Article Text

Abstract
Background Prevention of healthcare-associated urinary tract infection (UTI) has been the focus of a national effort, yet appropriate indications for insertion and removal of urinary catheters (UC) among surgical patients remain poorly defined.
Methods We developed and implemented a standardised approach to perioperative UC use to reduce postsurgical UTI including standard criteria for catheter insertion, training of staff to insert UC using sterile technique and standardised removal in the operating room and surgical unit using a nurse-initiated medical directive. We performed an interrupted time series analysis up to 2 years following intervention. The primary outcome was the proportion of patients who developed postsurgical UTI within 30 days as measured by the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP). Process measures included monthly UC insertions, removals in the operating room and UC days per patient-days on surgical units.
Results At baseline, 22.5% of patients were catheterised for surgery, none were removed in the operating room and catheter-days per patient-days were 17.4% on surgical units. Following implementation of intervention, monthly catheter removal in the operating room immediately increased (range 12.2%–30.0%) while monthly UC insertion decreased more slowly before being sustained below baseline for 12 months (range 8.4%–15.6%). Monthly catheter-days per patient-days decreased to 8.3% immediately following intervention with a sustained shift below the mean in the final 8 months. Postsurgical UTI decreased from 2.5% (95% CI 2.0-3.1%) to 1.4% (95% CI 1.1-1.9; p=0.002) during the intervention period.
Conclusions Standardised perioperative UC practices resulted in measurable improvement in postsurgical UTI. These appropriateness criteria for perioperative UC use among a broad range of surgical services could inform best practices for hospitals participating in ACS NSQIP.
- surgery
- quality improvement
- infection control
Statistics from Altmetric.com
Introduction
Urinary tract infection (UTI) is one of the most common postsurgical infections, contributing to increased morbidity, hospital length of stay and hospital cost.1 2 At least half of all hospital-acquired UTIs are believed to be avoidable2 and overuse of perioperative urinary catheters (UC) and breaches in infection control practices contribute to the majority of these. Increased attention has been paid to hospital-acquired UTI prevention since 2008 after the Centers for Medicare and Medicaid Services introduced non-payment to hospitals for patients who developed catheter-associated UTI.3 A national effort has been under way since 2009 to improve catheter-associated UTI rates in the USA resulting in a measured decrease among 10% of American hospitals.4
Despite this, there is tremendous need for improvement among surgical patients. UC use in the operating room relies heavily on individual preferences of surgeons and anaesthetists.1 2 5 6 Guidelines put forward by the US Centers for Disease Control and Prevention (CDC) in 2009 specified that perioperative UCs should be restricted to surgeries involving or contiguous to genitourinary structures, or with anticipated prolonged duration or requiring large-volume infusions or diuretics during surgery, or needing intraoperative monitoring of urinary output.1 Although these criteria were an instrumental first step in defining appropriateness, they leave significant room for interpretation around the duration of surgery requiring catheterisation and how to determine the need for intraoperative monitoring of urine output. Further, catheter removal at the conclusion of the case was not considered as a potential intervention for reducing catheter exposure, nor is it addressed in guidelines. Once patients are transferred to the ward, prior studies have suggested that physicians are often unaware of which patients remain catheterised and are slow to remove them postoperatively.7
To assist hospitals in reducing UTI among surgical patients, the American College of Surgeon’s National Surgical Quality Improvement Program (ACS NSQIP) provides risk-adjusted peer comparison of postoperative UTI within 30 days of surgery. Despite over 560 participating hospitals across North America, few studies have reported their processes and outcomes in addressing high rates of postoperative UTIs. We hypothesised that standardisation of perioperative UC use based on consensus criteria for perioperative insertion and removal could result in improvement in postsurgical UTI as measured by ACS NSQIP.
Methods
Setting and surveillance definition
Sunnybrook Health Sciences Centre is a tertiary care hospital with over 600 acute care beds and performs around 15 000 surgical procedures annually. The hospital joined ACS NSQIP in 2013 and began to receive postsurgical UTI rates each quarter for patients admitted to general surgery, vascular surgery, neurosurgery, orthopaedic surgery and plastic surgery. Postsurgical UTI is defined by the ACS NSQIP as symptomatic UTI based on the symptoms included in the National Healthcare Safety Network (NHSN) surveillance definition within 30 days of an operative procedure. This definition involves the presence of at least one of the following symptoms (fever >38.0, urgency, frequency, dysuria, suprapubic tenderness, costovertebral angle pain or tenderness) and a urine culture with >100 000 colonies/mL urine up to 72 hours after or 24 hours prior to signs or symptoms. The data from ACS NSQIP are generated by retrospective chart review of hundreds of randomly selected cases each quarter to identify an estimate of the percentage of surgical cases that developed postsurgical UTI. Each chart review is performed by a trained independent chart abstractor who is not involved in the Quality Improvement team.
Baseline state
The postsurgical UTI rates on our surgical services were 3.3% in 2013, which was among the highest (10th decile) compared with 560 other North American hospitals. Review of operating room records in 2014 confirmed that 37.5% (3698/9851) of patients were being catheterised for surgery based on individual surgeon or anaesthetist’s discretion. Different operating room personnel performed UC insertion and frequently this involved a junior team member such as a resident or student who had limited prior training in use of sterile technique. On inpatient units, a point prevalence audit on inpatient wards demonstrated that 19% (54/273) of patients were catheterised even though 69% (37/54) lacked an appropriate guideline-based indication1 corresponding to 52.5% (386/747) unnecessary catheter-days. Semistructured interviews with front-line nurses demonstrated that 74% (40/54) were unaware of the reasons for maintaining a UC. On the physician side, 80% (28/35) acknowledged that on a busy surgical ward, it is difficult to reassess the need for UCs and that removal is often delayed.
Achieving consensus
Before developing standard practices around perioperative urinary catheterisation, we first sought to achieve consensus among the 124 surgeons and eight surgical advance practice nurses at our institution regarding appropriateness criteria for all surgical patients (not limited to surgical specialties where postsurgical UTI was available). Based on the CDC guidelines as a starting point, in-person and online discussions were held from November 2014 to May 2015 until consensus was reached on specific criteria for insertion of a UC and the duration of time it should remain in place for all surgical patients (table 1). These criteria were used for the development of policy for restrictive UC insertion in the operating room and the medical directive for nurses, allowing for postoperative removal of catheters by nurses on the ward.
Consensus criteria for urinary catheter insertion and maintenance in perioperative period for all surgical patients at a tertiary care centre
Restrictive UC insertion
Effective May 2015, the criteria for UC insertion were included in a new operating room policy and introduced through multiple training sessions as follows: operating room nurses received weekly reminders for 1 month; surgical fellows and residents reviewed the criteria during their orientation and all staff surgeons were made aware of these during faculty meetings. It was decided that all staff should assess the need for the UC at the end of each procedure before transferring the patient to the postanaesthetic care unit. Therefore, asking the question ‘Can this catheter be removed before transfer?’ was added to the policy.
Sterile insertion of UCs
Effective April 2015, all medical students were required to participate in a mandatory simulation laboratory on UC insertion after completing an online training module. During the simulation session, medical students were given five scenarios to test their knowledge of the criteria for catheter insertion in the operating room. Once the decision to insert a catheter was made, students proceeded to practise UC insertion following all the necessary steps using sterile technique. A facilitator was available to guide and teach the students. Successful completion of the simulation lab required three correct UC insertions. Surgical fellows and residents were required to complete an online training module before they were allowed to begin their rotation. Catheter insertion was audited in the operating room to ensure proper sterile techniques and that criteria were followed.
Medical directive for nurse-initiated UC removal
To standardise postoperative removal of UCs, a medical directive was created for nurse-initiated removal on postoperative day 2 at 06:00. A medical directive is an order given in advance by physicians (or others authorised to write orders) to enable a qualified health professional (typically a nurse) to apply the order under specific conditions without a direct assessment by the physician at the time.8 This model of care was cocreated by advance practice nurses in our hospital and first piloted successfully among general medicine patients,9 then adapted for surgical patients based on the consensus criteria of all staff surgeons.
The medical directive was intended to be applied by nurses in the morning of postoperative day 2. Nurses were to remove the UC by default unless the patient met one of the listed exclusion criteria (Table 1). Once the catheter was removed, a simple algorithm was used to provide postcatheter care and to address any urinary retention (see online supplementary appendix).
Supplementary file 1
Prior to implementation in July 2015, all nurses on surgical wards underwent a 30 min training session where they were given cases to practise applying the medical directive. Advance Practice Nurses who were instrumental in creating the medical directive played a supervisory role and performed weekly random audits to confirm adherence between July 2015 and July 2016.
Equipment factors
During implementation of the medical directive, it became apparent that multiple equipment factors needed to be addressed in order to improve sustainability. Nurses commented that condom catheters often fell off and bladder scanners were frequently under repair and unavailable. We implemented better adhesive condom catheters which were rated as a superior product by 100% (35/35) of nurses surveyed. All surgical units were equipped with a second bladder scanner device and to improve their availability, biomedical engineers were trained to perform any repairs in-house instead of sending it to manufacturing.
Measures
The primary outcome was the number of postoperative UTIs within 30 days of surgery per 100 surgical cases, derived from random chart reviews by an independent chart abstractor through ACS NSQIP. The definition of postsurgical UTI put forward by NSQIP remained unchanged throughout the study period. Process measures included UC insertions in the operating room, removals at the end of case and the number of catheter-days per patient-days across all surgical wards, using a validated electronic UC surveillance tool and normalised to patient census.10
Statistical analysis
We performed an interrupted time series analysis of UC insertions, removals at end of case and overall utilisation ratio (catheter-days per patient-days) across all surgical wards. Statistical process control was used to compare the baseline period (December 2014 to March 2015) to the implementation period (April to June 2015) and the intervention period (July 2015 to March 2017). Control limits of P-charts were set at 3 σ (equivalent to 3 SDs) where consecutive points below the lower control limits represent a significant decrease equivalent to p<0.01.11 All analyses were performed with Excel (V.15.0) and QI Macros (KnowWare International, V.2013.07). The study was approved by the Research Ethics Board of Sunnybrook Hospital, Toronto, Ontario, Canada. The need for individual consent to be included in the analysis was waived.
Results
At baseline, the median age of patients undergoing surgery was 57 years (IQR 26) and 46.6% (1007/2162) of patients were female, as compared with 57 (IQR 27) and 46.4% (9000/19 499) during the implementation/intervention periods. The median duration of surgery was 94 min (IQR 89) as compared with 93 min (IQR 89) during the implementation/intervention periods.
Throughout the implementation and intervention periods, 60/61 (98.4%) rotating clinical clerks and 107/146 (73.3%) surgical residents completed the training. On the surgical units, 198/220 (90%) nurses underwent 30 min training on how to use the medical directive to remove UCs on surgical units.
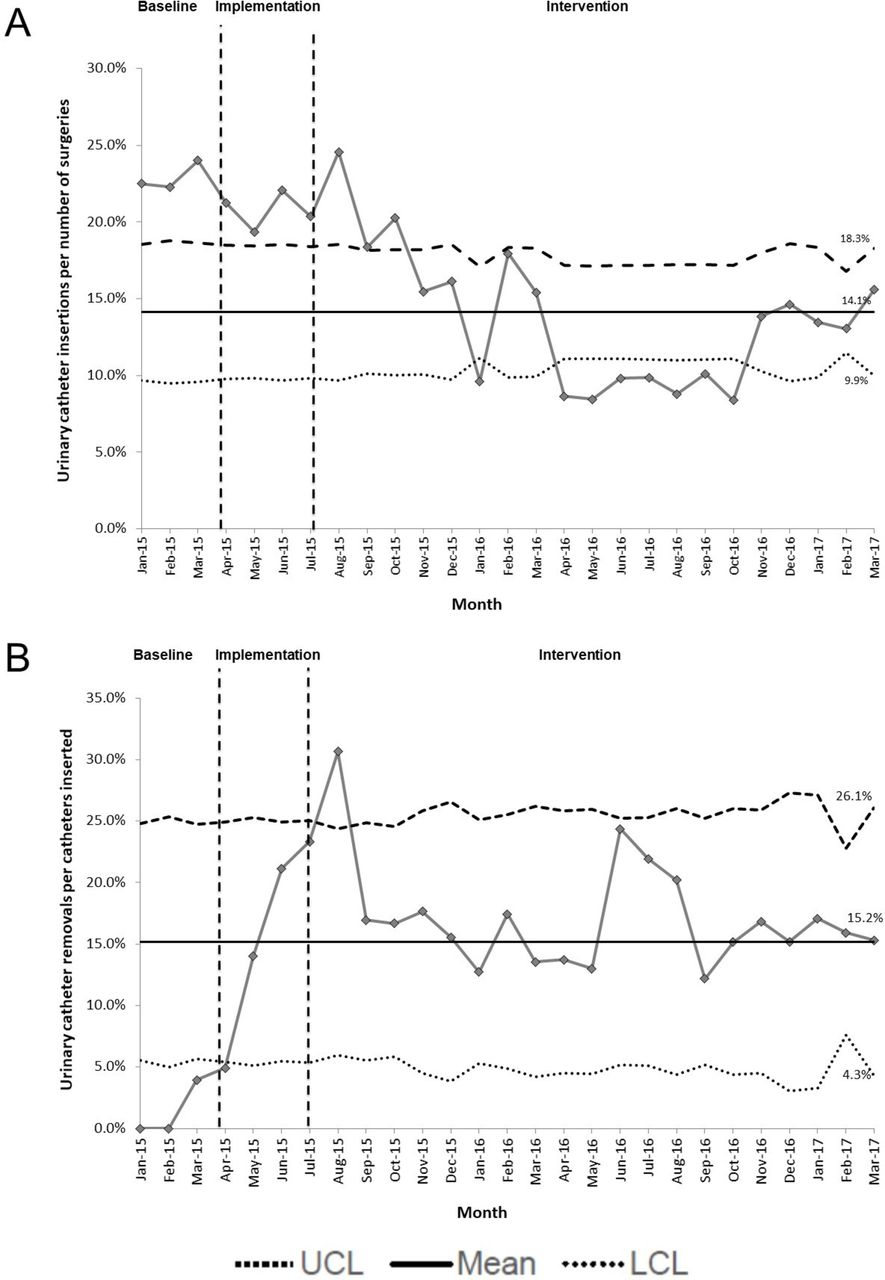
Figure 1A,B depicts rates of UC insertion preprocedure and removal postprocedure in the operating room, respectively. At baseline, 22.5% (486/2162; 95% CI 20.1% to 24.3%) of patients were catheterised for surgery and none were removed at the end of the case. Following implementation of the intervention, catheter removal at the end of the case increased significantly above 3 σ (42/137; 30%, 95% CI 23.6% to 38.8%) while UC insertion took longer to decrease with an eventual shift below 3 σ from April to October 2016 (744/8150; 9.1%, 95% CI 8.5% to 9.8%). Catheter insertions subsequently drifted upward from November 2016 to March 2017 while remaining significantly below baseline (561/4048; 13.9%; 95% CI 12.8% to 15.0%; p=0.0001). The number of catheters removed at the end of surgery regressed to the mean as fewer catheters were being inserted, with 16.4% (341/2076; 95% CI 14.9% to 18.1%) of inserted catheters that continued to be removed between September 2015 and March 2017. On surgical wards, baseline catheter-days per patient-days were 3451/19 880 (17.4%, 95% CI 16.9% to 17.9%) and reached below 3 σ to 623/5043 (12.4%, 95% CI 11.5% to 13.3%) at the beginning of intervention period with a sustained shift below the mean from August 2016 to March 2017 (figure 2). Weekly random audits on surgical units confirmed high compliance of catheter removal with 426/485 (87.8%) UCs meeting exclusion criteria for the medical directive.
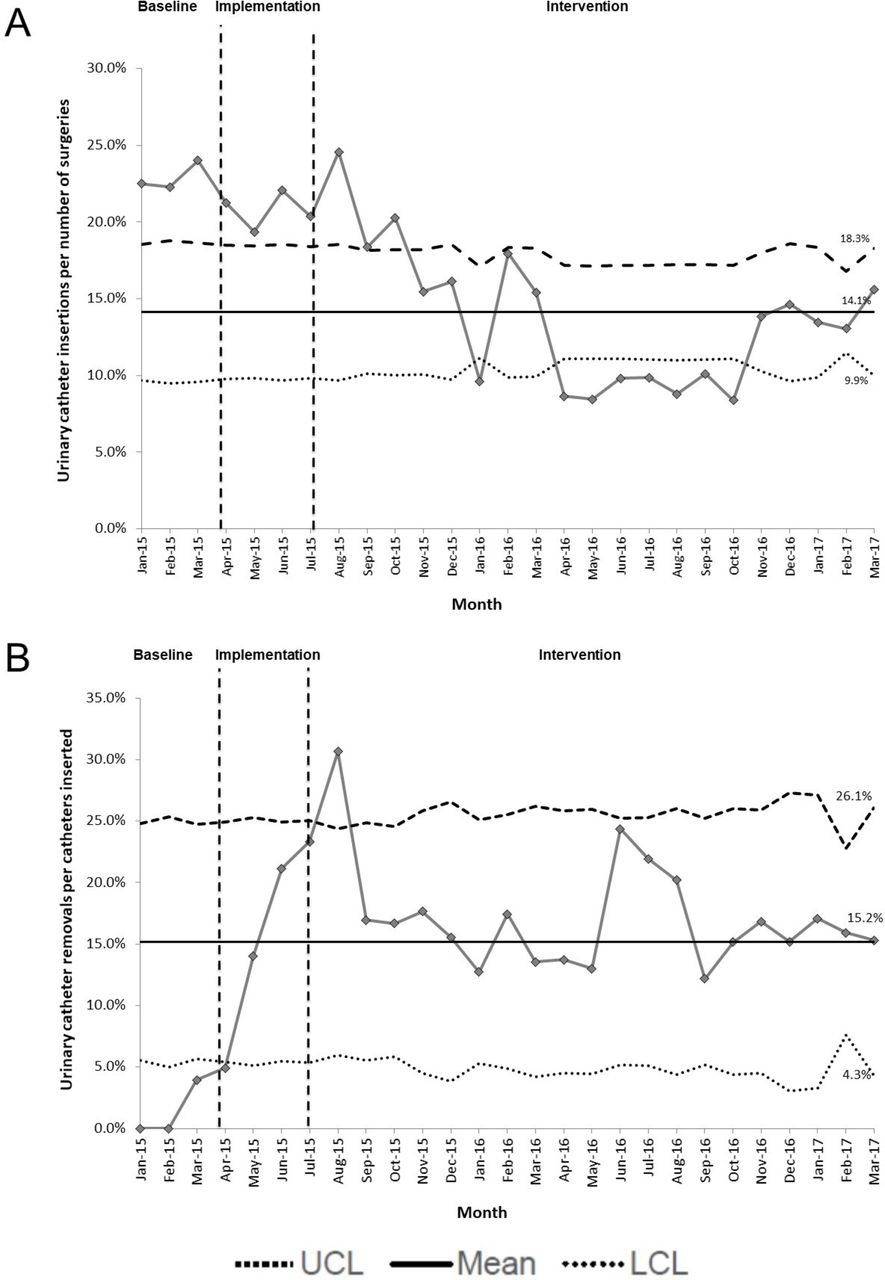
(A) Urinary catheter insertions in the operating room and (B) urinary catheter removals at the end of surgery before and after implementation of a protocol for standardised perioperative catheter use. LCL, lower control limit; UCL, upper control limit.
- Download figure
- Open in new tab
- Download powerpoint
Urinary catheter maintenance on surgical units before and after implementation of medical directive for nurse-initiated postoperative catheter removal. LCL, lower control limit; UCL, upper control limit.
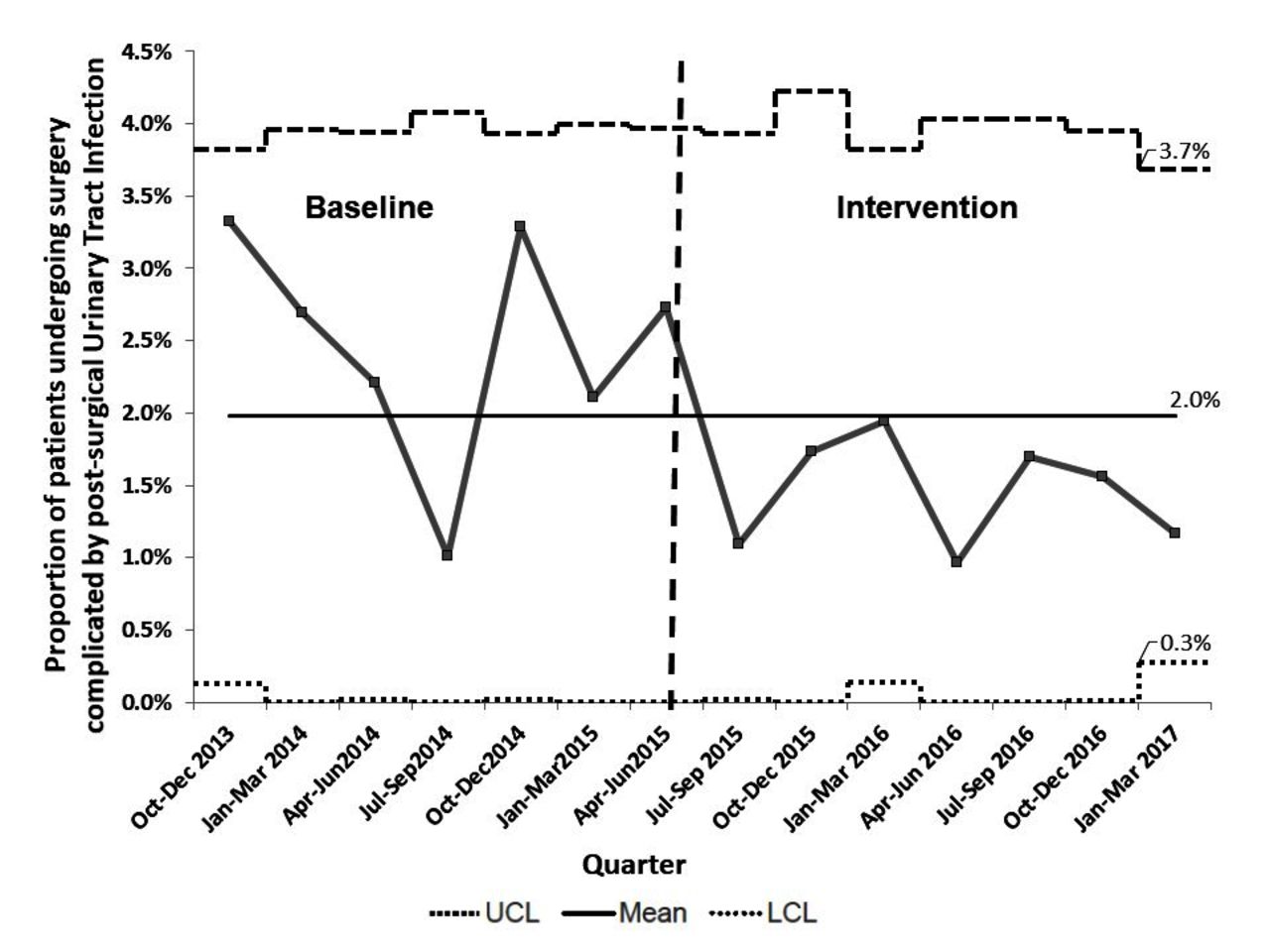
Figure 3 displays quarterly postsurgical UTI rates throughout the study period. The baseline postsurgical UTI rate was 79/3127 (2.5%, 95% CI 2.0% to 3.1%) but decreased significantly during intervention period to 46/3193 (1.4%, 95% CI 1.1% to 1.9%; p=0.002) with a shift below the mean UTI rate. By March 2017, postsurgical UTI reached an annual rate in the third decile compared with peer hospitals of the ACS NSQIP.
{kind=link}
{kind=link}
Postsurgical urinary tract infection rate before and after implementation of standardised perioperative catheter use. LCL, lower control limit; UCL, upper control limit.
Discussion
We implemented a standardised approach to perioperative urinary catheterisation which included limiting intraoperative catheter insertions, ensuring use of sterile technique and promoting routine removal postoperatively. This approach resulted in a significant shift in UC utilisation intraoperatively and postoperatively, which was associated with a measured reduction in postsurgical UTIs, from 10th decile to third decile compared with peer hospitals of the ACS NSQIP.
Over the past 15 years, UTI prevention efforts have intensified across the USA, Canada and Europe with focus on minimising UC use, the main risk factor for healthcare-associated UTI.1 4–6 Despite the improvements seen, the most common approach has been to implement processes that promote daily reassessment of UCs, but few have sought to operationalise ‘appropriateness’ for inserting or maintaining UCs.4 Because guidelines put forward by the CDC in 2009 remain quite broad in regard to the perioperative use of UCs, our experience is that these are frequently left to the discretion of individual surgeons or anaesthetists.
One before-after study performed over a decade ago standardised perioperative catheter use for their orthopaedic surgeries by restricting their use to surgeries lasting over 5 hours or if the patient had advanced age or high American Society of Anesthesiologists class.12 13 Our study involved standardising use of UCs across a large number of surgical services including general surgery, vascular surgery, neurosurgery, orthopaedic surgery and plastic surgery. While these criteria were based on the CDC guidelines, at least four important refinements were made. First, we standardised the anticipated duration of surgery requiring a catheter to 4 hours. Second, we defined the surgeries needing intraoperative monitoring of urinary output as those with significant anticipated fluid shifts or blood loss. Third, we standardised asking the question about whether the catheter can be removed immediately following the case. Finally, we standardised postoperative removal on the morning of postoperative day 2 for all patients not meeting exclusion criteria (Table 1). This pragmatic evaluation across a broad number of surgical services will help refine appropriateness criteria for urinary catheterisation as has been done for medical patients, to promote improved benchmarking and improvement efforts.9 14 15
Standardising perioperative UC practices was also met with specific challenges. The implementation of our new processes occurred over 3 months (April to July 2015) with significant training of operating room and ward staff. Some change in practice was immediately evident starting in April such as removal of UCs at the end of surgery, but it took up to 6 months to see a reduction in the rate of UC insertion as staff became more comfortable operating without a UC in place (figure 1A,B). This example highlights the time needed for socioadaptive changes that follow an implemented technical change.16 On the surgical wards, barriers to avoiding UC placement have already been extensively documented in the literature and we similarly learned the importance of supporting front-line staff with functioning bladder scanners and alternatives to UCs to reduce staff workload.5 17
Our study’s primary outcome was postsurgical UTI as defined through participation in ACS NSQIP. This measure differs from the traditional focus on catheter-associated UTI as it includes all UTIs meeting symptoms consistent with the NHSN definition but limited to those arising within 30 days of an index surgery. This difference reflects the goal of ACS NSQIP which is to improve surgical outcomes. Prior studies have demonstrated that data generated from ACS NSQIP can be used to measure improvements in surgical site infection,18 19 yet there are few published examples demonstrating improvement in postsurgical UTI. With over 560 hospitals across North America participating in ACS NSQIP, our pragmatic study provides evidence that postsurgical UTI is a relevant outcome measure that is responsive to changes in perioperative UC utilisation.
Our study has several important limitations. It was carried out at a single large academic centre where surgical practices may be different from other institutions; however, the standardised perioperative approach to urinary catheterisation was applied to a broad range of surgical procedures. The potential for confounding factors affecting UC use remains but our time series analysis allowed us to distinguish the impact of our intervention from any underlying secular trends. Finally, the use of postsurgical UTI using the methodology put forward by ACS NSQIP as an outcome measure was limited to infections arising within 30 days of surgery and would not have captured hospital-acquired UTIs outside of this time frame.
Standardised perioperative UC practices were fully implemented at our large tertiary care hospital resulting in sustained practice change with a measurable improvement in postsurgical UTI. These appropriateness criteria for perioperative UC use among a broad range of surgical services could inform best practices for hospitals participating in ACS NSQIP.
Acknowledgments
We thank our department of surgery front-line staff and the rest of the team from Sunnybrook’s Infection Prevention and Control team. We also acknowledge the hard work of all patient care managers and advance practice nurses who supported this project.
References
Footnotes
Contributors All authors contributed and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval Sunnybrook Health Sciences Centre Research Ethics Board.
Provenance and peer review Not commissioned; externally peer reviewed.