Article Text

Abstract
Objectives: To conduct a multicentre study on adverse event and near miss reporting in the NHS and to explore the feasibility of creating a national system for collecting these data.
Design: Prospective voluntary reporting by staff with anonymised transfer of data was used by a national system to collect data from 18 NHS trusts.
Participants: Staff from 12 acute trusts, three mental health trusts, two ambulance trusts, and one primary care trust.
Main outcomes measured: Number of incidents, date and time of incident, patient age and sex, clinical speciality, location, outcome, risk rating, type and description of incident.
Results: A total of 28 998 incidents were reported including 11 766 (41%) slips, trips and falls, 2514 (9%) medication management incidents, 2429 (8%) resource issues, and 2164 (7%) treatment issues. 138 catastrophic and 260 major adverse outcomes were reported. Slips, trips and falls (n = 11 766) were the most common type of incident.
Conclusions: Voluntary reporting by staff when linked to a multicentre data collecting system can yield information on a large number of incidents. This provides support for the principle of creating a national IT system to collect and analyse incident data.
- patient safety
- incident reporting
- adverse events
Statistics from Altmetric.com
Unanticipated adverse outcomes termed adverse events (or patient safety incidents), as well as near misses are frequent occurrences in healthcare systems.1–5 In a retrospective review of notes, adverse events occurred in 10.8% of admissions to acute hospitals in the UK with half of the events having preventable elements and one third associated with severe morbidity or mortality.6 An error rate of 49% was recently identified in intravenous drug administration.7 Other industries faced with errors and near misses have created reporting systems to collect data and thus provide an evidence base for the development of safety solutions.8 This has been advocated for health care.9 The Department of Health in England, under the leadership of the Chief Medical Officer, produced two reports—Organisation with a Memory10 and Building a Safer NHS11—which addressed the problem of medical error. At the same time, there were a number of high profile examples of failures in healthcare delivery including the inadvertent intrathecal administration of vincristine.12 The British Government responded by creating the National Patient Safety Agency (NPSA) to collect data on patient safety incidents and implement solutions to improve safety within the NHS in England and Wales. Critical to the success of a national reporting system is the question of whether clinical staff will report incidents. Fear of censure, severe time constraints, and a lack of focus on incidents are recognised to diminish willingness to report adverse events and near misses. A survey of US physicians and patients identified that neither group had a sense of urgency in relation to adverse event reporting.13 A study of doctors and the general public in the US found that, while the majority of physicians believed that reduction in medical errors should be a national priority, physicians were made less likely than the public to believe that quality of care was a problem (29.1% v 67.6%).14
At its inception, the NPSA had to learn whether staff in the UK would be prepared to report incidents. The Agency also had to pilot an IT based system of data collection. The purpose of the present study was therefore to evaluate multicentre incident reporting and assess the feasibility of creating a system which NHS staff could use to report nationally adverse events and near misses. The study was also conducted to inform the design of the future national reporting and learning system for the NHS by the NPSA.
In England and Wales there are over 700 NHS organisations with responsibility for delivering health care. These have been termed “trusts” and embrace hospitals, mental health providers, ambulance service providers, and primary care organisations (box 1). Before the study there was no requirement for these organisations to have any harmonisation of clinical risk management systems or processes. Organisations had various reporting systems ranging from commercially provided or locally built IT systems to paper based systems with varying degrees of sophistication. Reporting rates varied from thousands per organisation per year to very few. Managerial support for incident reporting was also variable. The present study evaluated, in a limited number of NHS organisations, whether it was possible to produce aggregated data on adverse events and near misses. NHS organisations with IT based systems and appropriate management support were thus recruited to the study.
Box 1 NHS trusts
At the time of the study, state funded healthcare delivery organisations in England and Wales were called “trusts”. The main categories were: acute (delivering hospital based care for those with physical illnesses), mental health (focusing on psychiatric disease), primary care (embracing all aspects of primary care including general practice) and ambulance trusts (focusing on ambulance services). Some trusts covered more than one area of work—for example, acute and mental health.
METHODS
The initial intention was to recruit 28 NHS trusts from England and Wales. It was planned to include those delivering acute services, mental health, ambulance services, primary care, as well as a representative private sector hospital. The initial study group was selected on the basis of the strength of management interest in clinical risk management and geographical location to ensure an adequate distribution across England and Wales. The approach taken in this study was not to alter the existing IT based reporting system but, rather, to evaluate whether a national system could be configured which technically had the potential to integrate with a diverse set of local arrangements. This approach had to be evaluated since it had a lower cost than requiring substantial change to existing systems. After the study commenced, it became clear that the IT systems used in a proportion of trusts had such differences in technical specification, and particularly in field definition, that data transfer was going to be a major challenge. Following review of the IT interconnectivity, only 18 trusts were able to participate and data from these were analysed. These trusts included 12 acute trusts, three mental health trusts, two ambulance trusts, and one primary care trust. The study period was from September 2001 to June 2002. The 18 trusts commenced entry data at different times during the study period.
Incident data
A broad definition of an incident was accepted as including any event which caused harm to a patient (adverse event) or potentially might have resulted in harm (near miss). Incidents of violence by patients against staff were included as such incidents could potentially have resulted in harm to other patients. Recognised outcome grading of “catastrophic”, “major”, “moderate”, “minor”, “none” was used.15 In order to reassure the clinicians entering the data, the NPSA insisted that, although local NHS trusts might know the names of those reporting incidents, all data received by the Agency was anonymous. This was achieved by checking that all data fields containing names of patients and healthcare staff had the names removed.
Data validation
As the data accumulated, it became clear that even the 18 selected trusts used markedly different reporting systems with different field names and field characteristics. Following data transfer to the NPSA, major inconsistencies with the data became apparent. It was therefore necessary to review manually all the events reported by each trust. A minimum acceptable data set was determined. The data for each incident were checked by a member of staff at each trust for the following data sets; time of incident, date of incident, patient age, patient sex, clinical speciality, location, risk rating, outcome for patient, type of incident, and description of incident. Following this validation, more than 95% of the data in each field was complete for all the incidents with the exception of the time of the incident where 10.4% of the reports lacked data.
Data analysis
Having collected data on nearly 30 000 incidents, as part of a process to initiate methodology development we invited a number of external collaborators (listed under acknowledgements) to review the data and generate questions which could be specifically addressed by NPSA staff sorting and examining the data. The data presented in this report cover all incidents but with special reference to those with a more serious outcome. Where possible, data have been aggregated. However, information obtained from very different services such as acute and mental health has also been reviewed separately.
The key question at the start of this study was whether a sufficient number of incidents would be reported to suggest that national data collection by the NPSA was a reasonable long term objective. Furthermore, the NPSA needed to know whether serious incidents would be reported via a national system and thus support the allocation of NHS central resources to data collection and finding preventative solutions.
RESULTS
Number of reports and reporting behaviour
A total of 28 998 reports were received. Of the 18 organisations who reported incidents electronically, there were 12 acute trusts, three mental health trusts, two ambulance trusts, and one primary care trust. Most reports (n = 27 474, 95%) were from acute trusts; of the rest, the majority (n = 1367, 5%) were from mental health trusts with only 156 (0.5%) from ambulance trusts and 32 from primary care trusts.
Category of type of reports
In the 28 998 records there were 108 different types of incident recorded, but most of these occurred rarely. The common categories related to falls, medication, resources, treatment, records, behaviour, medical devices, and clinical management (table 1). The most commonly reported incident was “slips, trips and falls” which accounted for 11 766 (41%) of the incidents notified to the NPSA. Of the incidents reported from all care settings, 138 were classified as catastrophic and 260 major (see below).
Frequency of different types of incident
Acute trusts
The 12 acute hospitals comprising the majority of the study group reported 27 475 incidents, 95% of all reports. The outcomes from 100 were catastrophic and a further 179 were classified as major.
The number of adverse incidents reported overall was generally higher in the day than at night and there was a trough in the middle of the day. However, slips, trips and falls—comprising the highest category of adverse incident type—occurred at a fairly even rate over the 24 hour day. Two thirds of all incidents (n = 18 269) happened on hospital wards, with more than half (n = 10 307) of these incidents being slips, trips and falls (table 2).
Location of incidents in acute trusts
In the 27 475 records from acute trusts there were 74 different categorisations recorded for clinical specialty. Half of the reports (52%) from acute trusts are accounted for by just six specialties (table 3).
Number of reports from the most frequent specialties reporting from acute trusts
Mental health trusts
The three mental health trusts submitted 1367 reports—about 5% of all reports. Mental health trusts had more reports in the early evening and fewer during the night.
The types of incidents reported by mental health trusts were quite different from those from acute trusts. Slips, trips and falls were still a high proportion (26%), but incidents related to violence, self-harm and abscondment were frequent (table 4). There were 10 inpatient suicides as well as 300 self-harm incidents and 21 attempted suicides. Twenty seven unexpected deaths were notified, but no clear pattern was seen when the text descriptions were reviewed.
Type of incident reported by mental health trusts
Ambulance trusts
Very few reports were available from ambulance trusts, with just 124 out of the 28 998 records. Ambulance reports related either to delays or failure in treatment (28% of reports) or delays or failure in admission (33% of reports). Ambulance trusts have a target of 8 minutes for life threatening calls (category A) with a minor delay resulting in notification of an incident. There were no unexpected deaths.
Primary care trust
The one primary care trust which participated submitted 32 reports.
Incidents with outcome reported as major or catastrophic
Specific analysis was performed on the 138 incidents categorised as catastrophic and on the 260 in the major category, derived from all care settings. While the most common location of these incidents was a ward (table 5), there were many other locations including the patient’s home. Of the large number (n = 10 307) of slips, trips and falls on hospital wards, 33 had an outcome classified as major or catastrophic. The data on which clinical speciality was associated with reporting the greatest number of such events are subject to a potentially large attribution bias. However, neonatalogy, A&E, adult mental health, endoscopy, obstetrics, anaesthetics, and old age mental health submitted reports with major or catastrophic outcomes (table 6). The methodology in the present study produced inadequate information on contributory factors for the major or catastrophic incidents. Thus, unexpected death was listed in 93 incidents, slips, trips and falls in 34, failure/delay in admitting to hospital in 31, failure/delay in treatment in 28, lack of adequate facilities/equipment in 26, resuscitation in 14, medication administering in 12, inpatient suicide in 10, and “other” in 41.
Locations of incidents with a major or catastrophic outcome
Number of reports by clinical specialty which resulted in a major or catastrophic outcome
Specific clinical problems
There were 616 (2%) incidents of self-harm or suicide, most of which had an outcome classified as “none” or “minor”. However, there were 13 suicides with three in the community, all of which were reported by mental health trusts. There were also 22 attempted suicides. Although 5% of the total reports were from mental health trusts, over half (54%) of the self-harm or suicide grouping were from these trusts.
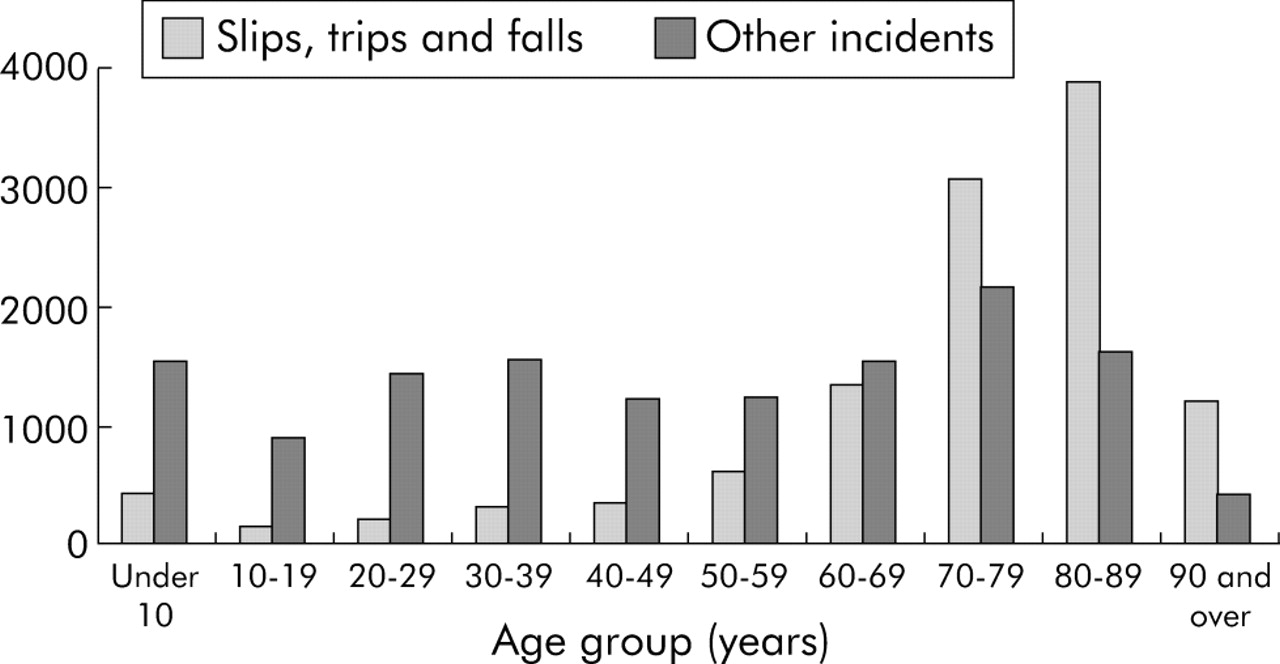
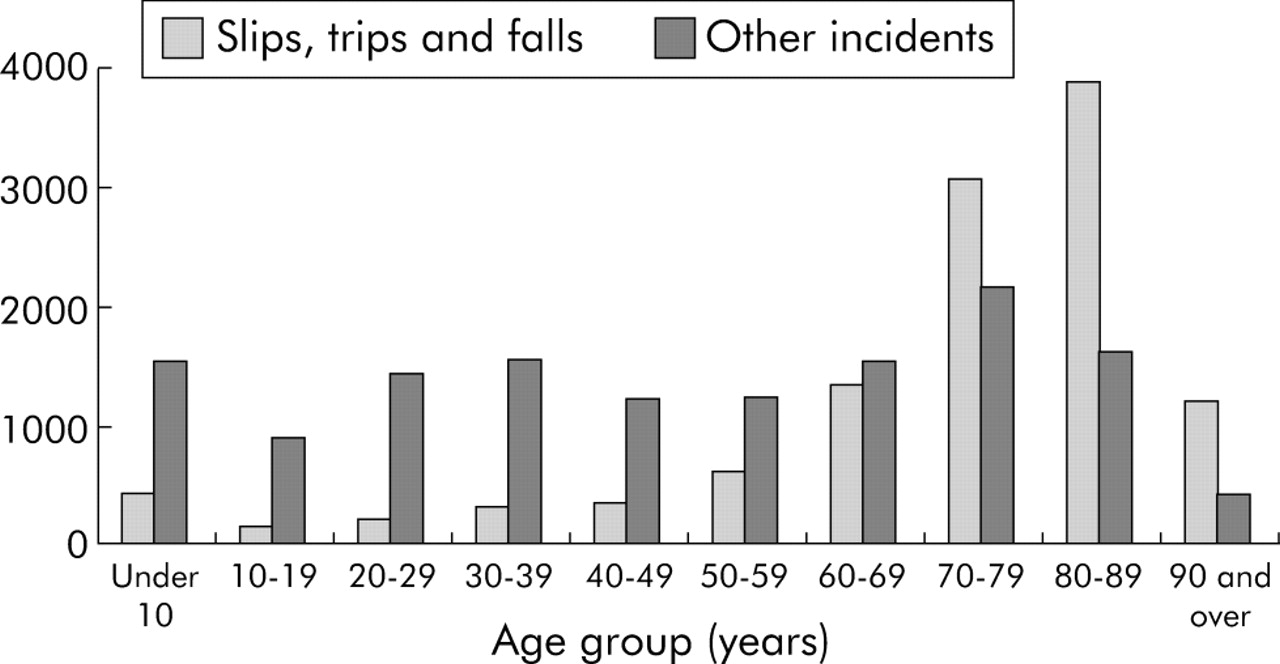
Slips, trips and falls accounted for 41% of the incidents reported in this study. The age distribution of those involved in these incidents was quite different from other types of adverse incidents (fig 1). The number of these incidents reported to the NPSA increased with patient age. For patients in their 60s, slips, trips and falls accounted for 47% of the reports, while for those in their 70s and older the majority of reports were of this type.
{kind=link}
Comparison by age of slips, trips and falls with all other incidents.
Medication management was the second highest category of adverse incidents with 2514 reports accounting for 9% of the reports. Within this category, medication errors accounted for 45.5% (n = 1193), administration errors 23.7% (n = 596), supply 11.7% (n = 293), prescribing 7.6% (n = 191), infusion problems 6.4% (n = 161), adverse drug reactions 2% (n = 51), and others 1.2% (n = 29).
DISCUSSION
Main conclusions of the study
This study was able to collect information on nearly 30 000 incidents. This is the first multicentre evaluation of adverse events and near misses in the NHS. The data do not permit an analysis of incident rates, but a large number of incidents were collected from less than 5% of NHS organisations. This study thus confirmed that the objective of the NPSA to create a national system to collect data on incidents from all NHS organisations in England and Wales was likely to provide data on a large number of problems with healthcare delivery. The results yielded a gratifyingly rich data set covering a broad range of incident types and care settings.
As outlined in the methods above, there were major methodological problems with IT compatibility, connectivity, comparability of fields and data standardisation. These have informed the development of the NPSA national learning and reporting system for collecting data electronically. In particular, it is clear that any national system needs to have clear requirements and standards as opposed to attempting to fit in with existing local systems.
Despite the technical problems, it was apparent that large numbers of incidents did occur in the NHS, some of which had serious or catastrophic outcomes. NHS staff were also sufficiently concerned by such incidents to make reports. This suggests that, with an appropriate culture and the development of an appropriate IT system, it will be feasible to develop a national reporting and learning system for adverse events and near misses in the NHS.
Limitations of the study
There are many limitations to this study. The data are not representative of all healthcare organisations in the country with over 95% of incidents having come from acute hospitals. The participating organisations represent a small minority of those in England and Wales. Primary care in particular was underrepresented due to limited development of IT based incident recording systems covering multiple geographically dispersed healthcare delivery settings.
Voluntary reporting has many limitations. Incident reporting will be linked to the importance of the event in the reporter’s mind. There may be disincentives to report certain categories of incident. In this study there was no attempt to validate reports or to look for unreported incidents.
Causality is also not easy to infer. Thus, a minor delay in arrival of an ambulance to a fatally injured accident victim was an adverse event with a fatal outcome but there may have been no causal relationship.
Key messages
-
Substantial numbers (n = 28 998) of adverse events and near misses were notified from 18 NHS organisations.
-
Less than 2% (n = 398) were associated with catastrophic or major adverse outcomes for the patient.
-
Collection of this type of information was fraught with technical and IT interconnectivity problems.
-
Analysis of the data provided preliminary information on the major types of patient safety incident.
Although it is tempting to try to identify rates of incidents, there are several problems with defining a denominator for the rate. We have no data on number of patients treated nor on number of employees in the participating organisations. It is also important to remember that the data reflect number of reports notified by reporters not incident occurrences. Thus, clinical teams with a low tolerance of patient safety violations are likely to be associated with the greatest number of incident reports. For these reasons, we have not attempted to make statistical comparisons.
Lessons from the study
While this study was performed in the NHS in England and Wales, there are a number of lessons which apply to the development of similar systems in any country. A large number of incidents occur particularly in the acute hospital and mental health sectors. The majority of these do not result in harm to patients. However, a small number of incidents do have a major or catastrophic outcome. Robust data can be collected on adverse events and near misses, and reports on these can be used to help inform a programme of work to improve patient safety. Further work to address the causes of other patient safety incidents has already been initiated by the NPSA.
Acknowledgments
The purpose of data collection by the NPSA is to allow the NHS to learn and improve safety. This goal is not assisted by naming the NHS trusts from which the data were obtained. The authors would like to acknowledge the support and hard work of all staff within the NHS trusts who contributed to the data collection and validation.
Contributions to the data analysis were made by The World Health Organisation Uppsala Centre for monitoring adverse drug reactions; Professor Charles Vincent, Imperial College; Professor Trevor Sheldon, University of York; Professor Stephen Evans of London School of Hygiene and Tropical Medicine; Autonomy (Cambridge, UK); SAS UK and Ireland (Marlow, UK); SSSPS UK Ltd (Working, UK); and NRJ Consulting (Egham, UK).
REFERENCES
Footnotes
-
Conflict of interest: none.
These data have been made public in an appendix to the NPSA Business Plan 2002/3.