Article Text

Abstract
Background Central line-associated bloodstream infections (CLABSIs) are major contributors to preventable harm in the inpatient paediatric setting. Despite multiple guidelines to reduce CLABSI, sustaining reliable central line maintenance bundle compliance remains elusive. We identified frontline and family engagement as key drivers for this initiative. The baseline CLABSI rate for all our paediatric inpatient units (January 2016–January 2017) was 1.71/1000 central line days with maintenance bundle compliance at 87.9% (monthly range 44%–100%).
Objective To reduce CLABSI by increasing central line maintenance bundle compliance to greater than 90% using kamishibai card (K-card) audits and family ‘key card’ education.
Methods We transitioned our central line maintenance bundle audits from checklists to directly observed K-card audits. K-cards list the central line maintenance bundle elements to be reviewed with frontline staff. Key cards are cue cards developed using a plain-language summary of CLABSI K-cards and used by frontline staff to educate families. Key cards were distributed to families of children with central lines to simultaneously engage patients, families and frontline staff after a successful implementation of the K-card audit process. A survey was used to obtain feedback from families.
Results In the postintervention period (February 2017–December 2019), our CLABSI rate was 0.63/1000 central line days, and maintenance bundle compliance improved to 97.1% (monthly range 86%–100%, p<0.001). Of the 45 family surveys distributed, 20 (44%) were returned. Nineteen respondents (95%) reported being extremely satisfied with the key card programme and provided positive comments.
Conclusion Combining the key card programme with K-card audits was associated with improved maintenance bundle compliance and a reduction in CLABSI. This programme has the potential for use in multiple healthcare improvement initiatives.
- continuous quality improvement
- human factors
- lean management
- patient education
- paediatrics
Statistics from Altmetric.com
Introduction
Despite widespread initiatives to improve the quality and safety of healthcare, many patients continue to suffer preventable harm from central line-associated bloodstream infections (CLABSIs) worldwide.1 2 The Centers for Disease Control and Prevention (CDC) National Healthcare Safety Network (NHSN) reported that in 2017, about 24 000 CLABSIs occurred in acute care hospitals in the USA alone, despite 50% fewer infections from 2008.3 4 In addition to increased morbidity and mortality, the annual economic impact of CLABSI accounts for about US$ one billion of direct healthcare costs (based on 2013 data, USA).5 6 Harm events, such as CLABSI in paediatric patients, are often multifactorial, rendering them challenging to prevent. They can result from a breakdown at any of the multiple steps necessary for central line care, including hand hygiene, medication administration, fluid changes, dressing changes and accessing central lines. Each of the aforementioned steps further involves multiple processes that require adherence to specific infection prevention strategies, such as the use of alcohol or chlorhexidine wipes, alcohol caps on central line hubs, scrub and dry times, and chlorhexidine bathing.7–10
The CLABSI reduction practices vary widely across the world.11 Multiple guidelines are available across the world for CLABSI prevention in the form of clinical bundles, from various regulatory agencies, including the CDC (USA), European Centre for Disease Prevention and Control and National Institute for Health and Care Excellence (England and Wales).12 13 Clinical care ‘bundles’ are sets of three to five evidence-based practices created based on the current best practices and are proven to improve outcomes when performed collectively as intended.14 15 Adherence to such standardised bundles for CLABSI prevention also improves paediatric outcomes, as shown by the Children’s Hospitals Solutions for Patient Safety Network (SPS) in the USA.16 Despite evidence supporting the use of standardised bundles, ensuring reliable bundle compliance at the point of care remains a challenge for most healthcare organisations, and harm events from CLABSI continue to occur.
It is widely accepted that drifts in care practices at the frontline are usually followed by adverse outcomes,17 which was noted in our institution as well. Despite achieving the desired central line maintenance bundle compliance during some months at our institution, we found that sustaining it for every patient every time was challenging. Apparent cause analysis of CLABSI events from the last 3 years showed that the timing of infection was often related to central line care and maintenance beyond 2 days after line insertion. This was consistent with reports from the CDC (USA) that almost 72% of all CLABSIs reported to the NHSN in 2010 occurred more than 5 days after insertion, suggesting that infection prevention lapses likely occurred in the postinsertion care and maintenance of the central lines.1
A focused review of our non-compliant central line bundle audits using chart reviews and staff interviews revealed a combination of occasional missed checklists, knowledge gaps about bundle components, inadequate dressing changes and documentation gaps for line necessity. We identified frontline engagement as a common variable in all the non-compliant audits. We sought to engage our frontline staff with directly observed audits using the combination of face-to-face audits and non-punitive coaching though the ‘kamishibai’ rounding method. The kamishibai method is based on the use of the kamishibai card (K-card), a lean management tool based on Kaizen continuous improvement philosophy,18 shown to improve processes and reduce healthcare-associated infections.19 20 We subsequently designed a similar tool called the CLABSI ‘key card’ for families to help the frontline staff engage with families. Our baseline CLABSI rate was 1.71/1000 central line days with a maintenance bundle compliance of 87.9% (January 2016–January 2017). The aim of our project was to achieve and maintain zero CLABSI through frontline and family engagement. Our objective was to sustain greater than 90% compliance with the central line maintenance bundles by December 2018. We describe our quality improvement (QI) project using the SQUIRE V.2.0 framework.21
Methods
Hospital setting
Our hospital is a children’s medical centre within a medical school hospital campus, with over 80 inpatient beds, 4800 newborn deliveries and 20 000 paediatric emergency room visits yearly. Our Children’s Medical Centre has multiple interdisciplinary teams focused on preventing specific hospital-acquired conditions (HAC teams or HACs), all led by a physician–nurse dyad. Our multidisciplinary CLABSI reduction team consists of physicians, unit-based nursing managers and educators, QI specialists, mid-level providers, frontline nurses and ad hoc family representatives from our patient and family advisory council (PFAC), which is actively engaged in our quality and safety work.
Interventions
Frontline engagement and family engagement were identified as key drivers for our QI project. The core interventions included custom-designed audit tools referred to as K-card and key card.
K-card rounding for frontline engagement
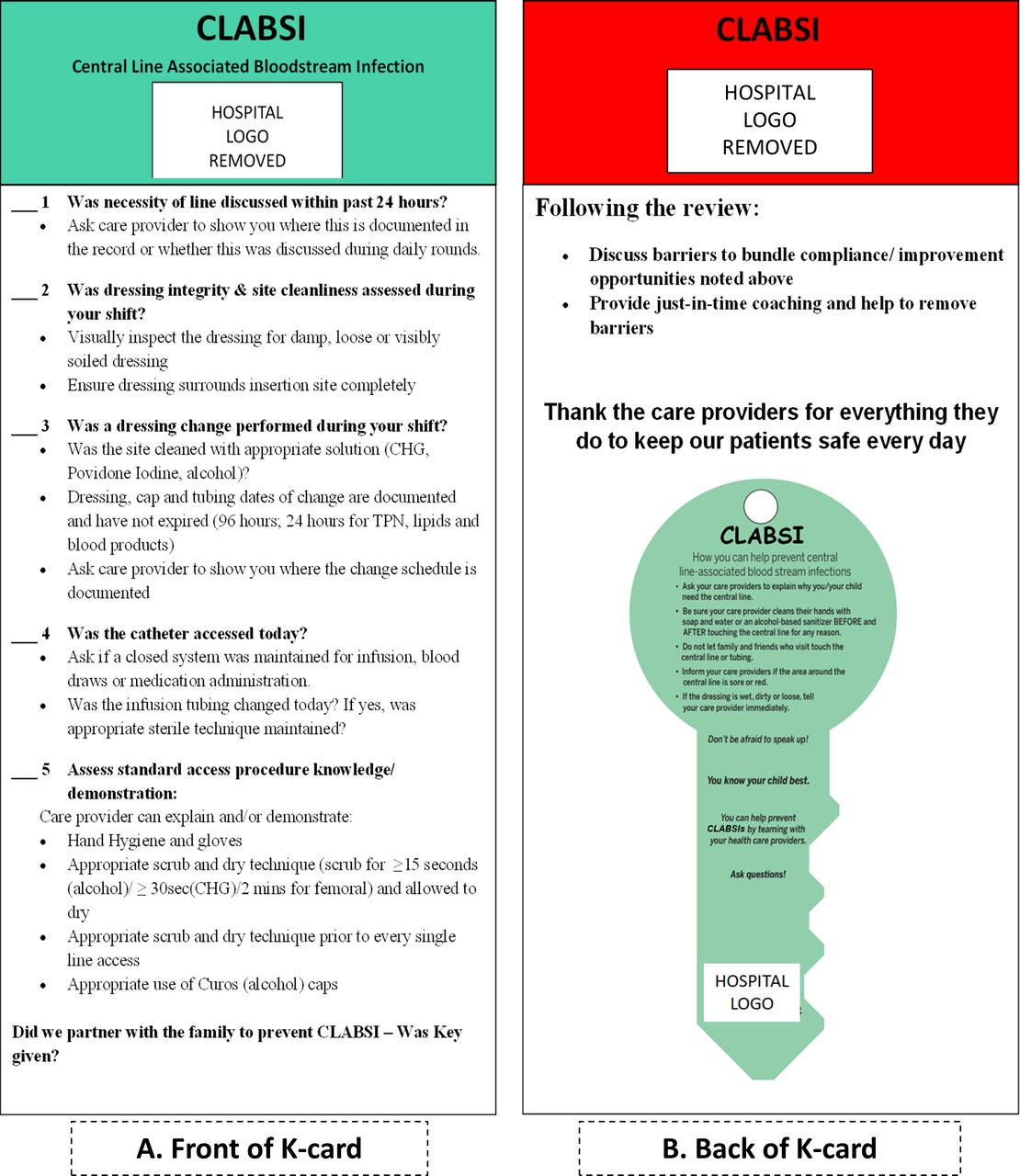
The K-card rounding concept for HAC prevention was modelled from the initial work of Helen Devos Children’s Hospitals and modified for our processes.15–18 The K-card for CLABSI is a laminated card that spells out the bundle elements for central line maintenance (figure 1) and used as a tool for auditing compliance to central line maintenance bundle elements. The audits were done by trained staff consisting of the CLABSI team leads, unit-based nursing leaders and nurse–educators. During the audit, each bundle element on the K-card was reviewed with the frontline staff. If all the applicable elements were completed correctly, the audit was considered a ‘pass’. The K-card was then displayed on the unit-based kamishibai board with its green side facing out. If one or more elements were incorrect, the audit was considered a ‘fail’, and the red side was displayed on the kamishibai board. The kamishibai board was centrally located in every unit, visible to staff and families. Failed bundle elements were used as coaching opportunities in real time and to identify challenges for execution at the frontline. Information about failed bundle elements was recorded only for QI purposes as a safety net, and identifying information was not displayed on the board. No punitive action was taken against the staff for failed audits. The staff were encouraged that our goal was to improve the entire unit’s performance and not to punish individual errors.

Modified K-card used for central line maintenance bundle audits is shown here. The K-card lists the standard central line bundle elements on the front (A) and a picture of the key card on the back (B). During K-card rounding, applicable bundle elements for the individual patient are reviewed with the patient’s frontline nurse. If all bundle elements are completed correctly, the audit is considered a ‘pass’, and the green side (A) is displayed on the unit-specific quality improvement board. If any of the items are incorrect, the audit is considered a ‘fail’, and the red side (B) is displayed on the wall. A monthly log of all audits is maintained by the CLABSI HAC team. CLABSI, central line-associated bloodstream infection; CHG, chlorhexidine; HAC, hospital-acquired condition; K-card, kamishibai card; TPN, total parenteral nutrition.
Key card for family engagement
The key card is a laminated card, shaped like a key with a plain-language summary of central line bundle elements on one side and action items related to bundle elements aimed at patients and families on the other side (figure 2). The concept for our key card programme was born as an extension of our K-card audits with frontline staff. When the K-card initiative was presented to our PFAC, the team discussed the creation of an educational tool that would allow patients (when age and developmentally appropriate) and families to understand what healthcare providers do every day to reduce the incidence of harm. While the K-card audits were intended as a substitute for retrospective chart review of checklists, the key card was designed as a cue card to facilitate frontline–family partnership. This project was aptly named the key card programme because we believe that a partnership between the healthcare team and the family is the ‘key to patient safety’. The goal of this tool was to extend the knowledge of the bundle elements outlined on the K-cards as a way to engage patients and families in harm reduction.
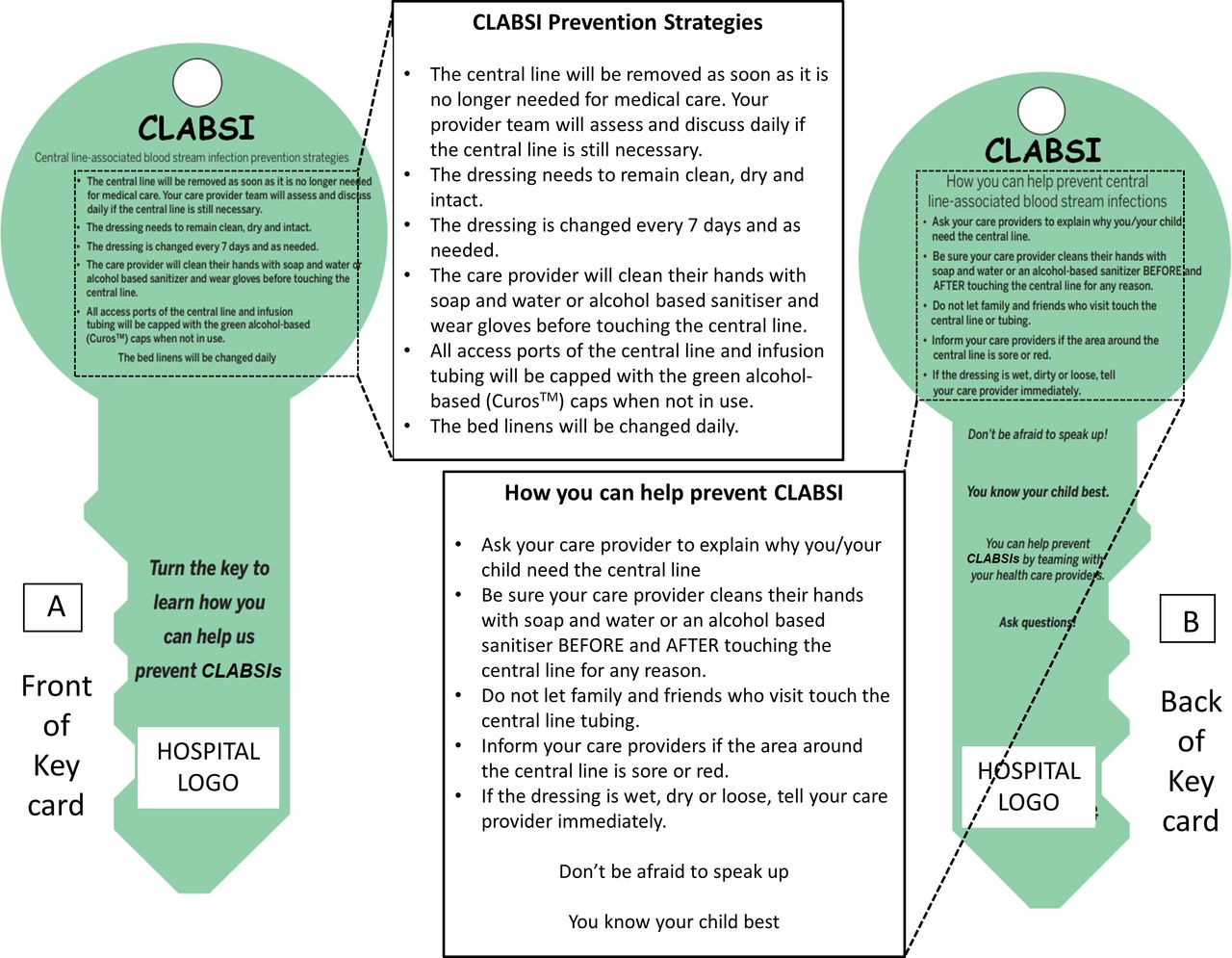
Key card for CLABSI reduction. The key card is shaped like a key, with the CLABSI bundle elements written in plain language on the front (A) and suggestions for parents/family members on what can be done to prevent CLABSI in their child (B). The content of the key cards is reviewed by the frontline staff with the parent or family member, explaining the individual bundle elements in plain language. The key shape signifies providing the family with the ‘key’ to their child’s safety. The text on the cards is magnified for better visibility. CLABSI, central line-associated bloodstream infection.
The Children’s Medical Centre organised a key card development team, which consisted of a core group of physicians, nurse educators, nursing leaders, frontline staff and ad hoc representatives from the PFAC. The key card development team targeted CLABSI for an initial pilot to test the concept. Our existing CLABSI team worked collaboratively with the key card development team from design to implementation. The teams reviewed current standards for harm reduction in various HACs from the SPS network, CDC, NHSN and The Joint Commission8 22 and translated them into plain language key cards. Our infection prevention department approved the initial draft of the CLABSI key card, which was then presented to our PFAC. Lastly, in addition to English, the key cards were translated into Spanish for Spanish-speaking families.
A standardised script developed based on the IPASS framework was used to communicate with the family.23 Our organisation had previously adopted IPASS as a standardised handoff tool, and applying it to the key card programme allowed us to limit variations in the style of communication when educating patients and families by using a communication process that was already familiar to the staff. The IPASS script for key card education included the following:
I: Introduce yourself and the Key card programme.
P: Establish Partnership with patient and family.
A: Acknowledge and explain HAC risk factors for the patient.
S: Summarise the ‘What (HACs, K-card, Key card), Why (goal of patient safety), How (prevention bundles)’ of the Key card programme.
S: Synthesis by receiver – ‘Are there any questions I can answer for you?’
The key cards were not used as audits. They were reviewed by the frontline nurse with families in an educational session to reinforce high-value CLABSI prevention practices. The family of every patient with a central line received a CLABSI key card, along with a detailed explanation of the programme. Following the initial education, the families were encouraged to engage with the frontline staff at every interaction and as needed for questions or concerns.
Process: moving from K-card to key card
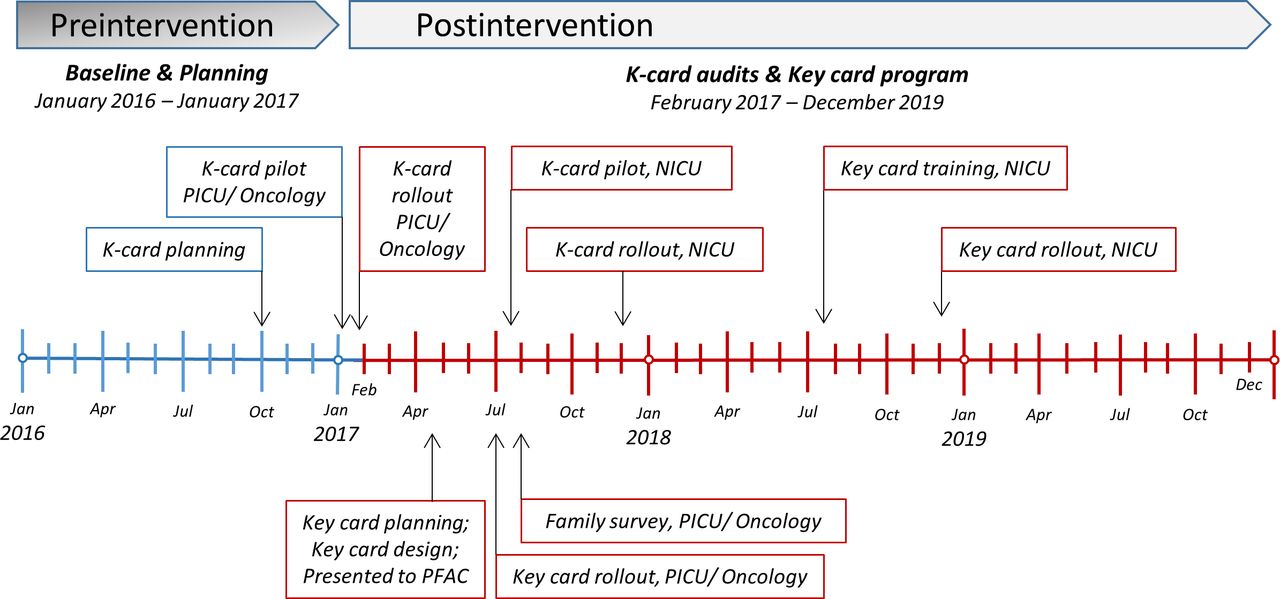
Our team first adopted the K-card rounding process for audits in January 2017 as a pilot and rolled out for in the paediatric intensive care unit (PICU) and paediatric oncology units in February 2017, followed by the key cards in June 2017. The K-card was rolled out in the neonatal intensive care unit (NICU) in December 2017 followed by key cards in December 2018. A detailed timeline of interventions is shown in figure 3.

Timeline of interventions is depicted in this figure. The baseline (preintervention) period is shown in blue and the postintervention period is shown in red. Timeline is annotated quarterly from January 2016 to December 2019. Vertical arrows for each intervention denote the month in which the specific intervention was rolled out. K-card, kamishibai card; NICU, neonatal intensive care unit; PFAC, patient and family advisory council; PICU, paediatric intensive care unit.
The planning phase for K-cards included designing K-cards, educating and training auditors to use non-punitive language and creating frontline awareness. During the pilot phase, simulated K-card audits were performed by the CLABSI team leads with a small group of enthusiastic frontline nurses. These audits were not counted for bundle compliance. Subsequently, a core group of auditors was created for each unit, who were assigned to perform a targeted minimum number of audits every month, aiming to capture as many nurses as possible.
The planning phase for the key cards included creating the key card, retraining the K-card auditors, educating the frontline staff on the key card process through a multimodal approach, including didactic learning sessions, emails, bulletin boards, staff meetings and huddles, direct observation and simulation sessions for using the standardised script. In the final phase, the key card process was transitioned to the frontline staff, which meant the frontline staff performed the key card education with families. Subsequently, a key card simulation training video was professionally developed using our staff and QI personnel as actors, aimed at training staff members. This was made available on the institutional internal website to review as needed.
The key card programme concept and tools were displayed conspicuously on the unit-specific QI board to increase ongoing staff and family awareness. The laminated key cards were displayed visibly in the patient rooms. Coloured paper copies of the key card were given to the family after each interaction to keep and share with other family members. After a brief pilot in the oncology population with indwelling central lines, the CLABSI key card was rolled out to the PICU, and subsequently the NICU, to include all paediatric patients with a central line. The process of performing audits for central line bundle compliance using K-card audits remained unchanged during and after implementing the key card programme. The interventions were rolled out using a series of plan–do–study–act cycles.24–26
Family engagement survey
An anonymous family engagement survey was developed to gather insight on the value of the programme and to identify opportunities for improvement during the initial phase of the key card programme (online supplementary file). The team sought to gauge whether the programme fostered a partnership between them and the staff, and whether it provided a better understanding of CLABSI prevention strategies and staff responsibilities. The survey also asked if the key card was easy to understand and if its purpose was explained clearly, and in a respectful manner. Overall satisfaction with the key card programme was assessed via a 5-point Likert scale. These surveys were distributed to the patients and families in person during their inpatient hospital stay after they received the key card education. The surveys were only given out during the early phase of key card roll-out. The families were expected to return the surveys voluntarily and were not pressured into completing the survey.
Supplemental material
Outcome and process measures
Our outcome measure was the rate of CLABSI, defined as the number of CLABSI events per 1000 central line days, consistent with the operational definition of CLABSI from CDC-NHSN.22 The number of CLABSI events was obtained using real-time microbiology reports in conjunction with our infection prevention department surveillance and case reviews. To monitor the impact of our interventions, compliance to central line maintenance bundle audits, obtained directly from the K-card audits, was used as our process measure. A core group of trained personnel conducted the audits to minimise variations. Family satisfaction rate from the family engagement survey was reported as a secondary measure.
Data analysis
A control chart (P-chart) was used to analyse CLABSI rate over time. Incidence risk ratio (IRR) was calculated for CLABSI rate (postintervention period CLABSI rate divided by preintervention period CLABSI rate). Process reliability (maintenance bundle audit compliance) over time was analysed as a control chart (P-chart) using control chart rules.27 Using the Shapiro-Wilk test for normality, the CLABSI rate, monthly bundle compliance percentage and monthly patient-central line days were found to be skewed. Therefore, the Mann-Whitney test (non-parametric counterpart to the two-sample t-test) was used to compare all three variables (CLABSI rate, monthly patient-central line days and monthly bundle compliance percentage) between preintervention and postintervention periods. The data analysis was performed using SAS V.9.4. Statistical process control charts were prepared using QI Macros (KnowWare International, Denver, Colorado, USA) plug-in on Microsoft Excel (V.2010).
Other considerations
The staff informed the parents about the programme and solicited their approval before proceeding with the key card education process. The staff were coached to communicate the following to family members: it is the medical team’s responsibility to ensure that everything is done in accordance with best practices. The key card is merely a tool to increase the parental awareness of best practices and to include them in the care of their child. Parents are encouraged to speak up freely if they notice any errors. The PFAC provides a support system to help parents understand their role. This initiative was reviewed by our institutional review board and fulfilled the criteria under QI. No potential conflicts of interest were identified with the interventions.
Results
Outcome measures
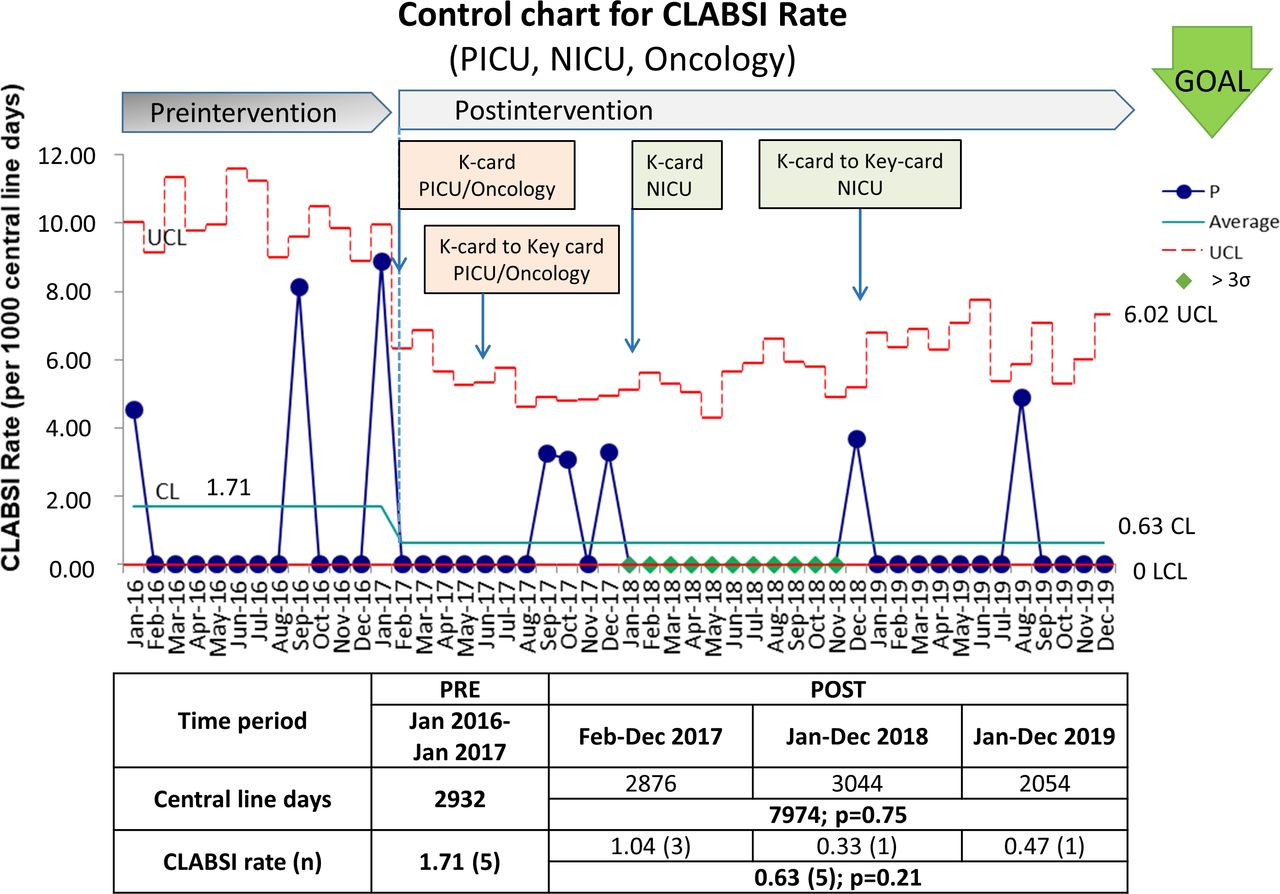
The cumulative CLABSI rate across all units (NICU, PICU and oncology) was 0.63 infections/1000 central line days for the postintervention period (February 2017–December 2019), a decrease from baseline rate of 1.71 in the preintervention period (January 2016–January 2017) (p=0.21), with an IRR of 0.37 (figure 4). This represents one CLABSI per year in each of 2018 and 2019. Furthermore, the infection in August 2019 was attributed to immediate postinsertion access and procedures based on our institutional review, which would not have been prevented using our K-card and key card interventions.
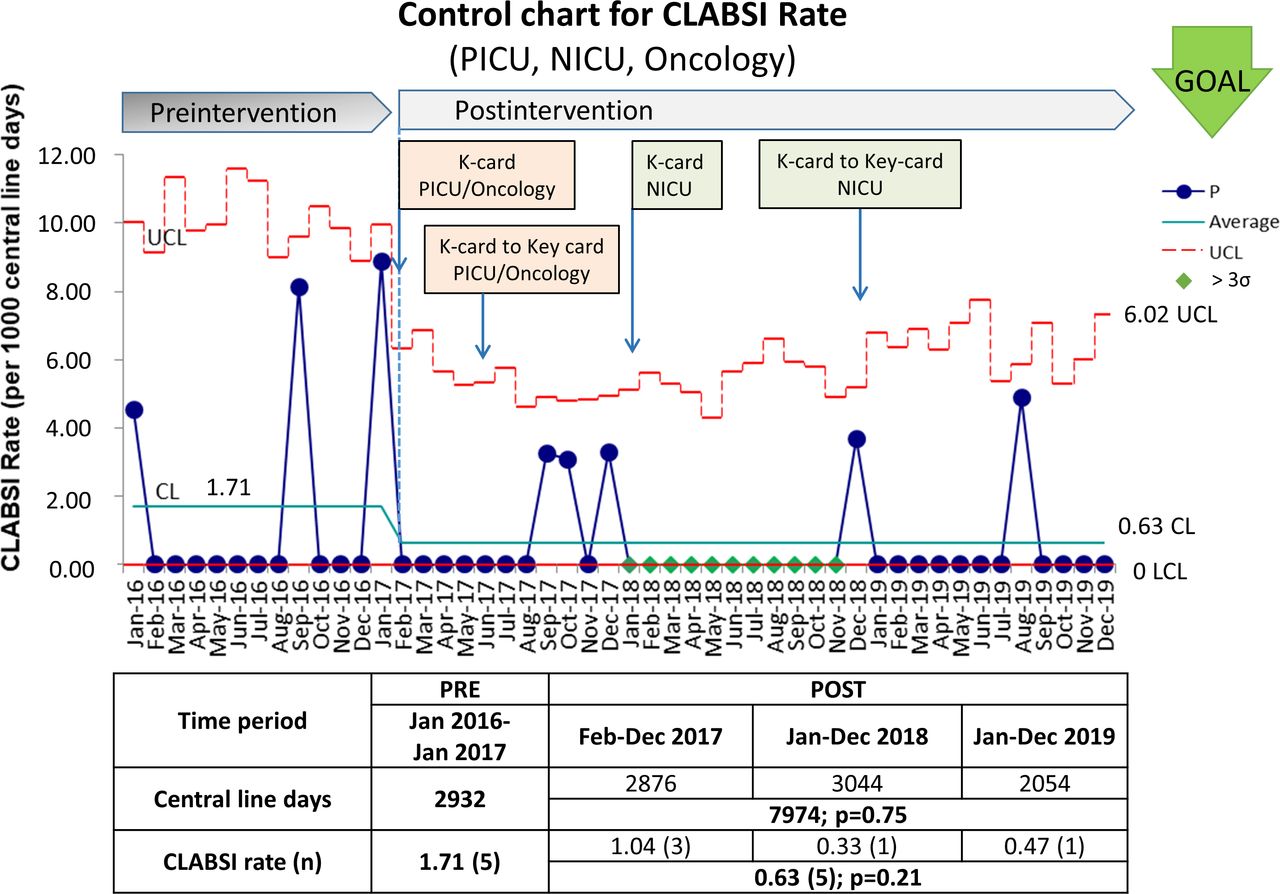
Outcome data for all units (NICU, PICU, oncology) are shown on this control chart (P-chart). The X-axis represents time in months from January 2016 to December 2019. The Y-axis represents the CLABSI rate per 1000 central line days. Lower and upper control lines (LCL and UCL) are denoted by red lines, and the green line (CL) represents the mean (centreline on the control chart). The green ‘goal’ arrow denotes the desired direction of change. Process change is denoted from February 2017. The cumulative CLABSI rate across all units was 1.71 infections/1000 central line days during the preintervention period and decreased to 0.63/1000 central line days during the postintervention period but was not statistically significant (p=0.21). The total incidence of CLABSI decreased from four to five cases per year to one in 2018 and one in 2019. K-card and key card roll-out timelines as annotated. The included table shows central line days and CLABSI rates during the preintervention and postintervention periods broken down by year. Central line days were not significantly different between the two periods (p=0.75; Mann-Whitney test). CL, centreline; CLABSI, central line-associated bloodstream infection; K-card, kamishibai card; LCL, lower control limit; NICU, neonatal intensive care unit; PICU, paediatric intensive care unit; UCL, upper control limit.
Process measures
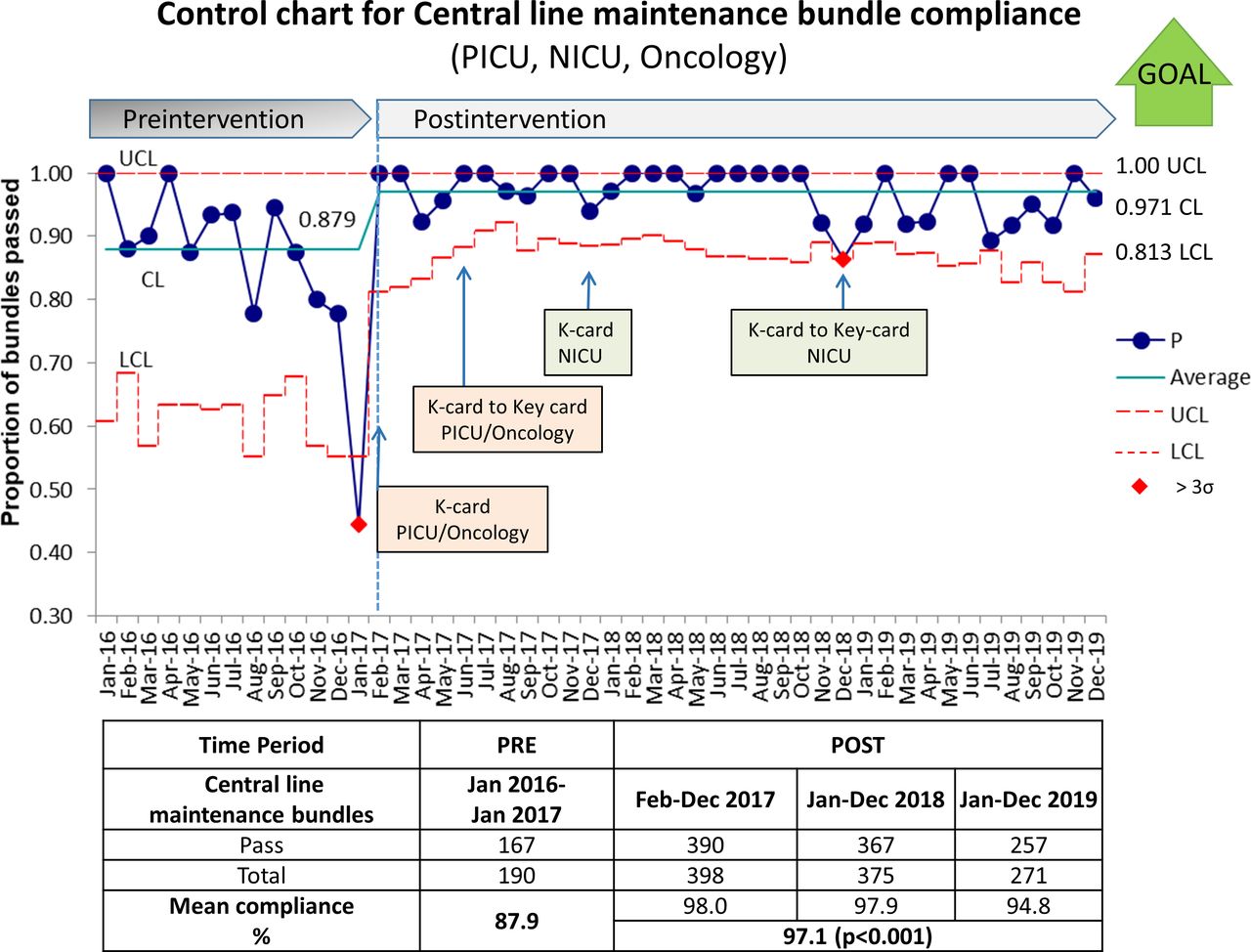
Our baseline compliance with the central line maintenance bundle was 87.9% (monthly range 44%–100%). Since February 2017, our bundle compliance improved to 97.1% (monthly range 86%–100%, p<0.001). Figure 5 shows the control chart for bundle compliance showing a process change from February 2017. The latter half of 2018 and early 2019 had a large number of new nurses in the NICU, coinciding with lower compliance and number of K-card audits. This was taken as an opportunity to start using key cards in the NICU. Our institution moved to a new electronic medical record system in October 2019, which coincided again with hiring new nurses who required training in K-cards and key cards. This was a challenging period with personnel shortage, associated with lower numbers of key card interviews and K-card audits. Despite the challenges, the bundle compliance continued to be under control around the new centreline at 97.1% (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Process data are represented here as a statistical process control chart or P-chart showing central line maintenance bundle compliance. The X-axis represents time in months from January 2016 to December 2019. The Y-axis represents the proportion of central line maintenance bundles passed. The red lines indicate UCL and LCL as denoted, and the green line (CL) indicates the mean (centreline on the control chart). Process change is denoted from February 2017 at the start of the programme. The green ‘goal’ arrow denotes the desired direction of change. Annotations denote when the interventions were rolled out. The chart shows that the process was in control around the new centreline after the process change. The included table shows the total number of central line maintenance bundle audits in the preintervention and postintervention periods. The mean bundle compliance increased significantly from 87.9% in the preintervention period to 97.1% in the postintervention period (p<0.001, Mann-Whitney test). CL, centreline; K-card, kamishibai card; LCL, lower control limit; NICU, neonatal intensive care unit; PICU, paediatric intensive care unit; UCL, upper control limit.
Family engagement survey
Of the 45 family engagement surveys distributed, 20 (44%) were returned for analysis. All respondents (100%) agreed that this helped them understand CLABSI prevention practices at our institution, and 95% (19/20) agreed or strongly agreed that they were extremely satisfied with the key card intervention. The families reported viewing their bedside nurses as advocates for their children. Many also expressed that a sense of control had been restored after understanding the safety practices aimed at preventing harm to their child and felt empowered to speak up. In addition to not coercing the families to complete the survey, some children had short hospital stays and some families did not stay with the children full time, further accounting for the low response rate.
Discussion
Frontline staff engagement and family engagement are the primary key drivers to our culture of safety and our high-reliability transformation journey. Using the K-card audits and key card education, our objective was achieved with maintenance bundle compliance over 90% annually since February 2017. Our CLABSI incidence decreased from four to five infections per year to one infection a year in each of 2018 and 2019, across all units. Although not statistically significant, the analysis is limited by a low number of infections. While a direct causal link between these interventions and a reduction in CLABSI cannot be established based on this project, improved staff knowledge and behaviours may have contributed to improving bundle compliance and, in turn, led to fewer CLABSIs.
Direct observation audits have previously been shown to improve compliance with central line maintenance bundles.19 20 The K-card audits provided the frontline staff with an opportunity to identify and address knowledge gaps and barriers. Due to the nature of the audit, this served a dual purpose of influencing behaviour and collecting reliable process data. The key cards extended the same concept to the patient (if age and developmentally appropriate) and their family members. Studies have shown that the act of teaching or explaining material to others improves one’s own long-term learning of the information.28 Combining the K-card audits with our key card programme likely served to solidify our frontline staff’s own knowledge of the central line maintenance bundle elements, as well as empowered them to engage their patients and families. It is possible that the frontline staff then performed better with the K-card audits due to improved knowledge retention. In order to hardwire subconscious staff behaviours, the CLABSI K-card audits were implemented for about 6 months in each unit prior to introducing the family engagement piece, the CLABSI key card.
Through the key card programme, we aimed to transform the patients and families from passive recipients of care to active members of the healthcare team, in line with our mission to evolve family-centred care. In addition to engaging frontline staff, the key card programme enabled the families to become partners in patient care. At a minimum, parents were noted to be more vigilant with hand washing and general hygiene practices. Patients and families have, on occasion, reminded a staff member to wash hands, or place alcohol caps on the central line tubing hubs. For example, a 6-year-old patient often reminded the nurses to place alcohol caps on his central line tubing hubs during daily tubing changes. The feedback obtained from families using the family engagement survey was overwhelmingly positive and helped strengthen our programme.
Our initiative showed that partnering with patients and families in the inpatient setting can reduce hospital-acquired harm in adults and paediatric patients, consistent with other publications.29–34 In 2002, The Joint Commission and Centres for Medicare and Medicaid Services (USA) encouraged patient and family participation in the acute care experience to promote safety.35 In a review of patient-focused quality interventions, Coulter and Ellins found that the majority of reviews on the effectiveness of strategies to inform, educate and involve patients in their treatment showed a positive effect on clinical decision-making, self-care and self-management of chronic diseases and patient safety.30 The patient and family’s role in healthcare is evolving rapidly with changes in healthcare trends, and healthcare professionals play a critical role by partnering with patients and families.31 However, partnerships with patients to improve safety can only be successful if patient involvement is valued and supported.31
Motivation, time, and commitment from the team members were vital to the success of our programme. There were several barriers during our project in the planning phase for both K-card and key cards, including the cost of printing materials, translation services, laminating the cards and obtaining infection control approvals for cleaning the cards appropriately. Our key card training video required input from staff, leadership, video editing services, identifying and training actors, writing the script, as well as the cost of making the video. During the pilot phase prior to the K-card roll-out, some staff reported feeling threatened during K-card audits. To address this, a great deal of time was spent training the auditors to perform the audits non-punitively, including watching videos and performing simulated and supervised audits. After K-cards became standard practice, the staff were more open to sharing their concerns without fear of failing the audits. An unanticipated barrier was the families taking the key cards home at discharge (especially in oncology). We subsequently clarified to families that key cards were meant to be hung by the bedside, and parents were given colour photocopies to take home.
The impact of the key card programme is not directly quantifiable since it drives change by improving knowledge retention and behaviours. Thus, sustaining the K-card audit compliance would indicate a positive impact of the key card programme. A limitation of this project is the difficulty in isolating the impact of the current interventions in the context of ongoing interventions to improve the culture of safety across our organisation. In addition, the improvement in maintenance bundle compliance in our project may also be partly attributed to a broad range of ongoing interventions targeting CLABSI reduction, including new display boards for QI initiatives, and interventions aimed at decreasing overcrowding in the NICU during times of high census. This intervention also does not address gaps in central line insertion practices. Nevertheless, in a complex world of harm reduction in patient care, we believe that improving frontline staff buy-in using knowledge retention techniques always has a positive role to play.
Conclusion
In conclusion, our key card programme for CLABSI reduction is a novel concept that can be combined with K-card audits to engage frontline staff and families simultaneously. We achieved sustained improvement in our central line maintenance bundle compliance and a reduction in CLABSI. Although causality cannot be established, this project provides a template for adopting educational interventions (such as K-card and key card) for frontline and family engagement. Our key card programme has now been expanded to other HACs, including catheter-associated urinary tract infections, breast milk safety and exclusivity, and newborn drop and fall prevention. This concept is scalable across a wide range of educational interventions in healthcare.
Acknowledgments
We thank our patients, families, quality improvement team members, physicians, nurses and the Department of Pediatrics for their participation in our patient safety initiatives.
References
Footnotes
RK and MG are joint first authors.
MLQ-A as the senior author.
Contributors RK and MG contributed equally to this paper. RK, MG, MLK and MLQ-A contributed to designing the study, intervention roll-out, data collection and analysis. MA and RK performed statistical analysis. All authors revised the manuscript and reviewed and approved the manuscript in its final form.
Funding The project was funded by the Departments of Quality and Safety, and Pediatrics at our institution.
Disclaimer The funding organisations did not have any role in the design, implementation, interpretation and reporting of the results.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. All data relevant to the study are part of our institutional quality improvement departmental records.