Article Text

Abstract
Background: Chemotherapy is prescribed according to protocols of several cycles. These protocols include not only therapeutic agents but also adjuvant solvents and inherent supportive care measures. Multiple errors can occur during the prescription, the transmission of documents and the drug delivery processes, and lead to potentially serious consequences.
Objective: To assess the effect of a computerised physician order entry (CPOE) system on the number of errors in prescription recorded by the centralised chemotherapy unit of a pharmacy service in a university hospital.
Patients and methods: Existing chemotherapy protocols were standardised by a multidisciplinary team (composed of a doctor, a pharmacist and a nurse) and a CPOE system was developed from a File Maker Pro database. Chemotherapy protocols were progressively introduced into the CPOE system. The effect of the system on prescribing errors was measured over 15 months before and 21 months after starting computerised protocol prescription. Errors were classified as major (dosage and drug name) and minor (volume or type of infusion solution).
Results: Before computerisation, 141 errors were recorded for 940 prescribed chemotherapy regimens (15%). After introduction of the CPOE system, 75 errors were recorded for 1505 prescribed chemotherapy regimens (5%). Of these errors, 69 (92%) were recorded in prescriptions that did not use a computerised protocol. A dramatic decrease in the number of errors was noticeable when 50% of the chemotherapy protocols were prescribed through the CPOE system.
Conclusion: Errors in chemotherapy prescription nearly disappeared after implementation of CPOE. The safety of chemotherapy prescription was markedly improved.
- CPOE, computerised physician order entry
Statistics from Altmetric.com
Medical prescription is the result of a complex cognitive process.1 As such, it must integrate several elements—namely, patient’s characteristics and medical conditions, treatment goals and particulars, institutional rules and habits, and the preferences of medical and nursing staff and of the patient. Medical order sheets are an essential way of communication between doctors, nurses and pharmacists. Medication errors refer to errors in the processes of ordering, transcribing, dispensing, administering or monitoring drugs.2 They can lead to adverse drug events, some of which are preventable. Recent studies have shown that about 50% of preventable adverse drug events during treatment occur during the prescribing phase.3–5 In a study specifically on ordering of drugs, about 20% of orders were found to be poorly legible and 24% were incomplete.6
Chemotherapy is given according to protocols and for repeated cycles. Potent and potentially toxic drugs are used, usually given with infusion solutions. The dosage is commonly adapted to the patient’s body surface area and/or renal function. Given the complexity of existing protocols, multiple errors can occur during prescribing, transmission of documents and drug delivery, potentially leading to serious consequences. Therefore, recommendations have been published to decrease the likelihood of errors occurring during the prescribing phase7: only experienced doctors must be given rights to prescribe drugs, and each prescription should be checked by a senior oncologist before it is transmitted to the pharmacy.
Computerised prescribing systems have several advantages. They are complete and legible, standard dosages can be automatically provided and the doctor who is prescribing can be identified at any time. Further, they eliminate the need for error-prone manual paper transcription, and provide a control over effectively administered drugs, because nurses record into the system every drug given to every patient. In addition, warnings about drug–drug interactions can be incorporated.8 Electronic prescribing systems have shown to improve the clinical outcome and to decrease the costs in antibiotic treatment.9
In this study, we assessed the effect of a computerised physician order entry (CPOE) system on the number of errors in prescription recorded by the centralised chemotherapy unit of the Pharmacy Service, University Hospital, Lausanne, Switzerland.
METHODS
Setting
The study was conducted in an 850-bed University Hospital, Lausanne, Switzerland, serving as primary care centre for the city of Lausanne (250 000 inhabitants), as a secondary care centre for a population of 650 000 inhabitants and being one of the two university hospitals in French-speaking Switzerland (1.8 million inhabitants). The multidisciplinary oncology centre is responsible for all adult chemotherapy prescriptions both in the inpatient and outpatient services (1500 and 20 000 treatments per year, respectively).
Development of the computer software
The development of the computer software followed different stages. Firstly, all existing chemotherapy protocols were collected and compared with original protocols. They were standardised for the whole institution by a multidisciplinary team composed of a doctor (RS), a pharmacist (MV) and an oncology nurse (NF). Then, a CPOE system was developed on the File Maker Pro software without professional programmer support. It consists of a prescribing module permitting chemotherapy prescription for individual patients, directly connected to the standardised chemotherapy regimen database, and automatically proposing standard doses based on body surface area (computed from the patient’s height and weight) or creatinine clearance. From the serum creatinine concentration, the software automatically computes the creatinine clearance according to the Cockroft–Gault formula.10 Standard doses can be decreased (or increased) to take into account patient-specific characteristics, particularly performance status, decreased renal or hepatic function, or toxicity during prior chemotherapy administration. An explanation for the dose modification is required, for each individual prescription and cytotoxic agent, by indicating the percentage of dose to be given. All drug doses can be rounded off within a prespecified range according to drug toxicity and commercially available packaging (the prescribing module will automatically indicate the available dose per package). After electronic signature and validation (or modification) by a senior staff member, the linked pharmacy module automatically edits the documents needed for centralised chemotherapy preparation and for billing. Finally, an administrative module issues working documents for doctors (summary of chemotherapy protocols and expected side effects) and for nurses (surveillance and treatment sheets). All corrections are instantly updated on all documents generated by the specific prescription. Access for consultation, modification or validation of a specific prescription is controlled by a multilevel access-rights module.
Prescribing process
Before computerisation, treatment blocks were not standardised between protocols and oncologists. The doctor’s prescription was retrieved from a preformatted handwritten document that was sent to the pharmacy service by the nursing staff. Both doctors and nurses checked the prescription and copied the necessary information for each drug on their specific working sheets. Identified errors had to be communicated to all other professionals involved, and corrected on several documents, with no guarantee of completeness.
Since computerisation, a prescription by a junior doctor is validated by a senior doctor online before being further processed by the computer software. Once validated, it is automatically transferred to the nursing staff and to the pharmacy service, and specific documents are edited directly by the computer software. Similarly, any correction on the initial prescription is immediately transmitted to all professionals involved. Any creation of a new chemotherapy regimen or any change to an existing standardised chemotherapy regimen has to be validated by the multidisciplinary team before implementation.
Assessment of the effect on safety
The effect of the introduction of the computer software on the prescribing phase was assessed as the number of errors or interventions recorded by the pharmacy service, which led to either an inquiry for additional information or a correction. These figures were expressed as percentages of the total number of prescriptions in a given month.
Errors were classified into major and minor errors, according to their potential effect on patients. Major errors referred to dosage or drug name, as well as type of medical device used (eg, infusion bag or syringe) or route of administration, whereas minor errors referred to the volume or type of infusion solutions.
The analysis compared two periods: before (15 months) and after (21 months) computerised protocols became available. In the second period, comparison was further carried out between computerised ordering and remaining handwritten protocols. Comparisons between outcomes were carried out on monthly error rates using the binomial test with 95% confidence interval (CI). The error rate was computed over time as a function of the percentage of computerised protocols used in a given month. Statistical significance was assumed at p<0.05.
As this study only observed current practice and did not involve patients directly, neither ethics committee approval nor patient consent was needed.
RESULTS
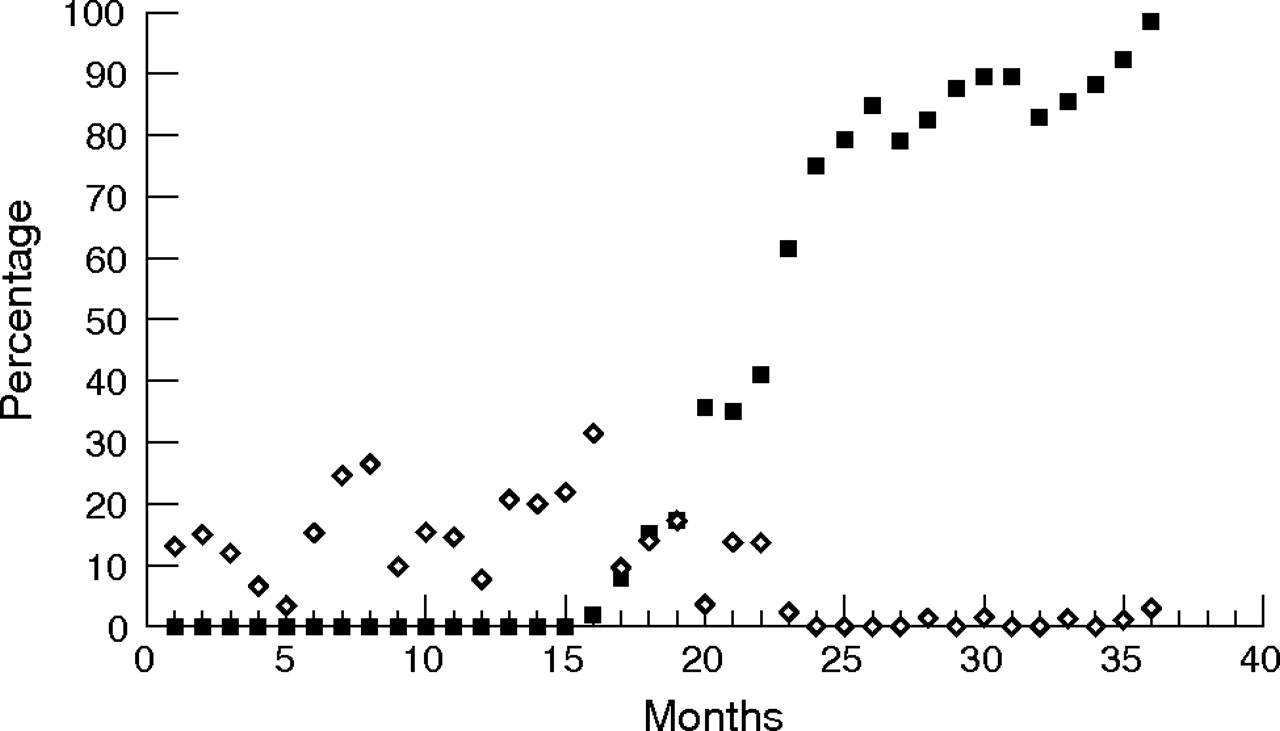
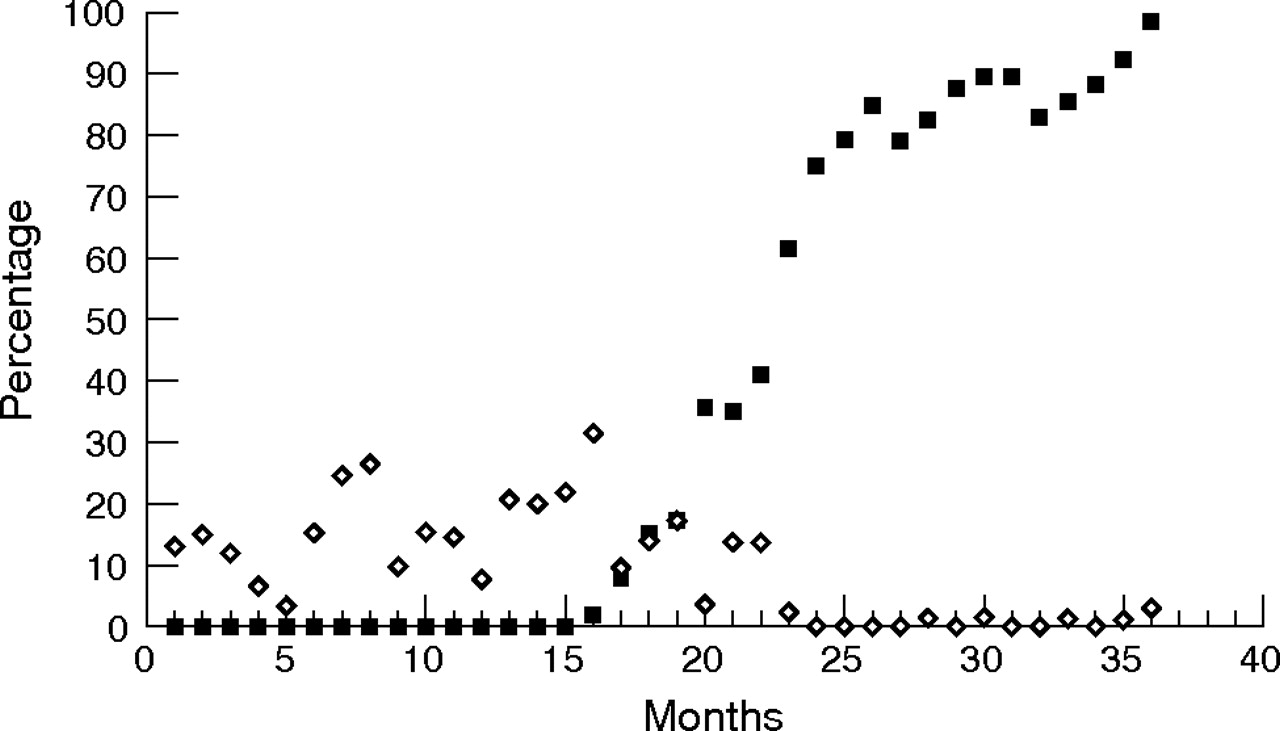
Before prescribing computerisation, 141 errors were recorded by the pharmacy for a total of 940 prescribed chemotherapy regimens (15%). Of these, 27 (19%) errors were major and 114 (81%) minor. The average monthly error rate amounted to 15% (95% CI 13% to 18%). After introduction of the CPOE system, 75 errors were recorded for 1505 prescribed chemotherapy regimens (5%). Of these errors, 69 (92%) were recorded in the 978 remaining handwritten prescriptions (7%; the prescribing module was not immediately available for all prescriptions); 17 (25%) were major and 52 (75%) minor. The average monthly error rate amounted to 13% (95% CI 10% to 16%). This decrease in rate was not statistically different from the rate observed in the first period (p = 0.36). In the 527 prescriptions using the computerised prescribing module, only 6 (1%) errors were recorded, all of which were minor. The average monthly error rate thus amounted to 0.6% (95% CI 0.3% to 1.4%). Table 1 shows a detailed distribution based on computerisation status, by months and in total, and the percentage reduction in errors. Altogether, the average error percentage decreased from 13.1% to 0.6%—a 22-fold reduction. Figure 1 illustrates the relationship between the percentages of errors and the percentage of available computerised protocols, showing that a dramatic change occurred when about half of the protocols were available in computerised form.
Temporal evolution of the numbers and percentages of errors recorded with the two different types of protocols (by month), before (months 1–15) and after (months 16–36) introducing computerised physician order entry
{kind=link}
Temporal evolution of the percentage of errors (open diamonds) compared with the percentage of computerised prescriptions (solid squares).
Table 2 shows the distribution of errors by types. Errors linked with handwritten prescriptions outnumbered those recorded with computerised prescriptions, except for the category “medical device”. A later version of the software included information about the presence or absence of a central venous access device as part of the patient information, thus enabling the provision of some chemotherapy agents as a short infusion rather than slow injection (eg, vincristine or doxorubicin).
Distribution of errors by type: handwritten prescriptions (1467 orders) and computerised prescriptions (978 orders)
DISCUSSION
Our study showed that computerised chemotherapy prescription had a substantial effect on the number of errors during prescribing, and thus on safety. This effect was long lasting. It was already noticeable after only 10% of protocols were computerised, and the errors were almost nil when half of the protocols were available in computerised form.
Studies have shown that computerisation can reduce variations in drug dosages for H1 blockade by 11%, as well as ondansetron prescribing exceeding the recommended doses (0.6% v 2.1%; p<0.001).11 Similarly, in a paediatric critical care unit, computerised prescribing reduced potential adverse drug events by 41% (from 2.2% to 1.3%), medical prescribing errors by 99% (from 30.1% to 0.2%) and violations of rules by 98% (from 6.8% to 0.1%), in 13 828 medical orders written for 514 patients.12
A review of 18 studies on CPOE showed that systems of this type can help in planning a therapeutic regimen and hold special promises for improving the quality and safety of drug prescriptions.13 A systematic review of five trials involving CPOE showed a positive effect on error prevention in two cases and on prescribing quality in three cases.14
More recently, attention was drawn to the potential failures of CPOE systems, as they involve complex modelling of diagnosis and treatment.13 CPOE was claimed to actually increase the number of adverse drug events and increase the costs, particularly during the first years after its introduction.15 Its lack of flexibility was emphasised in another editorial,16 underlying the fact that its full potential will be reached only to the extent that innovation surprises are identified, complex cultural and procedural issues considered, and conscious efforts made to preserve interacting with the healthcare team. A recently published study17 analysed a leading CPOE system in detail and identified 22 types of risks of medication errors, divided into two categories: information errors by fragmentation and systems integration failure, and human–machine interface flaws. Therefore, doctors should be aware that high levels of adverse drug events may occur even in a highly computerised hospital, if the CPOE system lacks decision support for drug selection, dosing and monitoring.18 This danger was also present in our study as a new category of errors appeared only with the CPOE system, which did specify the type of infusion material in which the chemotherapy drugs had to be prepared, because the information about the presence of a central venous line was missing.
Additional potential dangers include overlooking the fact that CPOE systems will neither correct unintended discrepancies in drug prescriptions recorded at the time of hospital admission between the outpatient regimen and the hospital treatment19 nor oblige doctors to comply with computer alerts. In a survey of five adult primary care practices, 3481 consecutive computer alerts (67 leading to interrupting prescriptions and 122 to maintaining prescriptions) were randomly selected for detailed analysis. This study showed that 91% of alerts about drug allergy and 89% of alerts about drug interactions of high severity were overridden. This was less often the case if the prescriber was a house officer (odds ratio (OR) 0.26 (95% CI 0.08 to 0.84)) or if the patient had multiple allergies (OR 0.70 (95% CI 0.53 to 093)), but more often the case for drug renewals (OR 17.74 (95% CI 5.60 to 56.18)). More disturbingly, 36.5% of these alerts were judged inappropriate. Eventually, no adverse drug event was observed in the group respecting the alerts, and only three events were recorded when the alert was overridden.20
Despite these limitations, CPOE systems have shown to reduce medication errors up to 81%, but to the best of our knowledge only one study has been recently published specifically on paediatric chemotherapy,21 although its complex prescriptions, drug combinations and required supportive measures make it error prone. This study showed that CPOE decreased improper dosing, incorrect dosing calculations and incomplete nursing checklists, but increased mismatch between drug orders and treatment plans. Our study is the first contribution focused on a pharmacy perspective. Our system works, did not require professional software developers, is flexible and can be adapted for changing needs over the years. In due time, it will be replaced by a professional new prescription system involving all hospital wards and disciplines.
Our study has also limitations. It involved only one centre, with few patients and a limited number of prescribers. However, its results seem to be valid as they have been stable over time despite a high staff turnover rate linked with our teaching hospital status (since its introduction, about 360 users for 23 500 prescriptions were recorded into the system). The classification of errors reflected only the pharmacist’s view and focused only on the prescribing phase. This scope should be extended to encompass the rest of the drug administration process, which contributes considerably to errors associated with drug prescription and administration.8
Although computerised prescribing may be more cumbersome for doctors than handwritten prescription, it carries several advantages. These include an easy access to prescribing history, the automatic editing of treatment plans and surveillance charts for nurses, and the issuing of nominal fabrication orders and also direct billing capacities for the pharmacy. The automated paperwork eliminates the risk of transcription errors. Their effect was not specifically considered in this study. The potential additional advantage of such a protocol database is that further modules can be added for quality assurance. Specifically, an additional sheet retrieving preparation error occurring in the central pharmacy could be used as a quality control measure. Similarly, nurses could add to the database all administration errors occurring during treatment, and doctors could incorporate all adverse drug events recorded during drug administration. In this way, the frequency of side effects could be systematically monitored, and experimental protocols could be modified when necessary. Finally, such a system could easily be adapted for other institutions as the software does not need special hardware equipment.
In conclusion, introducing a CPOE system for chemotherapy prescriptions markedly decreased the number of errors recorded by the pharmacy service of our institution. The implementation of such a system seems to be a worthwhile objective for all hospitals and all categories of drugs.
Acknowledgments
We thank Bernard Testa, PhD, for critically reading this manuscript.
REFERENCES
Footnotes
-
Competing interests: None.