have been highlighted as contributing to institutional resilience.64 From an engineering and control paradigm, the process of feeding back information gained regarding the current state of operational safety within a work system to improve future safety may be regarded as cybernetic regulation.65 In order to describe this feedback loop, fig 1 depicts the main functional stages of the learning process for incident reporting, drawing upon descriptions of existing safety systems gained through the interviews and review of available published research and guidance in this area.121735636667

The safety-feedback loop represents an ongoing, cyclical process of reporting, evaluation and corrective action at the organisational level. The main functional stages of this cycle involve: (a) receipt, screening and archiving of incoming reports, (b) analysis of trends in aggregated incident data and investigation of root causality in specific incidents and (c) development and implementation of systems improvements to prevent recurrence and address system vulnerabilities. The outcome from the various forms of analysis of reported incidents may take several forms, such as alerts about new hazards based upon a limited number of reports, trends based upon analysis of large centralised databases or information on emerging best practices in addressing specific safety problems.42 Specific event types may then be monitored proactively, in order to evaluate the effectiveness of corrective measures and detect any inadequacies in existing safety solutions.
For the development of effective feedback systems, the crucial stages of the process depicted in fig 1 are the action formulation and implementation stages for systems improvements, based upon prior analysis of information from incident reports and investigation of contributory factors associated with specific incidents or incident types. In line with the requirements set out above, clear policies must exist to define the process, agents and responsibilities for this corrective action process. How an individual organisation implements these functions may vary according to local structure, conditions and culture. Gandhi et al, for example, provide a description of feedback and follow-up processes that illustrate how the functions relating to feedback within fig 1 may be operationalised within a specific context. In this system, a hospital patient-safety team comprising safety leads, project managers and the medical director is responsible for assigning responsibility and ownership for specific safety follow-up actions.7 Additionally, this group is responsible for feeding back to senior leadership and front-line clinical groups. Interdisciplinary safety committees meet to assist event analysis and formulation of specific system improvements. Committee members normally include leaders in nursing, pharmacy, risk-management, information systems and patient safety, all of whom can take responsibility for the implementation of specific actions. Front-line staff are involved in the committees to help develop effective systems solutions. Each safety issue is tracked as it passes through the safety committee process, with timescales set for follow-up and reporting of overdue items. Following action, the loop is only considered closed at the point of reporting back on the follow-up actions taken to the original reporter. Further monitoring ensures that interventions have the desired impact and that the gains are sustained over time.
IMPLICATIONS FOR HEALTHCARE SYSTEMS
The review described within this article gives rise to several practical findings and recommendations for healthcare reporting systems and associated research, which are outlined in box 1. Additionally, the information gained from this review may provide the basis for the development of a common framework representing current “best practice” knowledge for safety-feedback processes at the organisational level in healthcare. The implications of this are considered below along with the opportunities to use feedback to support positive safety cultures within healthcare organisations.
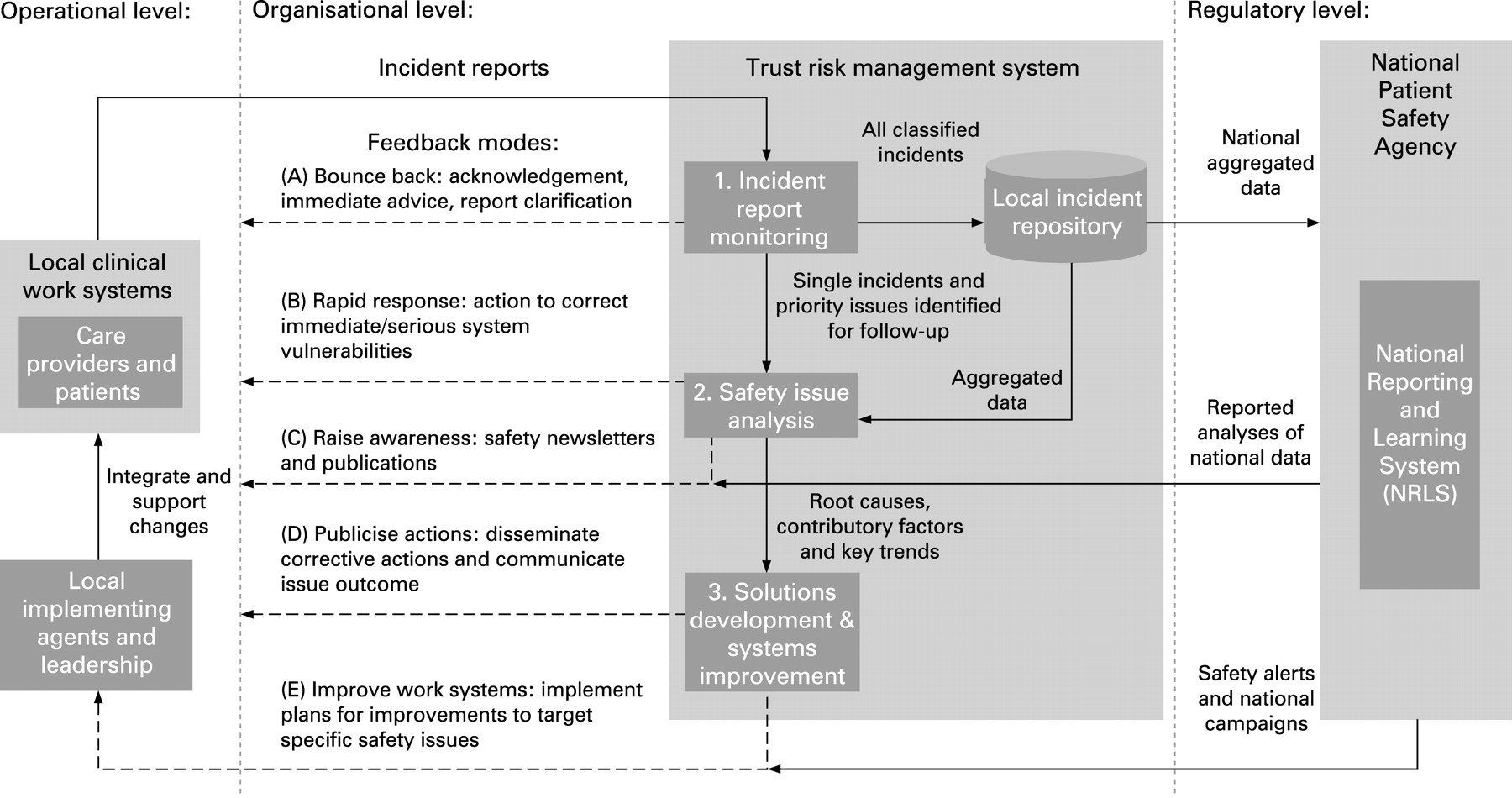
In terms of defining best practices for this area, what is evident from the reporting systems focused upon in this review is that considerable variation exists in terms of the feedback mechanisms employed in each case and the variable degree to which different organisations feed back to reporters and broader clinical communities as a whole. Although the majority of reporting systems described in the literature contributed to safety improvement, they varied in terms of their initial or preliminary responses to incidents and the degree to which this mitigating action occurred rapidly following the reporting of an event. In order to develop a more unified view based upon information gained from the review, fig 2 comprises a framework for information and action feedback from incident reporting. Here, the system requirements and various feedback channels described by safety experts and in the available literature have been synthesised into an overall model that can be related to the stages of processing a reported safety issue at the level of an organisation’s risk-management system. It is important to note that at this local level, specialised processes for follow-up of incidents, of the type indicated within fig 2, require confidential rather than anonymous initial reporting, a lesson that has been learnt in aviation and other industries.9
{kind=link}
{kind=link}
In accordance with the system requirements outlined in table 3, the framework described here illustrates how comprehensive feedback processes might be operationalised to deliver safety critical actions and information to front-line work systems. Information from reporting is used at multiple levels of a centralised or national system by various agencies for different purposes, but here we are primarily concerned with the channels which feed back directly to front-line work systems. Feedback loops operate at both the organisational and supra-organisational or regulatory levels at which data from local systems are aggregated on a national level. This allows learning across organisations from rarely occurring events, remedial action for which is fed back to all local-level organisational systems. All healthcare organisations may then benefit from operational experience in a single organisation, and national remedial measures can be effectively implemented through common local mechanisms.
A common framework for safety-feedback processes that integrates local and national level systems may contribute to an improved capacity for learning from failures at the service level. Recent reports have highlighted that effective safety feedback and learning is often not effectively integrated within current risk-management systems in English NHS Trusts.12 On the level of national or centralised reporting programmes, there is a danger that multiple reporting and feedback channels introduce complexity into the process of implementing guidelines in practice and spreading patient safety lessons.12 The use of common local channels of the type depicted within fig 2 for feeding back information from both organisational and external incident databases may therefore be beneficial.
Even with effective safety-feedback processes, there are limits to the extent that a safety control loop based upon responding to adverse events can prevent novel failure modes occurring in the future. Any safety-management system that relies solely upon analysing incidents is retrospective in focus and should be complemented with proactive, anticipative strategies that promote resilience within work systems and the ability to adapt to future variations safely.68 Capable information and action feedback are fundamental to the support of continuous improvement in care processes, regardless of the source of intelligence on current opportunities and vulnerabilities.
Leaving the architecture of systems for learning aside, the impact of safety feedback upon the development of a positive safety culture within an organisation should not be overlooked. Some authors have linked timely and effective feedback processes with the development of effective reporting and learning cultures within healthcare organisations, commenting that the introduction of supportive characteristics such as feedback may result in as much as a 10-fold increase in reporting rates.46 This review shows that the use of safety newsletter feedback by reporting systems and local risk management to promote safety awareness is common.718–21304851–53555860 Clear policies must exist governing the content of newsletter and other forms of feedback, which are sensitive to the requirements of the various stakeholders with an interest in the information. Industry-safety experts understand that what information is made available to whom and for what purpose are all potentially sensitive issues that may damage trust between front-line staff and management within an organisation, if not handled appropriately.
The long-term success and viability of all reporting systems rely upon the continued disclosure of details concerning operational errors and failures by individuals. Getting the content of feedback right in terms of the message it conveys regarding how incident data will be used, the level of anonymity provided to reporters and the potential consequences of disclosing errors and near misses through reporting are all critical issues that can impact upon reporting culture. Feedback that promotes a systemic, rather than individual, view on the causes of failure can underpin the development of a safety-conscious and just culture within the organisation that is likely to promote the future reporting of failures in care. Such a culture recognises the impact of latent system conditions and contextual factors on individual-level behaviour and error.16 In this way, effective information feedback can promote a systems view on the causes of failures in care, while comprehensive action feedback processes address the latent organisational, managerial, cultural and local work system factors that conspired to produce harm.
CONCLUSIONS
This article has attempted to capture the rationale that underlies effective feedback processes, based upon a review of the available literature and experience in several well-established industrial, transport and healthcare reporting programmes. To this end, a general framework for the development of best practice in the area of feedback from incident-reporting systems has been proposed. The findings from this review suggest that effective feedback relies upon both timely corrective actions to improve systems and broad information dissemination to raise awareness of current vulnerabilities at the front line. Adequate feedback on safety issue progress and dialogue with front-line staff ensures solutions are effective, are accepted and encourage future reporting. Timely, useful feedback on safety-issues delivered through convenient and effective channels can promote the development of a positive safety culture within the organisation. The organisational safety-feedback loop must be closed and operate as a continuous, rather than temporary or “special case” process. Current safety issues may then be detected promptly through reporting and local investigation, resulting in practical safety solutions that are actioned to prevent recurrent failures.
The review described in this article is limited by the extent to which information concerning the operational details of feedback processes for established healthcare reporting systems is determinable from the available published literature on the subject. Based upon expert opinion in this area, the requirements and characteristics for effective feedback systems described within this article are grounded in practical experience across domains but have not yet been evaluated systematically in healthcare. Further survey of international best practices in this area, drawing upon the frameworks and criteria established within this article, would extend current understanding and promote sharing of mechanisms and strategies that have been found to be effective in various local contexts. Future development in reporting systems must compliment the detection, analysis and investigation of adverse events with serious consideration of the practical issues surrounding how to use the information gained from such activities to improve operational safety. Considerable scope exists, for example, for research that seeks to evaluate the relative impact of different types of information and action feedback processes. The challenge remains to develop more effective feedback systems that promote learning from patient-safety incidents and continuous improvement in the clinical work systems that give rise to them.
Box 1 Key messages for healthcare reporting systems
Considerable effort has gone into establishing reporting systems in healthcare; it is less clear as to how the information from incident reporting and analysis can be used effectively to improve patient safety in care delivery processes, effectively closing the safety-feedback loop.
Effective safety feedback does not rely solely upon publicising incident rates, but rather involves timely, visible and repeatable corrective action and quality-improvement processes.
Multiple means of feeding back actions and safety information should be employed to promote safety awareness, improve clinical processes and maintain reporting.
The relative effectiveness of different feedback mechanisms for incident reporting and situations in which they are optimally applicable is not currently well understood or based upon evaluative evidence.
A comprehensive, common framework that incorporates multiple modes of feedback would be of benefit for risk-management systems in healthcare organisations. Such a framework should include both information and action-feedback processes in order to promote patient safety.
Acknowledgments
Contributions to this research by D Lusher (Terema), L Earll (Researchthatworks), the international panel of safety experts that contributed to this research and the UK patient safety managers, risk managers and other health professionals that attended the associated workshop event on feedback from incident reporting in Coventry, UK are gratefully acknowledged.
REFERENCES
Supplementary materials
web only appendix 18/1/11
Files in this Data Supplement:
Footnotes
See Editorial, p 2
A supplementary table is published online only at http://qshc.bmj.com/content/vol18/issue1
Funding: UK Department of Health Patient Safety Research Programme.
Competing interests: None.
Ethics approval: Ethics approval was provided by Thames Valley Multi-Centre Research Ethics Committee 05/MRE12/13.