Article Text

Abstract
Objective To describe relationships between teamwork behaviours and errors during neonatal resuscitation.
Methods Trained observers viewed video recordings of neonatal resuscitations (n = 12) for the occurrence of teamwork behaviours and errors. Teamwork state behaviours (such as vigilance and workload management, which extend for some duration) were assessed as the percentage of each resuscitation that the behaviour was observed and correlated with the percentage of observed errors. Teamwork event behaviours (such as information sharing, inquiry and assertion, which occur at specific times) were counted in 20-s intervals before and after resuscitation steps, and a generalised linear mixed model was calculated to evaluate relationships between these behaviours and errors.
Results Resuscitation teams who were more vigilant committed fewer errors (Spearman's ρ for vigilance and errors = −0.62, 95% CI −0.07 to −0.87, p = 0.031). Assertions were more likely to occur before errors than correct steps (OR = 1.44, 95% CI 1.10 to 1.89, p = 0.008) and teaching/advising occurred less frequently after errors (OR = 0.59, 95% CI 0.37 to 0.94, p = 0.028). Though not statistically significant, there was less information sharing before errors (OR = 0.90, 95% CI 0.77 to 1.05, p = 0.172).
Conclusions Vigilance is an important behaviour for error management. Assertion may have caused errors, or perhaps was an indicator for some other factor that caused errors. Teams may have preferred to resolve errors directly, rather than using errors as opportunities to teach their teammates. These observations raise important questions about the appropriate use of some teamwork behaviours and how to include them in team training programmes.
Statistics from Altmetric.com
There is almost no debate about the belief that good teamwork improves the quality and safety of healthcare. Poor teamwork is associated with poor quality in neonatal intensive care,1–3 emergency departments,4 the operating room,5 6 trauma resuscitation,7–9 and among residents of all disciplines.10 Thus, influential organisations such as the Institute of Medicine, Joint Commission and the Agency for Healthcare Research and Quality (AHRQ) recommend team training for healthcare providers. In fact, AHRQ is disseminating a team training programme for healthcare providers throughout the USA.11 But even as influential organisations disseminate team training programmes, recent studies have concluded that that team training does not improve teamwork or the quality of care.12–14
Given the substantial effort directed towards team training, coupled with its weak and conflicted evidence base, there is a need for more research. Some of this research should focus on development, implementation and evaluation of training programmes,2 12 14 but other research needs to ask more fundamental questions about the relationships between specific team behaviours and specific tasks carried out by providers.15 16 Observations of teams who have not had team training is one way to understand how some behaviours may or may not be useful for preventing or managing errors.16 To address that issue, we analysed video recordings of 12 infants who required intubation in the delivery room. The two specific aims were to (1) determine if the teamwork behaviours vigilance and workload management were correlated with the percentage of resuscitation steps judged to be in error and (2) determine whether other teamwork behaviours were associated with neonatal resuscitation errors.
Methods
Resuscitations
We analysed 12 video recordings of neonatal resuscitations that were selected from a set of 132 resuscitations of infants born by caesarean section in an urban teaching hospital.2 The hospital had an 80-bed neonatal intensive care unit and approximately 3400 deliveries during the study year. The 12 selected resuscitations included or should have included intubation. Based upon our previous work with the full set of 132 resuscitations, we knew that more complicated resuscitations, such as those involving intubation, contained more teamwork behaviours.2 Eleven of the 12 resuscitations included at least one intubation attempt, and one resuscitation team did not attempt to intubate the infant but should have according to Neonatal Resuscitation Program (NRP) guidelines. The other 120 resuscitations did not include intubation (in accordance with NRP guidelines) and were not included in this study.
The resuscitation teams included neonatal transport nurses, respiratory therapists, paediatric residents, fellows and attending physicians. All but one of the resuscitations in this study included a fellow or an attending physician on the team. Low-risk deliveries at the study hospital often did not include a fellow or attending physician; 13.8% of the 132 caesarean section resuscitations included a fellow and 3.8% included an attending physician.2 None of the providers on the resuscitation teams had received teamwork training. The newborns' birth weights ranged from 657 to 3755 g, and gestational ages ranged from 24 to 41 weeks (table 1).
Provider team members and newborn characteristics for neonatal resuscitations
The resuscitations occurred in a resuscitation room adjoining two labour and delivery operating rooms. Videos were recorded 24 h a day, Monday–Friday between 1 January and 31 December 2002. The institutional review board approved the study protocol and each provider gave consent to be video recorded. Video cameras were focused on each radiant warmer in the resuscitation room to capture a close up view of the infant (camera A). Another camera was placed in the corner of the ceiling to provide a view of all providers on the resuscitation team (camera B). Nurses were responsible for starting and stopping the video recordings. A research assistant collected the video tapes each day and downloaded the files to a computer.2 The two video recordings for each resuscitation (from cameras A and B) were edited to begin and end at the same time, providing two video camera angles synchronised in time to visualise each resuscitation.
Data collection
The NRP consists of a series of steps that providers should carry out to resuscitate an infant. Two NRP instructors scored the resuscitation steps for errors. At the time of data collection, these observers had been registered nurses for more than 25 years, NRP instructors for 12 years and NRP regional trainers for 2 years. Teamwork behaviours were scored by two trained observers who were research assistants (one in psychology and one in clinical research). NRP errors and teamwork behaviours were scored using Noldus Observer software (version 5.0, Noldus Information Technology, Wageningen, The Netherlands). Both pairs of observers were from outside institutions and were not personally familiar with the study participants.
Teamwork observers trained for approximately 40 h over 5 months to standardise scoring of teamwork behaviours. The observers first discussed the teamwork behaviours with an investigator (EJT) and observed a training video that illustrated teamwork behaviours during neonatal resuscitations. Next, the teamwork observers and the investigator independently scored two intubation resuscitations not included in the data set and met afterwards to discuss differences in their teamwork observations and refined teamwork definitions. The teamwork observers then scored a total of 28 resuscitation videos divided into five phases. At the end of each phase, Cohen's κ was calculated to determine inter-rater reliability for each teamwork behaviour and areas of disagreement were discussed among the investigators and reviewers. During the final phase of scoring, Cohen's κ for the teamwork behaviours was 0.54 for workload management, 0.57 for evaluation of plans, 0.59 for vigilance, 0.65 for teaching/advising, 0.66 for information sharing, 0.82 for inquiry, 0.87 for assertion and 1.00 for intentions shared.
NRP observers trained for approximately 25 h over 3 months to standardise the scoring of NRP steps and errors. The observers independently scored a total of eight resuscitation videos during the training period. Cohen's κ for NRP observers' scoring of errors was 0.70 for the eight resuscitation videos observed during training.
The observers for errors each scored six resuscitations (half of the sample). Errors were defined as instances when a team did not complete an indicated step, when they completed a step that was not indicated, or when a step was performed incorrectly. Video recordings from cameras A and B for each resuscitation were scored for correct and incorrect steps, and the data files from both video cameras were merged together to create one record of NRP steps per resuscitation.
The two teamwork observers each scored all 12 resuscitation videos from cameras A and B. Six teamwork behaviours were scored as events: (1) information sharing, (2) inquiry, (3) assertion, (4) intentions shared, (5) teaching/advising and (6) evaluation of plans. Event scoring indicates that the behaviour occurred at a specific point in time, but did not continue for any duration. Two teamwork behaviours, vigilance and workload management, were scored as states. State scoring indicates that the behaviour extended for some duration. The teamwork behaviours measured in this study are defined in table 2 and have been adapted from commercial aviation Crew Resource Management programmes.2 17 18
Definitions of teamwork behaviours
Vigilance and workload management are conceptually different than the other teamwork behaviours. Vigilance and workload management extend for some duration, while other behaviours (like information sharing) are discrete events. At any point during a given resuscitation, the team is either vigilant or not vigilant, and managing their workload or not managing their workload. Other behaviours are best characterised as instantaneous events.
The data files from cameras A and B were merged together to create one record of teamwork behaviours for each resuscitation per observer. The two observer records for each resuscitation were merged together so that each file contained teamwork observations from both teamwork observers. If duplicate teamwork codes by the two observers occurred within 2 s, the second teamwork code was removed from the record (ie, it was assumed to represent the same behaviour as the first code). This procedure of combining records from both teamwork observers increased sensitivity for detecting teamwork behaviours. The 12 teamwork observations were then merged with the 12 observations of NRP steps for analysis.
Analyses
Our first aim was to determine if teamwork state behaviours (vigilance and workload management) were correlated with the percentage of NRP steps judged to be in error. Teamwork observers viewed each resuscitation and noted times when vigilance and/or workload management were exhibited by the team and times when the behaviours were not exhibited. Teamwork state percentages were calculated as the total time the team demonstrated each behaviour divided by the total resuscitation time (from the placement of the newborn on the warmer to the stabilisation of the infant, indicated by calling for transport to neonatal intensive care). We hypothesised that teams who were more vigilant and exhibited more workload management would commit fewer errors during the resuscitation procedure. The overall percentage of vigilance and workload management was correlated with the overall percentage of NRP errors by calculating Spearman's ρ.
The second aim was to determine whether specific teamwork event behaviours were associated with the occurrence of NRP errors. A generalised linear mixed model (logit) was calculated with a dichotomous dependent variable indicating whether an error occurred for each NRP step performed. The independent variables in the model were the number of teamwork behaviours occurring in the 20 s before or after each step. All teamwork event behaviours were included in one model. Two teamwork behaviours were very rare (evaluation of plans and intentions shared), so we excluded them from the analyses. We analysed four teamwork event behaviours in the model (sharing information, inquiry, assertion and teaching/advising). All analyses were performed using STATA (Intercooled STATA V.9.2, College Station, Texas, USA).
A 20-s time window was chosen to relate teamwork events to NRP steps after examining the data in 5-, 10-, 15-, 20-, 25- and 30-s windows. Differences in the number of teamwork behaviours occurring before and after errors were apparent with time windows of 20 s or more. A causal relationship between teamwork behaviour and an NRP step is harder to justify the longer the separation in time between the two. The 20-s time window was selected as the best compromise between sufficient time to include relevant behaviours but not irrelevant behaviours.
The resuscitations were divided into five phases according to NRP guidelines: (1) preparation and initial steps, (2) oxygen administration, (3) bag/mask ventilation, (4) chest compressions and (5) intubation and drug administration. We combined the intubation and drug administration NRP phases because our sample only included one resuscitation in which drugs were given. Our generalised linear mixed model accounted for correlations among resuscitation steps completed within each resuscitation phase and within each team. Accounting for these correlations within phases and teams was necessary because each resuscitation involved multiple steps and phases.
Results
Table 3 describes the median percentage of observed teamwork states per resuscitation. Although many resuscitation teams were vigilant at all times, some were not. Any lapses in vigilance may be important given the life threatening situation.
Median percentage duration of teamwork states per resuscitation
During the 12 resuscitations, a total of 756 teamwork event behaviours were observed. Table 4 presents the median number of observed teamwork events per resuscitation. Information sharing, inquiry and assertion accounted for most of the teamwork behaviours observed. We excluded intentions shared and evaluation of plans from the analyses because these behaviours were rarely observed.
Median number of teamwork events per resuscitation
During the 12 resuscitations, 547 NRP steps were observed: 152 (27.8%) incorrect (errors) and 395 (72.2%) correct. The number of NRP steps and errors recorded in the five phases are presented in table 5. Most of the NRP steps (86%) and errors (91%) were recorded in phases 1 (preparation and initial steps), 3 (bag/mask ventilation) and 5 (intubation and drug administration).
Description of observed NRP steps and errors by phases
Teamwork states
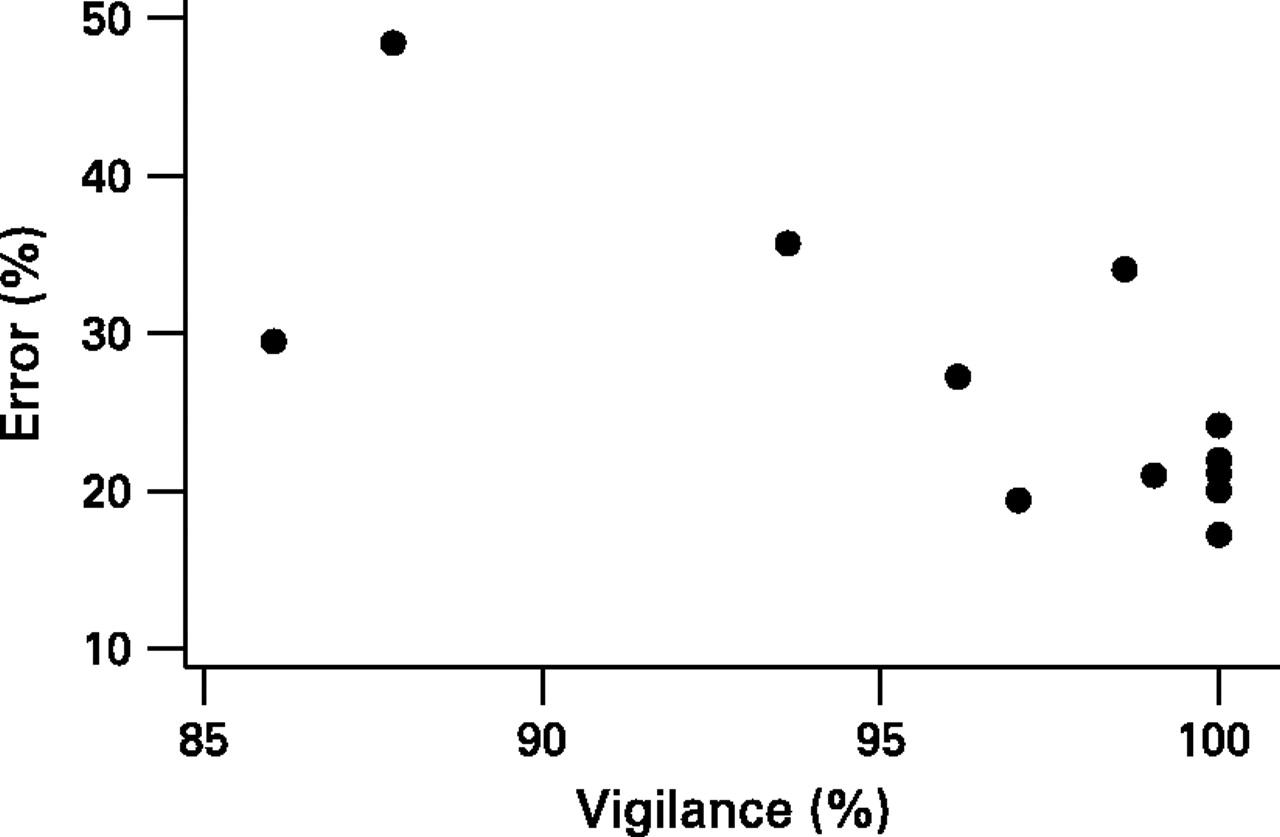
Vigilance was negatively correlated with NRP errors (Spearman's ρ = −0.62, 95% CI −0.07 to −0.87, p = 0.031) (fig 1). Teams that were more vigilant had a lower proportion of errors than teams that were less vigilant. The five teams that maintained their vigilance throughout the resuscitation had error rates of less than 25%. In contrast, five of the seven teams that lacked sustained vigilance throughout the resuscitations had error rates exceeding 25%. No significant correlation was found between workload management and NRP errors (Spearman's ρ = −0.15, 95% CI −0.65 to 0.44, p = 0.633).
{kind=link}
Proportions of vigilance and errors during neonatal resuscitations (Spearman's ρ = −0.62, 95% CI −0.07 to −0.87, p = 0.031).
Teamwork event behaviours
The associations between the teamwork event behaviours and errors were evaluated by odds ratio calculated from a generalised linear mixed model. The associations between teamwork event behaviours and NRP errors are presented in table 6.
Results from the generalised linear mixed model indicating associations between teamwork behaviours and NRP errors
More assertions before NRP steps significantly increased the odds of an error. One additional assertion before an NRP step increased the odds of an error by 44%. Teaching/advising was less likely to occur after an error than after a correct NRP step. We also observed a trend for less information sharing before NRP errors.
Discussion
We assessed the relationships among teamwork behaviours and errors during neonatal resuscitation and found that teams who were more vigilant committed fewer errors. In addition, assertion occurred more often before errors than correctly performed steps and teaching/advising occurred more often after correct steps than errors. There was also more information sharing before correct steps, although this relationship did not reach significance at the 0.05 level. Each of these observed temporal sequences raises interesting questions about when and even if, teams should use these behaviours.
These behaviours were derived from those found to be useful in Crew Resource Management Programmes of commercial aviation and during observations of aircrews.17 19 In that setting, these behaviours are called threat and error management behaviours.20 The word “management” means that the behaviours could be used to both prevent errors and respond to errors. Our findings help confirm that this model also applies to healthcare teams during neonatal resuscitation. For example, the association between more vigilance and fewer errors suggests that vigilance may prevent errors, or trap errors and prevent them from propagating. Vigilance is an observable component of broader team concepts such as situational awareness21 22 or team monitoring23 that are widely thought to be important determinants of safe care.
However, we also found that assertion was more frequent before errors than before correctly performed steps. One interpretation is that this behaviour actually caused, instead of prevented errors. Assertions may have distracted other team members from the resuscitation tasks and thus caused errors. As none of the providers in this study had teamwork training, their assertions were typically short imperative statements advocating more aggressive resuscitation techniques for infants that were not responding to the current methods (eg, “Let's intubate” and “We need to do chest compressions”). It is possible that different styles of assertion, perhaps modelled after SBAR (situation, background, assessment and recommendation),24 could be taught to these providers and might result in lower risk of subsequent errors. Another interpretation of this finding is that assertion did not cause errors but instead relates to another factor that caused the errors. For example, assertion may indicate a high illness severity in the newborn, causing the team to rush through the resuscitation, skipping NRP steps or performing them incorrectly. Assertions for more aggressive resuscitation techniques were a direct result of high illness severity in the newborns. The time immediately following these assertions typically included preparing and providing resuscitation methods not yet performed on the infant, thus increasing the chances for errors to occur. On one hand, assertion causing errors seems unlikely given the enthusiastic support for the use of behaviours like these by numerous experts and healthcare consultants. On the other hand, two reviews of the literature12 13 and a large randomised trail of team training14 have found no benefit of team training on the quality or safety of care. This finding should at least remind us to not automatically assume that so-called teamwork behaviours are beneficial to patient care.
Teaching and advising were less likely to occur in the 20 s after an error than after a correct step. This may indicate that teams were focused on resolving errors and stabilising the infant rather than using the occurrence of errors as opportunities to teach their teammates. Although the relationship between information sharing and errors was not statistically significant, the finding suggests that more information sharing before NRP steps may prevent errors.
While other groups have identified important team behaviours and concepts for a variety of care settings,3 4 6 21 23 this study is unique in that it looked at very specific temporal relationships among team behaviours and errors. Other strengths include the attention to observer training and the richness of the dataset—we observed 547 NRP steps (152 errors) and 756 teamwork event behaviours. The large number of observed behaviours and errors allowed us to use advanced statistical methods to examine temporal relationships between teamwork and errors.
The study is limited by its observational design; the results and conclusions are exploratory and open to several interpretations as noted above. The results may not be generalisable beyond academic settings, to teams that have received team training (these teams had not received any team training), or to resuscitations that do not include intubation. While it is possible that the observations of errors occurring after team behaviours were due to inappropriate expression of those team behaviours, the observers for this analysis (and a previous analysis of these resuscitations)2 did not notice obviously inappropriate team behaviours.
In conclusion, our results reinforce the existing belief that team behaviours are best thought of as error management, not just error prevention, behaviours and that vigilance is a particularly useful error management behaviour. The study also raises questions about whether or not assertion could prompt errors or be associated with other factors that lead to errors. Such findings emphasise the need for thoughtful evaluation of which behaviours should be taught in team training programmes.
References
Footnotes
Funding This study was funded by AHRQ grants 1PO1HS1154401 and U18HS1116401.
Competing interests None.