Article Text

Abstract
Background Quality improvement (QI) efforts have become widespread in healthcare, however there is significant variability in their success. Differences in context are thought to be responsible for some of the variability seen.
Objective To develop a conceptual model that can be used by organisations and QI researchers to understand and optimise contextual factors affecting the success of a QI project.
Methods 10 QI experts were provided with the results of a systematic literature review and then participated in two rounds of opinion gathering to identify and define important contextual factors. The experts subsequently met in person to identify relationships among factors and to begin to build the model.
Results The Model for Understanding Success in Quality (MUSIQ) is organised based on the level of the healthcare system and identifies 25 contextual factors likely to influence QI success. Contextual factors within microsystems and those related to the QI team are hypothesised to directly shape QI success, whereas factors within the organisation and external environment are believed to influence success indirectly.
Conclusions The MUSIQ framework has the potential to guide the application of QI methods in healthcare and focus research. The specificity of MUSIQ and the explicit delineation of relationships among factors allows a deeper understanding of the mechanism of action by which context influences QI success. MUSIQ also provides a foundation to support further studies to test and refine the theory and advance the field of QI science.
- Quality improvement
- quality assurance
- healthcare
- context
- models
- organisational
- continuous quality improvement
- collaborative
- quality of care
- healthcare quality
- healthcare quality improvement
- breakthrough groups
- control charts
- run charts
- implementation science
Statistics from Altmetric.com
- Quality improvement
- quality assurance
- healthcare
- context
- models
- organisational
- continuous quality improvement
- collaborative
- quality of care
- healthcare quality
- healthcare quality improvement
- breakthrough groups
- control charts
- run charts
- implementation science
Introduction
The use of quality improvement (QI) methods in healthcare is now widespread. Some QI initiatives have documented significant improvements in processes or patient outcomes,1 some have shown only modest improvements,2 3 and others have failed to show any improvement at all.4 This variation in success has led to scepticism about the effectiveness of QI methods when applied in healthcare settings.5 An alternative explanation for the mixed success of QI in healthcare may be the effects of context on the successful application of QI methods, not the efficacy of the methods themselves. To deal with this problem requires a shift in focus from studies examining whether QI methods work to studies aimed at understanding why, when, and where they work most effectively.6
Context includes characteristics of the organisational setting, the environment, the individual, and their role in the organisation or QI project.7 Contextual factors are distinct from the technical QI process (eg, the QI methods themselves and the clinical interventions).8 Just as the nature of the specific disease and the characteristics of individual patients matter when examining the efficacy of interventions in clinical medicine, the features of the providers and organisations involved in QI initiatives matter when assessing their effectiveness.6 Contextual features (eg, local circumstances, resources, training, motivation, skill, etc.) of the providers participating in QI and the organisations where QI takes place must be considered when studying QI.9
In order to make progress in understanding the role of context in the evaluation and execution of QI efforts, explicit conceptual models, frameworks, and taxonomies are needed to focus and align research and to help practitioners learn how to manage key contextual factors that influence QI success.9–12 A logic model that outlines the mechanism of action by which contextual factors affect QI outcomes is an important element of assessing and improving QI effectiveness12 and the goal of this study was to develop such a model. Using knowledge gained from a systematic review of the literature13 and engagement from a panel of QI experts, the aim of this study was to develop a practical, comprehensive conceptual model for organisations and QI researchers to employ in describing, evaluating and optimising contextual factors that impact a QI project's likelihood of success.
Methods
To develop the Model for Understanding Success in Quality (MUSIQ), a panel of 10 QI experts was convened, including researchers and practical improvers, as well as experts from healthcare and other industries. The members of the expert panel are listed in online appendix S1.
At the beginning of the project, panelists were oriented to the goals of the model development process, including (1) developing a product that would be useful to both QI practitioners and researchers, (2) creating a model with the expectation that it would be tested and further improved, (3) using a level of abstraction that allowed for enumeration of most of the key factors while limiting respondent burden when the model was tested in real world settings, (4) illustrating how contextual factors influence the success of individual QI projects across a single or multiple healthcare microsystems, and (5) creating a model that is applicable to a broad range of QI approaches.14 Panellists were instructed to think about contextual factors operating across all levels of the healthcare system (eg, external environment, macrosystem, microsystem).15 Measurement of context or how to test the validity of the final model was not a specific requirement of the committee.
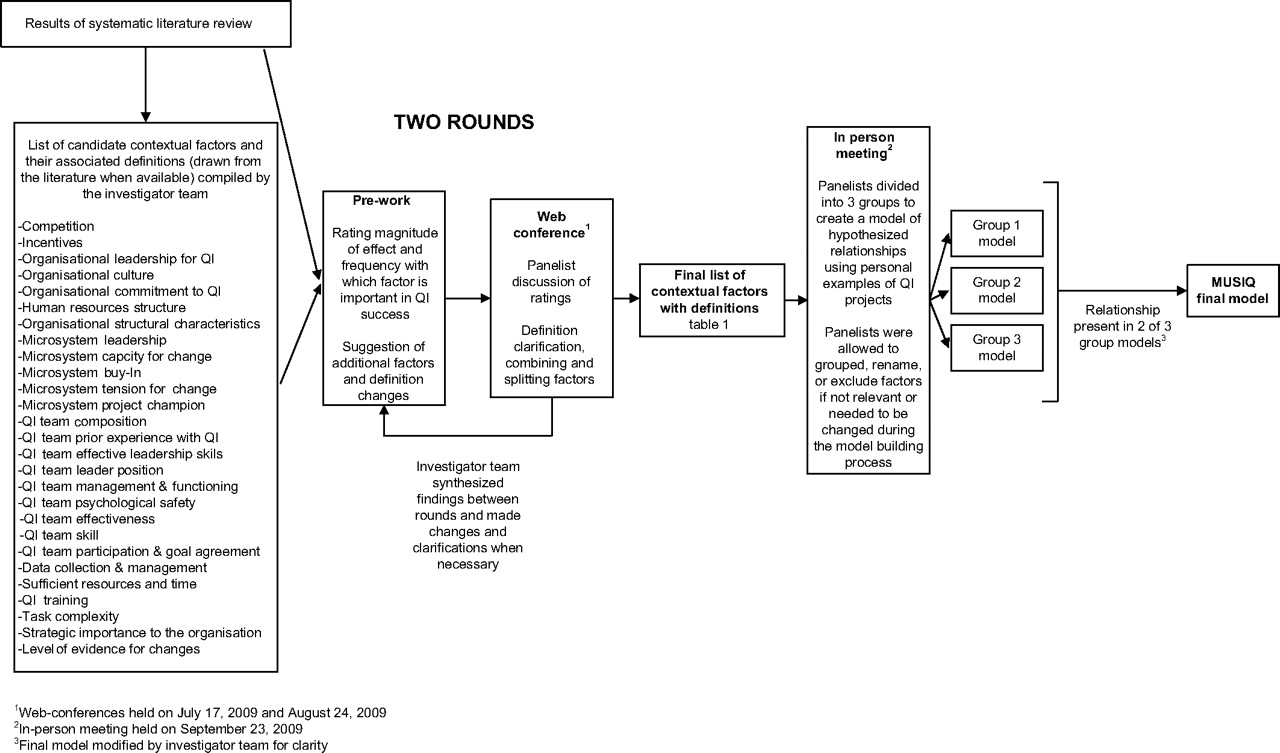
Figure 1 summarises the model development process. Adaptations of the modified Delphi process and nominal group techniques were used to accomplish this goal.16–18 Panellists met three times: twice via web conference and once in person. Meetings were facilitated by an experienced consultant with QI expertise who was not a member of the research team. The goal of the web conferences and associated preparatory work was to identify key elements of context that expert panellists believed were important in QI success and to agree upon working definitions of these elements. Before the first meeting, panellists were provided with a list of candidate contextual factors and associated definitions (taken from the literature, when available). This list was developed by the investigator team via a systematic review of the literature specifically undertaken to support the model development13 as well as from the investigators' own personal QI experiences. Panellists were also provided with summary data from 93 studies examining the role of context in QI success in both healthcare13 and industry. Throughout the model development process, contextual factors were organised based on the level at which they were believed to operate (eg, environment, macrosystem, microsystem).
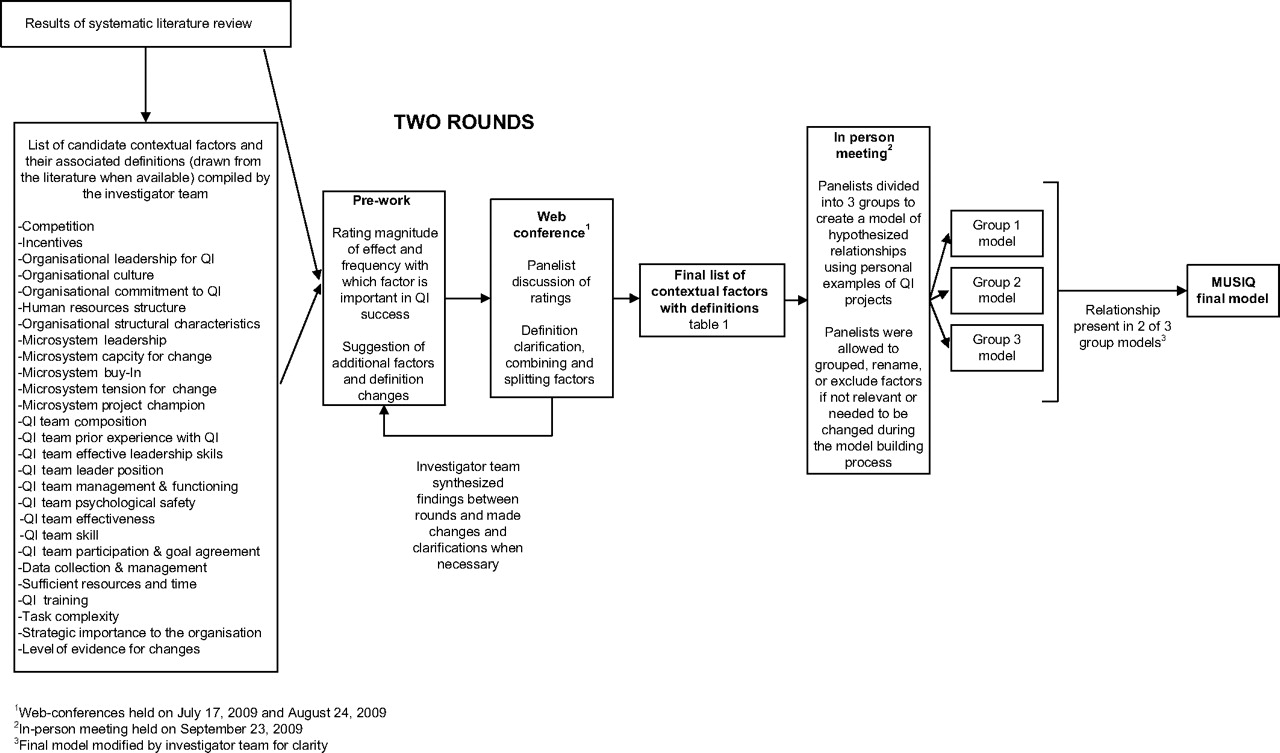
Model development process. A panel of experts were provided with the results of a systematic literature review and then participated in two rounds of opinion gathering to identify and define important contextual factors. Panellists subsequently met in person to identify relationships among factors to be included in the final model. MUSIQ, Model for Understanding Success in Quality; QI, quality improvement.
Prior to each meeting, panelists undertook the following tasks: (1) they suggested clarifications to definitions of contextual factors; (2) they rated factors on their importance in QI success and the frequency with which factors were influential (using four-point Likert scales); and (3) they suggested additional potentially relevant factors. Panellists were sent the results of their personal ratings as well as a summary of ratings of the entire panel before participating in the web conferences. During the web conferences, measures of disagreement in the factor ratings were used to guide discussions. Between rounds, the investigator team used the results of the expert panel discussions to make decisions about combining (or splitting) factors into broader (or narrower) constructs, eliminating factors that were felt not to be aspects of context, and clarifying definitions to reflect the expert panel discussions.
The 1-day, in-person meeting focused mainly on identifying causal relationships believed to exist among factors that would be included in the logic model and would help to explain the mechanism of action by which contextual factors affect QI outcomes. Experts were divided into three groups based on background and area of expertise in order to ensure a diversity of perspectives. Using personal examples of QI projects, each group constructed a model identifying hypothesised relationships between the contextual factors and their relationship with QI success. The final version of MUSIQ reflected relationships for which there was agreement between at least two out of the three groups. Investigators modified the final model slightly for clarity. Four relationships initially hypothesised as potential moderating effects were simplified into direct relationships in the version of the model presented here.
Results
Key contextual factors influencing QI success
A list of the key contextual factors identified by the expert panellists for inclusion in MUSIQ and the final definitions of these factors (refined through the panel's iterative process) are provided in table 1. Additional details describing changes in the key contextual factors and modifications to contextual factor definitions resulting from each of the three expert panel meetings are presented in online appendix S2.
Contextual factors included in the Model for Understanding Success in Quality (MUSIQ)
The definitions reflect the panellists' emphasis on the importance of examining specific contextual factors across multiple levels. For example, factors such as motivation, leadership, and culture operate at multiple levels. Panellists emphasised that including a separate factor for leadership at the organisation, microsystem, and team levels is important because key leadership behaviours are slightly different in each setting. Final definitions also reflected discussions about the importance of embedding directionality within construct definitions. Contextual factors were identified and defined so that they could be readily operationalised and, consistent with the supporting literature, to have positive hypothesised relationships with QI success. Having this directionality became important in the model-building process and in anticipating future testing to validate the directionality of these constructs and model relationships.
Relationships among key contextual factors in MUSIQ
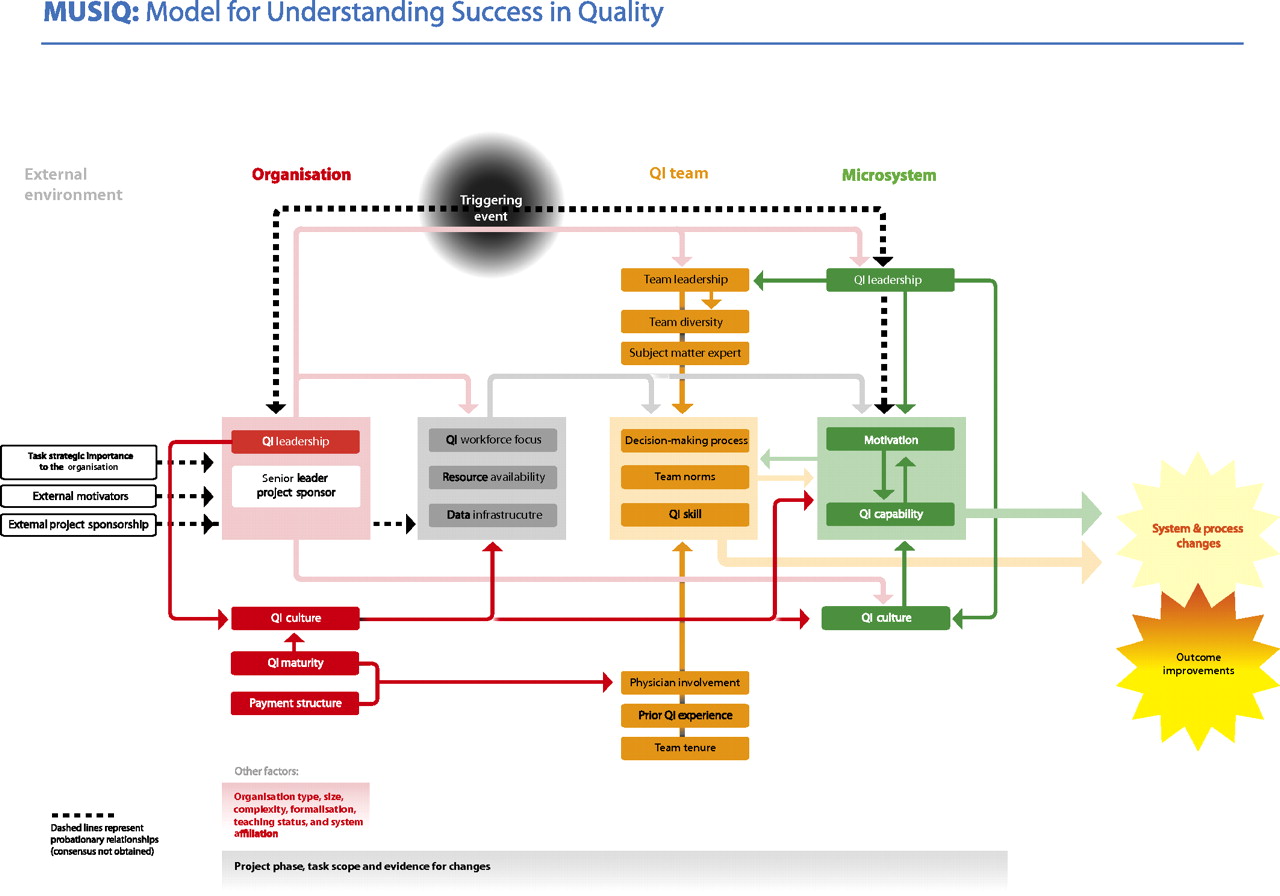
The final version of MUSIQ (figure 2) hypothesises that QI success (eg, the implementation of system and process changes and associated outcome improvements) is influenced directly by microsystem and QI team factors which are interdependent and mutually reinforcing. The microsystem staff's motivation and QI capabilities are central to QI success and influence how well they will implement necessary changes. The functioning of the QI team, including its decision-making processes, norms, and QI skills, are also critical to QI success in that the QI team is directly responsible for guiding the application of QI methods to implement change. QI team functioning is shaped by a number of other contextual factors, including diversity of team members, physician involvement, prior QI experience, presence of subject matter expertise, and team tenure.
{kind=link}
{kind=link}
Model for Understanding Success in Quality (MUSIQ). MUSIQ shows how context influences the success of individual quality improvement (QI) projects. Contextual factors are organised based on the level of the healthcare system in which they are believed to operate, including the microsystem (green), organisational or macrosystem (red), and environmental levels (white). Factors relating to aspects of QI support and capacity (grey) or characteristics of the QI team (orange) are identified as existing across system levels. Factors not assigned to a specific system level are also in white (eg, triggering event, task strategic importance).
The local microsystem context and the characteristics of the QI team are partly a function of the larger organisation in which they reside. While aspects of organisational context such as size, teaching status, and system affiliation may affect QI success, these non-modifiable characteristics do not factor prominently in MUSIQ. The extent to which physicians are employed and compensated and the sophistication and maturity of the organisation's QI programme were felt to be important in both encouraging physician involvement in QI teams and in establishing a culture supportive of QI (eg, values and norms that shape staff behaviours in support of QI). A culture supportive of QI, both within the organisation and microsystem, is hypothesised to have significant influence across all levels of the system.
Leadership is a pervasive and important theme throughout MUSIQ. At the organisation level, senior management leadership directly influences the development of a QI culture and guides resources and investment to support improvement. Senior management leadership also sets the tone for effective QI team and microsystem leadership. QI team leadership is important in overall successful QI team functioning and microsystem leadership is critical in establishing a culture supportive of QI within the microsystem, developing microsystem QI capability, encouraging staff motivation to improve, and promoting strong QI team leadership.
Factors relating to QI support and capacity are hypothesised to influence QI success. Having a system to collect, manage, and facilitate the use of data to support QI, having financial support (including allocation of resources and staff time), and development of the workforce to engage in QI through training, reward systems, and expectation setting are all believed to be important in facilitating the improvement work of the QI team and microsystem.
MUSIQ hypothesises that external pressures/incentives and project sponsorship by outside entities encourage organisational QI leadership to support particular QI initiatives. In addition, external project sponsorship can influence areas of workforce focus, resource availability, and data infrastructure by providing contributions of personnel, expertise, money, equipment, training, or other resources that aid a specific project. These two contextual factors that exist within the socio-political environment did not generate consistent support among panellists with respect to the mechanism of action by which these factors exert influence; therefore, relationships in MUSIQ are shown as ‘probationary’ to reflect the lack of consensus. Similarly, factors relating to the underlying motivation driving the choice of a QI project received uneven support as to the mechanism by which they influence QI success and are shown with ‘probationary’ relationships. For example, the presence of a positive or negative triggering event was believed to exert influence by encouraging QI leadership to support a specific improvement focus and by motivating staff, and alignment of the QI project goals with the organisation's overall strategic plan was hypothesised to influence organisational leadership to champion specific QI projects.
While determined not to be aspects of context, other factors, including project phase (eg, point in the course of the project between launch and sustainability), project complexity, project scope, and the level of evidence for changes, were identified as potential moderators of the relationships depicted in MUSIQ. However, in the interest of parsimony, the potential for moderating relationships, interaction effects, feedback, and reciprocal relationships (eg, double-headed arrows) were not fully explored by the panel and, as a result, none are included in MUSIQ.
Discussion
In order to adequately understand the context-sensitive features of QI implementation, explicit conceptual models are needed to outline the relationships among contextual factors and QI outcomes. Because QI occurs within the complex healthcare system, a theoretically informed model provides a powerful tool to help the mind conceptualise these complexities.30 MUSIQ identifies 25 key contextual factors likely to influence QI success, organises the factors based on the level of the healthcare system in which they are believed to operate, and explicitly identifies hypothesised relationships among contextual factors and QI success. In so doing, MUSIQ may provide a lens for QI researchers and implementers to organise their thinking about the role of context in QI implementation and facilitate studying the mechanisms of action of how context influences QI success, which may make efforts to optimise contextual factors to improve the success of QI initiatives more effective.
In developing MUSIQ, expert opinion was combined with published literature.13 Aspects of context in MUSIQ, including organisational leadership, culture, QI maturity within the organisation, and data infrastructure, have the strongest evidence base in the existing literature. Other aspects of context included in MUSIQ such as physician involvement, microsystem motivation to change, QI team leadership, and resource availability were studied less frequently in the published literature, but had consistent associations in the small number of studies examining these factors. The remaining contextual factors included in MUSIQ are supported by isolated reports in the published literature and by the expert panel's extensive collective experience with QI implementation in both healthcare and industry.
Because a system is a product of both its individual parts and their interrelationships, any effort to better understand the context-sensitive nature of QI implementation requires attention to the interconnections among all of the contextual factors.30 Literature examining the role of context in QI success is in an early stage of development and few studies have examined these complex associations and relationships.13 Therefore, panellists used their collective QI experience, knowledge of the literature, and group discussion to hypothesise relationships among contextual factors and QI success as outlined in MUSIQ. It is reassuring that in the few studies of indirect relationships between context and QI success, the literature supports the relationships identified in MUSIQ. For example, others have shown that external motivators (eg, competition), organisational culture, and organisational leadership influence chronic care improvement through effects on workgroup and team effectiveness.31 32 This is similar to the general hypotheses outlined in MUSIQ, which emphasise how the effects of organisational and environmental factors on QI success are mediated through factors within the microsystem and QI team.
Although previously developed models were not explicitly used in the model development process, MUSIQ aligns well with related models and frameworks. For example, many of the sub-elements of the context and facilitation categories of the Promoting Action on Research Implementation in Health Services (PARiHS) framework are prominent features in MUSIQ (ie, leadership, effective team work, decision-making process, culture, skills and attributes, roles, etc.).33 34 In addition, the concepts of the outer setting and inner setting included in the Consolidated Framework for Implementation Research (CFIR) are captured in MUSIQ by including a range of factors operating in both the external environment (outer setting) and the organisation and microsystem (inner setting).35 Furthermore, nearly all of the high-priority contexts for assessing QI and safety initiative effectiveness identified in an Agency for Healthcare Research and Quality (AHRQ) funded programme are included in MUSIQ.10 12 36 Factors such as structural organisational characteristics (eg, size, location, financial status, existing quality and safety infrastructure), external influences (eg, regulatory requirements, payments and penalties, national campaigns or collaboratives, local triggers/sentinel events), unit teamwork and leadership, and availability of implementation and management tools (eg, education and training, dedicated time, data feedback) are also included in MUSIQ.36 Elements included in MUSIQ are also supported by other relevant frameworks and models, including those described by Pettigrew et al,37 Lukas et al,38 O'Brien et al,39 and Cohen et al.40 What distinguishes MUSIQ from other models, however, is its broad focus on QI implementation, its relevance for individual QI projects occurring within single (or across multiple) microsystems, and, most importantly, that it maps the relationships among contextual factors to enable a deeper understanding of the mechanism of action by which context influences QI success. In addition, the systematic effort to take into account expert opinion and the results from a comprehensive systematic review of the literature13 contribute to MUSIQ's strong face validity.
As is common with social science theory development, there were key challenges in developing this conceptual model. First, the significant causal complexity of the subject matter made it difficult, if not impossible, to capture all of the contextual variables and relationships. In addition, representation of this model required significant simplifications that may inadequately or falsely represent reality. Therefore, what emerged from this theory-building process is a model that hopefully will help to explain the role of context in QI success in many specific circumstances. The authors recognise that there may be instances when aspects of MUSIQ may not apply (eg, QI implementation in small primary care offices where organisational factors such as QI leadership from the chief executive officer are not relevant or when certain contextual factors such as the distinction between QI team and microsystem leadership may need to be re-interpreted). As MUSIQ is applied in real-world settings, the authors hope to learn from anomalies where it fails to explain QI success accurately.41
Although in an early stage of development, the authors envision that MUSIQ could be used by others in a number of ways. MUSIQ has already been used to identify existing measures of contextual factors, develop new measures of key aspects of context, and test the relationships proposed in the model in more than 70 QI projects. The authors believe that using a common language and logic model such as MUSIQ will help align research efforts and generate knowledge more rapidly. It could lead to better standardisation of terminology and it could direct attention to specific hypotheses that can be tested in order to delineate the mechanism of action through which context affects the success of QI efforts. It could also inform quantitative research by providing a framework to guide the development and validation of measures to assess contextual factors. Although some rigorous efforts to develop measures of the factors influencing QI success have been published,42–46 the authors believe these efforts would benefit from closer alignment with relevant conceptual models, such as MUSIQ.6 9 In addition, hopefully MUSIQ will encourage researchers to use methods and study designs that are useful in understanding complex systems, including testing direct and indirect effects, the use of multi-level approaches and mixed methods approaches.
MUSIQ has also proven useful in helping QI implementers reflect on aspects of context that are important in the ultimate success of their QI project in a systematic way. Participants in the IHI Improvement Advisor programme have used MUSIQ at the outset of their QI project to think about contextual factors as they relate to their planned project. This self-assessment has helped them identify aspects of context that are weak in their setting and MUSIQ has helped them to take a comprehensive approach regarding what can be done to modify these aspects of context by intervening across multiple levels of the system. For example, to influence organisational leaders to provide resources and support for a given project, QI teams have considered demonstrating how their QI project aligns with the organisational strategy and how project sponsors in the external environment (eg, national collaboratives, IHI) have endorsed the effort. The authors encourage practical implementers to use MUSIQ to develop theories about which aspects of context help or hinder their project and test changes to aspects of context using Plan-Do-Study-Act (PDSA) methods. A key part of the PDSA cycle involves making explicit hypotheses and predictions prior to undertaking a test, and MUSIQ will help make these predictions explicit.47
The authors believe the aims and uses for MUSIQ among both QI researchers and implementers are well aligned. Hopefully MUSIQ can guide the collection and analysis of data in QI projects occurring in real-world settings with a goal of creating generalisable knowledge to support more effective implementation of QI methods in healthcare.6
Acknowledgments
We would like to thank all of the expert panel members (online appendix S1). We would also like to thank Carolyn Luzader for her help in facilitating the expert panel web-based and in-person meetings; Amy Borgert Martin and Brooke Mullet for help in executing the model development process; and Oscar Ferndandez for graphic design expertise in creating the graphic representation of MUSIQ (figure 2).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online appendix A
- Data supplement 2 - Online appendix B
Footnotes
Funding Support for this research was provided by Grant 65149 from the Robert Wood Johnson Foundation.
Competing interests None.
Ethics approval Exempt Determination by Cincinnati Children's Hospital Medical Center IRB.
Provenance and peer review Not commissioned; externally peer reviewed.