Article Text

Abstract
Background In-hospital medication review has been linked to improved outcomes after discharge, yet there is little evidence to support the use of community pharmacy-based interventions as part of transitional care.
Objective To determine whether receipt of a postdischarge community pharmacy-based medication reconciliation and adherence review is associated with a reduced risk of death or re-admission.
Design Propensity score-matched cohort study.
Setting Ontario, Canada
Participants Patients over age 66 years discharged home from an acute care hospital from 1 April 2007 to 16 September 2016.
Exposure MedsCheck, a publicly funded medication reconciliation and adherence review provided by community pharmacists.
Main outcome The primary outcome was time to death or re-admission (defined as an emergency department visit or urgent rehospitalisation) up to 30 days. Secondary outcomes were the 30-day count of outpatient physician visits and time to adverse drug event.
Results MedsCheck recipients had a lower risk of 30-day death or re-admission (23.4% vs 23.9%, HR 0.97, 95% CI 0.95 to 1.00, p=0.02), driven by a decreased risk of death (1.7% vs 2.1%, HR 0.79, 95% CI 0.73 to 0.86) and rehospitalisation (11.0% vs 11.4%, HR 0.96, 95% 0.93–0.99). In a post hoc sensitivity analysis with pharmacy random effects added to the propensity score model, these results were substantially attenuated. There was no significant difference in 30-day return to the emergency department (22.5% vs 22.8%, HR 0.99, 95% CI 0.96 to 1.01) or adverse drug events (1.5% vs 1.5%, HR 1.03, 95% CI 0.94 to 1.12). MedsCheck recipients had more outpatient visits (mean 2.11 vs 2.09, RR 1.01, 95% CI 1.00 to 1.02, p=0.02).
Conclusions and relevance Among older adults, receipt of a community pharmacy-based medication reconciliation and adherence review was associated with a small reduced risk of short-term death or re-admission. Due to the possibility of unmeasured confounding, experimental studies are needed to clarify the relationship between postdischarge community pharmacy-based medication review and patient outcomes.
- medication reconciliation
- transitions in care
- medication safety
Statistics from Altmetric.com
Introduction
The period of transition home after hospitalisation presents numerous risks to patients. In addition to reduced functioning, patients may experience a clinical deterioration or complications from treatment. Medications are the most frequent cause of postdischarge adverse events, with medication-related events occurring after 13%–16% of hospital admissions.1–3 This rate reflects errors in discharge medication lists, inappropriate prescribing, inadequate understanding of medication changes and insufficient monitoring.3–5 In some cases, medication-related adverse events lead to costly hospital re-admissions.6
Medication safety is a pillar of optimal discharge practices, and appears in multiple checklists.7–9 Medication-related interventions are frequently included in multicomponent transitional care interventions, many of which have reduced all-cause hospital re-admissions.10 In Canada, medication review at discharge is a hospital accreditation standard.11 Yet, studies investigating the effect of medication reconciliation alone have yielded inconsistent results.12 Medication reconciliation by in-hospital pharmacists has been found to reduce potential medication errors and drug-related re-admissions, but not all-cause re-admissions.13 14 In a recent systematic review, medication reconciliation delivered on the phone or in a clinic setting by community-based pharmacists did not reduce the subsequent rate of re-admission.15 Other systematic reviews examining medication review by pharmacists in any community setting (ie, primary care, in the home or in pharmacy) found mixed effects on medication adherence, clinical symptom improvement and healthcare resource utilisation, highlighting the challenge in understanding the effectiveness of a general medication review conducted in a community setting.16–18
In 2007, the Ontario Ministry of Health and Long-Term Care introduced MedsCheck, a programme of medication reconciliation and adherence review by community pharmacists.19 Patients presenting to pharmacy were eligible for a MedsCheck if they were receiving at least three chronic medications.20 The effect of MedsCheck on outcomes after hospital discharge has not been studied. Our objective was to determine if patients receiving MedsCheck after hospital discharge have lower rates of subsequent death or re-admission than eligible patients not receiving a MedsCheck assessment.
Methods
Setting, design and data sources
We conducted a retrospective propensity score-matched cohort study of patients discharged home from an Ontario hospital between 1 April 2007 and 16 September 2016. ICES houses de-identified linked health administrative data for all Ontario residents who have a valid provincial health insurance card. This includes information on demographics,21 hospitalisations,22 emergency department visits,23 outpatient visits,24 home care and time of death.25 The Ontario Drug Benefit database includes information on medications and professional pharmacy services (including MedsCheck) provided to low-income patients and those over age 65 years.26 As provincial health insurance is granted universally to all citizens and permanent residents, this study is population-based.
Study population
We included patients who were ≥66 years of age at discharge, were eligible for MedsCheck and filled a prescription at a community pharmacy within 7 days of discharge. Eligibility was defined, consistent with criteria for MedsCheck reimbursement, as taking three or more chronic medications over the previous 6-month period.27 MedsCheck programme documentation did not define ‘chronic medications’, however we adopted a previously used definition (online supplementary eTable 1).19 28 The 7-day window for the prescription fill was selected to capture medication changes resulting from hospitalisation.29
Supplemental material
We restricted the analysis to patients who were discharged to the community, excluding discharges or transfers to nursing homes, rehabilitation or other healthcare institutions. We also excluded three groups likely to have markedly different re-admission risk: newborns, patients admitted for an obstetrical delivery or those receiving palliative care (online supplementary eFigure 1).
The MedsCheck eligibility date was the earliest date at which an eligible patient filled a prescription in a community pharmacy. To ensure comparability of groups, we excluded patients who experienced an outcome or MedsCheck prior to their MedsCheck eligibility date. We also excluded patients with a missing age, sex, invalid home location or invalid death date. We selected each patient’s first hospital discharge during the study period, and excluded all others.
Exposure
The MedsCheck service was offered by a community pharmacist in a pharmacy or home setting. Programme guidelines for MedsCheck during the time of our study described it as a ‘one-on-one interview between the pharmacist and the patient to review the patient’s prescription and non-prescription medications’ and that it is expected to last approximately 20–30 min.27 In addition to taking at least three chronic medications, requirements for the service include: (1) Agreement by the patient. (2) One-on-one interview in an acoustically private area. (3) Provision to the patient of a complete list of prescription and non-prescription medications.27 Pharmacists may or may not have access to the hospital discharge medication list as this is typically provided in paper form by the patient. Follow-up on medication discrepancies or any other drug therapy problem is at the discretion of the pharmacist.
There are several MedsCheck billing codes, each corresponding to a specific patient population (online supplementary eTable 2). As an example, MedsCheck Annual can be done once yearly ($60), and MedsCheck follow-up ($25) can be provided at any time for any of the following indications: (1) Hospital discharge in the previous 2 weeks. (2) Before a planned hospital admission. (3) Physician referral. (4) Pharmacist decision based on previous non-adherence, medication changes or a change of pharmacy (online supplementary eTable 2).30 Pharmacists are not compelled to provide the service to all qualified patients, but can offer the service to eligible patients at their discretion.
The exposure in our study was receipt of any MedsCheck service. We allowed for MedsCheck to occur up to 14 days following hospital discharge.30
Other variables
We included patient, hospital and pharmacy-level variables which were likely to be associated with receipt of MedsCheck or an outcome.28 These included patient demographics, comorbidities, measures of previous healthcare usage (including receipt of MedsCheck in the previous year), hospital and hospitalisation characteristics (including year of discharge). Medication usage variables included the total number of medications and history of potentially inappropriate or high-risk medications in the previous year. Potentially inappropriate medications were as identified in the 2012 and 2015 Beer’s lists.31 32 High-risk medications were the drugs most frequently implicated in adverse drug events (online supplementary eTable 3).33–35 We also included the number of new medications filled postdischarge, as well as a whether a new high-risk medication or potentially inappropriate medication was dispensed. We categorised into quartiles each pharmacy’s ratio of annual MedsCheck volume to total volume, to account for differences in MedsCheck delivery patterns between pharmacies. Observations with missing information for categorical variables were included in the analysis by creating an additional variable level to explicitly denote missingness.
Main outcome measures
The primary outcome was time to death or re-admission. We defined re-admission as inclusive of both unscheduled emergency department visits and urgent rehospitalisations. The date of death was obtained from the Registered Persons Database, which captures over 98% of Ontario deaths.25 The date of re-admission was obtained from the Discharge Abstract Database (DAD), and has been found to be 99.9% accurate when compared with chart abstraction.22 The date of emergency department visit was obtained from the National Ambulatory Care Reporting System. This field is 100% complete and has not been previously validated. It can be expected to have similar accuracy to the date of admission in the DAD, since both are entered by the same trained hospital coders.
Secondary outcomes were time to adverse drug event requiring emergency department visit or hospitalisation (based on International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Canada (ICD-10-CA) codes, online supplementary eTables 4 and 5)34 36 37 and the count of outpatient physician visits. All outcomes were measured to 30 days after MedsCheck receipt.
Subgroups
We prespecified three subgroups at potentially higher risk for re-admission,38 and for whom a MedsCheck might be beneficial due to a higher risk of adverse drug events:34 36 37 (1) Patients with an admitting diagnosis of heart failure, (2) Patients with an admitting diagnosis of chronic obstructive pulmonary disease (COPD), (3) Patients filling a prescription for a new high-risk medication (online supplementary eTable 3). An additional subgroup analysis was undertaken in response to reviewer comments: we compared the outcomes of early MedsCheck recipients and controls (time from discharge ≤2 days) to the outcomes of late recipients and controls (>2 days).
Analysis
Patient, hospital and pharmacy characteristics of those receiving and not receiving a MedsCheck were compared using descriptive statistics. Comparisons were made using standardised differences, with differences of 10% or greater considered to be meaningful.39 40 MedsCheck recipients were matched 1:1 to eligible controls based on the logit of the propensity score and hard matching on subgroup variables. Further details are available in the appendix (online supplementary eFigure 2).
We estimated Kaplan-Meier survival curves for the primary composite outcome and death. We plotted cumulative incidence function curves for return to the emergency department and for urgent rehospitalisation, to account for the competing risk of death. We reported HRs (with 95% CIs) for all time-to-event outcomes, obtained from a Cox proportional hazards model estimated in the matched sample. The hazard of the outcome was regressed on a single variable (exposure to MedsCheck). A robust variance estimator was used to account for the paired nature of the data.41 Due to the competing risk of death, we reported cause-specific HRs for the outcomes of return to the emergency department, urgent rehospitalisation and adverse drug events.42
Comparison of the 30-day count of outpatient visits was made using a negative binomial model with generalised estimating equations to account for clustering of data within matched pairs. We reported the risk ratio and 95% CIs. We used a standard Z-test for the equality of the MedsCheck programme between those filling a new high-risk medication and those not filling a new high-risk medication. We similarly tested the equality of the effect of late receipt of MedsCheck (vs no MedsCheck) and the effect of early receipt of MedsCheck (vs no MedsCheck).
Significance was defined as p<0.05 and all hypothesis testing was two-tailed. All analyses were performed in SAS software, V.9.4 (SAS Institute, Cary, North Carolina, USA).
Sensitivity analysis
In response to editor feedback, we re-analysed all outcomes using a modified strategy. We incorporated pharmacy-specific random effects into the propensity score model, which effectively brought the propensity scores of patients presenting to the same pharmacy closer together. We then matched MedsCheck recipients and controls using the same approach as in our main analysis. Due to residual imbalance between matched groups on the proportion of patients filling their prescription at a high MedsCheck volume pharmacy, this variable was added as an additional hard-matching criterion.
Results
We identified 1840 288 discharges eligible for MedsCheck. Among these, 29 763 (1.6%) were excluded due to a prior outcome, and 2748 (0.1%) were excluded because of MedsCheck receipt after discharge but prior to their eligibility date (online supplementary eFigure 1). Patients excluded in each step were compared with the remaining patients in eTables 6 and 7. From the remaining 1807 777 hospital discharges, we selected the first discharge per patient, resulting in a sample of 879 497 patients. Of these, 77 459 (8.8%) received a MedsCheck within 14 days of hospital discharge. Before propensity score matching, patients receiving a MedsCheck differed from those not receiving a MedsCheck (online supplementary eTable 8). The greatest differences were in the median year of discharge (MedsCheck 2013 vs 2011, Std Diff 66%), the proportion with a Charlson Score of 0 (MedsCheck 27.8% vs 38.3%, Std Diff 22%), the proportion admitted electively (MedsCheck 15.9% vs 30.1%, Std Diff 34%), and the median length of hospital stay (MedsCheck 5 days vs 4 days, Std Diff 28%).
Characteristics of propensity score-matched cohort
Of patients receiving MedsCheck, 87% (n=67 163) were successfully matched to a control subject. Unmatched MedsCheck recipients are compared with matched MedsCheck recipients in online supplementary eTable 9. Matched MedsCheck recipients were similar in terms of all covariates to matched controls, with no standardised difference exceeding 10% (table 1). The greatest difference was in the proportion of patients filling their prescription at a pharmacy in the highest MedsCheck quartile (MedsCheck 42.6% vs 39.1%, Std Diff 7%).
Comparison of characteristics of MedsCheck recipients and matched controls
Outcomes
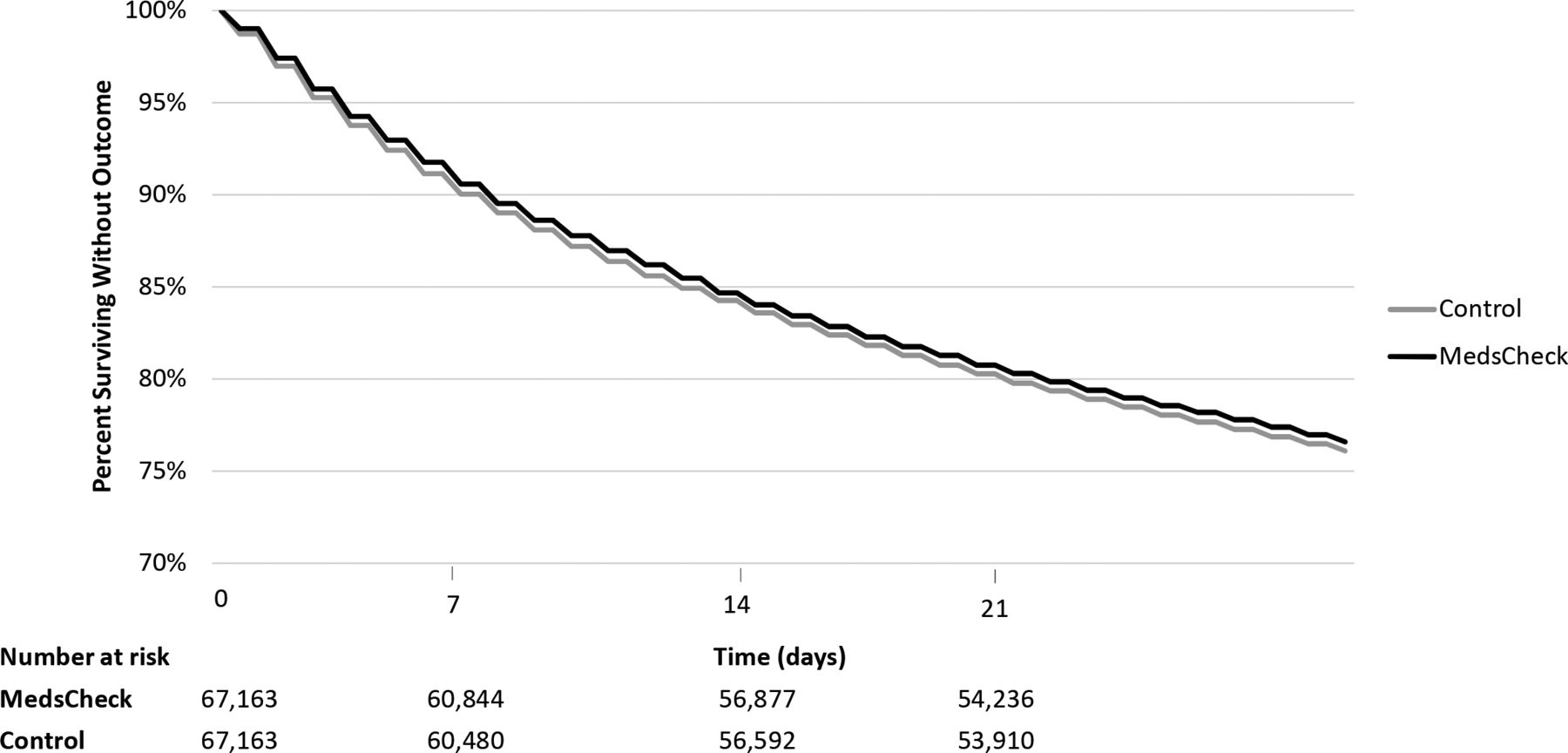
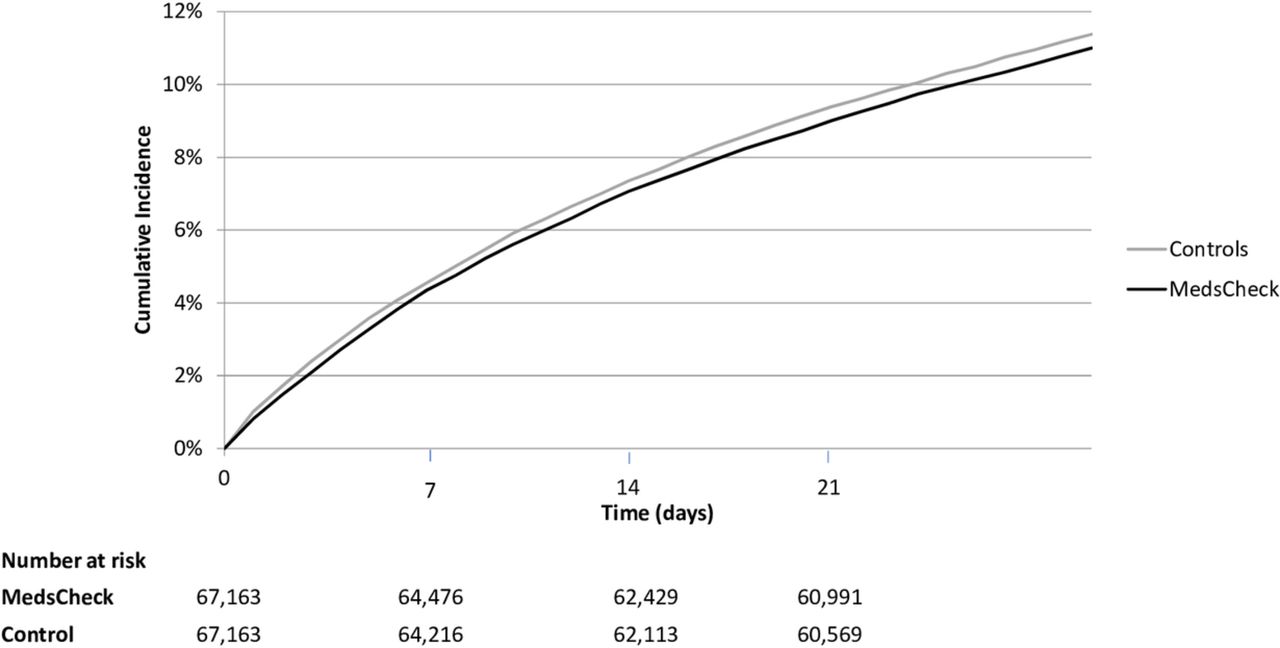
Those who received a MedsCheck after hospital discharge were less likely to experience death or re-admission within 30 days (23.4% vs 23.9%, HR 0.97, 95% CI 0.95 to 1.00, p=0.02, table 2 and figure 1). This was explained by a decreased risk of death (1.7% vs 2.1%, HR 0.79, 95% CI 0.73 to 0.86, figure 2) and rehospitalisation (11.0% vs 11.4%, HR 0.96, 95% CI 0.93 to 0.99, figure 3). We found no statistically significant difference in return to the emergency department (22.5% vs 22.8%, HR 0.99, 95% CI 0.96 to 1.01, online supplementary eFigure 3).
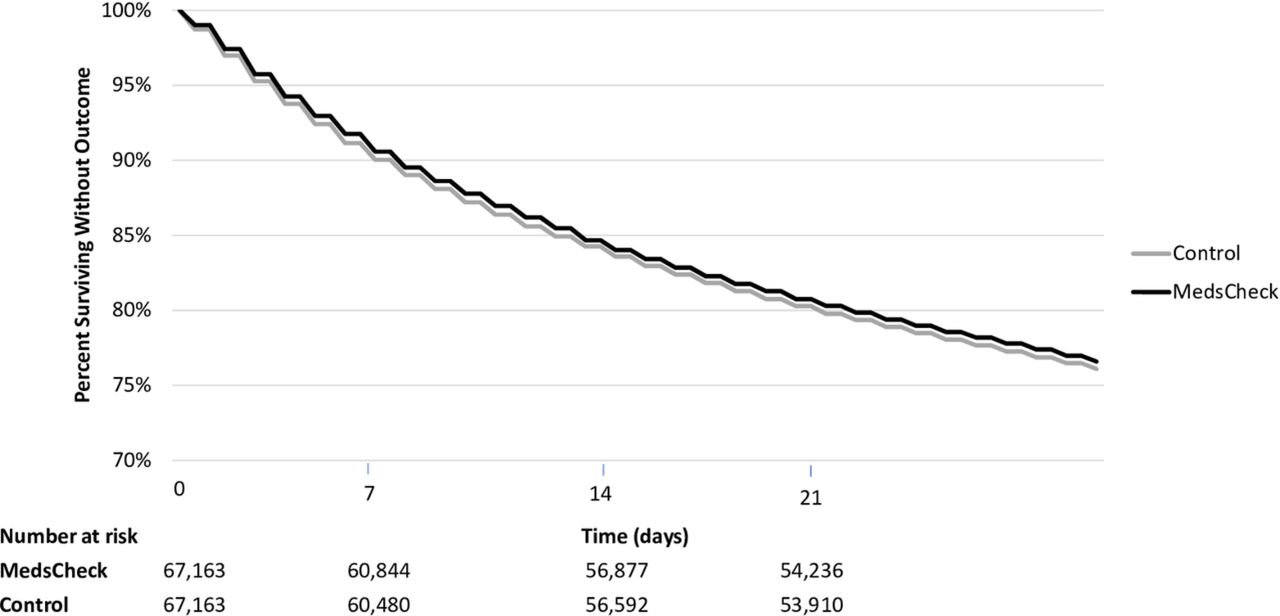
Kaplan-Meier curve of time to death or re-admission. Note: y-axis has been truncated for better visualisation.
Kaplan-Meier curve of time to death. Note: y-axis has been truncated for better visualisation.

{kind=link}
{kind=link}
{kind=link}
Cumulative incidence curve of time to urgent rehospitalisation.
Comparison of outcomes in the matched sample at 30 days, for all patients and subgroups
There was no difference in adverse drug events associated with MedsCheck status (1.5% vs 1.5%, HR 1.03, 95% CI 0.94 to 1.12). MedsCheck recipients had more outpatient visits than matched controls (mean 2.11 vs 2.09, RR 1.01, 95% CI 1.00 to 1.02, p=0.02).
Subgroup analyses
Heart failure
Among the 8420 (6.3%) patients hospitalised for heart failure, MedsCheck was not associated with any reduction in the composite outcome (MedsCheck 25.5% vs 27.2%, HR 0.93, 95% CI 0.85 to 1.01, table 2). However MedsCheck was associated with a reduced likelihood of death at 30 days (MedsCheck 2.1% vs 3.2%, HR 0.65, 95% CI 0.49 to 0.85). There was no difference in rehospitalisation (MedsCheck 14.9% vs 15.5%, HR 0.95, 95% CI 0.86 to 1.07) or emergency department visits (MedsCheck 24.5% vs 25.7%, HR 0.95, 95 % CI 0.87 to 1.03).
Among patients admitted for heart failure, there was no difference in the risk of adverse drug events between patients according to MedsCheck status (MedsCheck 2.1% vs 1.7%, HR 1.24, 95% CI 0.91 to 1.69). MedsCheck recipients had more outpatient visits than controls (mean MedsCheck 2.27 vs 2.18, RR 1.04, 95% CI 1.00 to 1.07, p=0.03).
Chronic obstructive pulmonary disease
Among the 6168 (4.6%) patients hospitalised for COPD, there was no association between receipt of MedsCheck and the primary outcome of death or re-admission (MedsCheck 22.3% vs 21.7%, HR 1.03, 95% CI 0.92 to 1.14) or any of the subcomponents of death (2.0% vs 1.9%, HR 1.05, 95% CI 0.74 to 1.50), rehospitalisation (13.0% vs 12.3%, HR 1.06, 95% CI 0.92 to 1.22) or emergency department visit (21.9% vs 20.9%, HR 1.05, 95% CI 0.94 to 1.17). There was no difference in the risk of adverse drug events between patients who did or did not receive a MedsCheck (MedsCheck 1.2% vs controls 1.3%, HR 0.88, 95% CI 0.56 to 1.38). MedsCheck recipients had more outpatient visits than did controls (mean 1.78 vs 1.62, RR 1.10, 95% CI 1.05 to 1.14).
New high-risk medication
A total of 83 584 (62.2%) patients filled a prescription for a new high-risk medication after discharge. Among those patients who filled a new high-risk medication, MedsCheck recipients had a lower rate of death or re-admission (MedsCheck 24.1% vs 25.2%, HR 0.95, 95% CI 0.92 to 0.97, table 2). This was not the case for those who did not fill a new high-risk medication (MedsCheck 22.3% vs 21.7%, HR 1.03, 95% CI 0.99 to 1.07, p for interaction=0.0004, online supplementary eTable 10) . Among those who filled a new high-risk medication, MedsCheck recipients were at reduced risk of each of emergency department visit (MedsCheck 23.2% vs 24.0%, HR 0.96, 95% CI 0.93 to 0.98, p for interaction=0.0006), rehospitalisation (MedsCheck 11.1% vs 11.9%, HR 0.93, 95% CI 0.90 to 0.97, p for interaction=0.01) and death (MedsCheck 1.8% vs 2.3%, HR 0.78, 95% CI 0.71 to 0.86, p for interaction=0.57).
Among patients filling a new prescription for a high-risk medication, we found no difference in adverse drug events between patients who did or did not receive a MedsCheck (1.7% vs controls 1.6%, HR 1.06, 95% CI 0.95 to 1.18, p for interaction=0.34). There was no difference in the count of outpatient visits between MedsCheck recipients and controls (median 2.17 vs 2.15, RR 1.01, 95% CI 1.00 to 1.02, p=0.27, p for interaction=0.32).
Early or late receipt of MedsCheck
Among MedsCheck recipients, 51 575 (76.8%) received the intervention early, that is within 2 days of discharge. Compared with later recipients and controls, early recipients and controls had fewer comorbidities, longer length of stay, were more likely to be diagnosed with a circulatory condition or symptoms not otherwise specified, had fewer previous outpatient physician visits and medications, but more new medications and new high-risk medications (online supplementary eTable 11).
Early MedsCheck recipients were at reduced risk of death or re-admission (24.5% vs 25.3%, HR 0.96, 95% CI 0.94 to 0.98, online supplementary eTable 12), unlike late recipients (19.9% vs 19.3%, HR 1.04, 95% CI 0.99 to 1.09, online supplementary eTable 13, p for interaction=0.007). Early recipients were at reduced risk of return to the emergency department (23.6% vs 24.1%, HR 0.97, 95% CI 0.95 to 0.99), whereas late recipients were at increased risk of return to the emergency department (19.1% vs 18.2%, HR 1.05, 95% CI 1.00 to 1.05, p for interaction=0.005). Late recipients were also more likely than early recipients to have a MedsCheck-associated increase in outpatient physician visits (Early RR 1.00, 95% CI 0.99 to 1.01, Late RR 1.03, 95% CI 1.01 to 1.05, p for interaction=0.016).
Sensitivity analysis: pharmacy random-effects model
Incorporating pharmacy-level random effects into the propensity score model modified our results in several ways. We successfully matched 1: 1 63 207 (82%) MedsCheck recipients to controls. MedsCheck receipt was no longer associated with a decreased rate of the composite outcome of death or re-admission (HR 0.99, 95% CI 0.96 to 1.01) or a decrease in rehospitalisation (HR 0.97, 95% CI 0.94 to 1.01), however, it was still associated with a decreased rate of death alone (HR 0.82, 95% CI 0.75 to 0.89). There was no change in the results for adverse drug events or outpatient physician visits (online supplementary eTable 14).
Discussion
Among eligible older patients filling a prescription after discharge from hospital, receipt of MedsCheck was associated with a small decrease in the rate of death or re-admission over 30 days, driven by decreases in the rate of death and rehospitalisation. Patients admitted for heart failure had a decreased rate of death if they received a MedsCheck, though there was no difference in re-admission. There was no difference in death or re-admission for patients with COPD. Patients filling a prescription for a new high-risk medication had a decreased rate of death or re-admission if they received a MedsCheck, driven by an increased rate of all three subcomponents: emergency department visits, rehospitalisation and death. MedsCheck received within 2 days of discharge was associated with a decrease in the risk of death or re-admission. Receipt of MedsCheck was also associated with a small increase in outpatient physician visits in the whole cohort, as well as for the heart failure, COPD and late presentation subgroups.
The low rates of MedsCheck (9%) for eligible patients in our study suggests that there may be challenges with current programme implementation.43 In addition, low rates of MedsCheck suggest that recipients may be highly selected.28 We could not distinguish which patients declined to receive a MedsCheck and which were simply not offered the service despite being eligible. Furthermore, we have no data on how much the variation in MedsCheck delivery relates to these factors. Although we accounted for differences in baseline healthcare usage, MedsCheck recipients might be more likely to seek care or engage in self-management. The increased rate of outpatient visits in MedsCheck recipients is consistent with this explanation. It is also possible that receipt of MedsCheck triggers outpatient visits to follow-up on identified medication-related issues.
We noted that late MedsCheck was associated with increased physician and emergency department visit but no reduction in death or re-admission, unlike early receipt of MedsCheck. It is possible that early MedsCheck is more effective at preventing adverse medication events, and that late MedsCheck triggers increased visits as adverse events are detected. Alternatively, late-presenting patients may be sicker, and more likely to experience a worse outcome regardless of MedsCheck receipt.
Postdischarge medication review has been included as one component of several bundled transitional care interventions. Such multifaceted interventions have led to reductions in re-admission rates.9 44 45 However, a recent systematic review reported that community-based medication reconciliation interventions did not on their own reduce the risk of re-admission after hospital discharge.15 Included interventions were mainly delivered by phone or in outpatient clinics. The only study conducted in a community pharmacy setting did not report re-admission rates.46 We identified one additional study conducted in a community pharmacy that reported a reduction in re-admissions (adjusted OR 0.07, 95% CI 0.01 to 0.63) for patients choosing medication review instead of usual care.47 These results were likely affected by immortal time bias since the outcome was measured from discharge, not from the time of intervention.
How MedsCheck might reduce the risk of death is uncertain. We found that patients filling a new high-risk medication did better if they received a MedsCheck, despite no corresponding difference in adverse drug events. One explanation may be that adverse drug event hospitalisation or emergency department visit codes are specific yet insensitive for medication-related complications. Consistent with this, the overall rate of adverse drug events in our study was considerably lower than reported in chart review-based studies.1 2 6 When directly measured, others have found that transitional care interventions can reduce adverse drug events.48 MedsCheck may also improve adherence, resulting in increased clinical stability. That a benefit was observed in the subgroup with heart failure but not those with COPD could point to differences in the effect of medications on each condition’s disease trajectory.
Our study was population-based and benefited from multiple linked health administrative databases. As a result, we were able to account for differences in sociodemographic characteristics, previous healthcare usage, hospitalisation and pharmacy characteristics, as well as medication usage profiles. We included several variables to account for factors affecting the likelihood of receiving a MedsCheck. This included history of dementia, language ability and markers of decreased mobility (use of home care and physician home visits). We also accounted for discharge year since MedsCheck use has increased over time.19 To minimise immortal time bias, we carefully aligned follow-up periods between recipients and controls. To ensure comparability of patient groups, we limited our selection criteria to patients over age 66 years who would be eligible for MedsCheck. The age criterion was necessary to obtain medication histories for the year prior to hospital discharge as medication data are incomplete for other age groups. Our study findings are thus limited to elders, and MedsCheck may have different associations in younger patients.
While our propensity score-matched design accounted for differences in previous healthcare usage, residual confounding remains possible. In particular, our findings of a moderate decrease in mortality with no difference in emergency department visits suggests that recipients may differ from controls in ways not measured here. For example, reduced mobility after discharge may prevent sicker patients from in-person pharmacy attendance. While a caregiver can receive medications on a patient’s behalf, MedsCheck can only be provided to a caregiver with patient consent. Further, a clinically deteriorating or frail patient may have a caregiver pick up medications and be unlikely to present in-person for a MedsCheck. Incorporating pharmacy-level random effects into the propensity score led to a dampening of several small associations. This change could relate to reduced sample size or to accounting for variation related to neighbourhood or pharmacy-level practices. Nonetheless, it suggests uncertainty about the magnitude and significance of MedsCheck-related benefit. The potentially modest benefits contrast with the scale and intensity of this intervention, suggesting a need to modify MedsCheck to enhance its impact. One possible strategy may be to focus on high-risk groups, such as those filling a new high-risk medication after discharge.
We did not include outcomes related to medication adherence. In Ontario, 90-day medication dispensation necessitates a longer follow-up period to measure drug adherence. This is further complicated by medication discontinuity occurring around the time of hospitalisation. As the health administrative databases do not contain information on in-hospital medications, we could not detect postdischarge primary non-adherence.29 Comparing long-term adherence to medications initiated during hospitalisation is an area for future research. In addition, MedsCheck is provided throughout Ontario in community pharmacies of all types. As a result, delivery likely varies across locations and providers, with local practices contributing to any potential effect of MedsCheck on recipients. Further, our findings may not be generalisable to other jurisdictions where pharmacist payment models and practice organisation differ significantly from the Ontario context.
In this study of patients filling a prescription after hospital discharge, receiving a community pharmacy medication review was associated with a small reduction in 30-day death or re-admission. Despite this, patients receiving MedsCheck were no less likely to return to hospital for an adverse drug event. In the subgroup of patients filling a prescription for a new high-risk medication, MedsCheck was associated with fewer emergency department visits, hospitalisations and deaths. Since selection for MedsCheck depends on both pharmacist initiative and patient willingness, our findings remain limited by the possibility of residual confounding, as evidenced by dampening of all observed associations in sensitivity analysis. There is a need for randomised studies to evaluate the benefit of community pharmacist-delivered medication review on postdischarge outcomes, including medication adherence.
References
Footnotes
Twitter @LapointeShaw
Correction notice This article has been corrected since it published Online First.
Contributors Study contributors: All authors had full access to all of the data (including statistical reports and tables) in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study guarantor: LL-S. Study concept and design: all authors. Analysis and interpretation of data: LL-S, PL. Drafting of the manuscript: LL-S. Critical revision of the manuscript for important intellectual content: all authors. Statistical analysis: LL-S, PL. Obtained funding: CMB, LD. Study supervision: LD.
Funding This study was funded by Open Pharmacy Evidence Network, Canadian Patient Safety Institute, Ontario Ministry of Health and Long-Term Care, Canadian Institutes of Health Research. This work was also supported by ICES, which is funded by annual grants from the Ontario Ministry of Health and Long-Term Care (MOHLTC). The opinions, results and conclusions reported in this paper are those of the authors and are independent from the funding sources.
Competing interests LL-S reports support from a CIHR Fellowship Award (FRN 146714), and the Philipson Scholar program at the University of Toronto. PCA is supported by a Mid-Career Investigator award from the Heart and Stroke Foundation. NMI reports support from CIHR and the Ontario Ministry of Health and Long-Term Care. DAR reports support from a Canada Research Chair in Medical Decision Science. CMB reports support from the Department of Medicine at the University of Toronto and Sinai Health System. None of these organisations had any involvement in the design and conduct of the study; collection, management, analysis and interpretation of the data; preparation, review or approval of the manuscript; and decision to submit the manuscript for publication. Parts of this material are based on data and information compiled and provided by the Canadian Institute for Health Information (CIHI) and Immigration, Refugees and Citizenship Canada (IRCC). However, the analyses, conclusions, opinions and statements expressed herein are those of the authors, and not necessarily those of ICES, MOHLTC, CIHI or the IRCC. No endorsement by ICES, MOHLTC, CIHI or the IRCC is intended or should be inferred. The named organisations and funding bodies had no involvement in the design and conduct of the study; collection, management, analysis and interpretation of the data; preparation, review or approval of the manuscript; and decision to submit the manuscript for publication.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available.