Article Text

Abstract
Objective: The epidemic proportions and management complexity of diabetes have prompted efforts to improve clinic throughput and efficiency. One method of system redesign based on the chronic care model is the Shared Medical Appointment (SMA) in which groups of patients (8–20) are seen by a multi-disciplinary team in a 1–2 h appointment. Evaluation of the impact of SMAs on quality of care has been limited. The purpose of this quality improvement project was to improve intermediate outcome measures for diabetes (A1c, SBP, LDL-cholesterol) focusing on those patients at highest cardiovascular risk.
Setting: Primary care clinic at a tertiary care academic medical center.
Subjects: Patients with diabetes with one or more of the following: A1c >9%, SBP blood pressure >160 mm Hg and LDL-c >130 mg/dl were targeted for potential participation; other patients were referred by their primary care providers. Patients participated in at least one SMA from 4/05 to 9/05.
Study design: Quasi-experimental with concurrent, but non-randomised controls (patients who participated in SMAs from 5/06 through 8/06; a retrospective period of observation prior to their SMA participation was used).
Intervention: SMA system redesign
Analytical methods: Paired and independent t tests, χ2 tests and Fisher Exact tests.
Results: Each group had up to 8 patients. Patients participated in 1–7 visits. At the initial visit, 83.3% had A1c levels >9%, 30.6% had LDL-cholesterol levels >130 mg/dl, and 34.1% had SBP ⩾160 mm Hg. Levels of A1c, LDL-c and SBP all fell significantly postintervention with a mean (95% CI) decrease of A1c 1.4 (0.8, 2.1) (p<0.001), LDL-c 14.8 (2.3, 27.4) (p = 0.022) and SBP 16.0 (9.7, 22.3) (p<0.001). There were no significant differences at baseline between control and intervention groups in terms of age, baseline intermediate outcomes, or medication use. The reductions in A1c in % and SBP were greater in the intervention group relative to the control group: 1.44 vs –0.30 (p = 0.002) for A1c and 14.83 vs 2.54 mm Hg (p = 0.04) for SBP. LDL-c reduction was also greater in the intervention group, 16.0 vs 5.37 mg/dl, but the difference was not statistically significant (p = 0.29).
Conclusions: We were able to initiate a programme of group visits in which participants achieved benefits in terms of cardiovascular risk reduction. Some barriers needed to be addressed, and the operations of SMAs evolved over time. Shared medical appointments for diabetes constitute a practical system redesign that may help to improve quality of care.
- SBP, systolic blood pressure
- SMA, Shared Medical Appointment
Statistics from Altmetric.com
INTRODUCTION
Background
Diabetes is a chronic disease whose epidemic proportions and management complexity threaten to overwhelm the acute care-oriented healthcare systems and individual primary care providers of today.1 Specialist expertise is limited, and waiting times are already afflicting the healthcare system, prompting efforts to improve clinic throughput and efficiency.2
One method to improve throughput and maximise efficiency is the Shared Medical Appointment (SMA) in which a multi-disciplinary team sees a group of patients (8–20) in a 1–2 h appointment. This system redesign, also called a “cluster visit” or “chronic healthcare clinic”, has been gaining popularity.3,4 While SMAs may be disease-specific or generic, chronic illnesses including diabetes, especially, lend themselves to the multidisciplinary approach.3–5 A recent review stated that: “Group visits are a promising approach to chronic care management for the motivated patients” and suggested that future research could benefit from more clearly defining the structure, processes of care, content of visits and appropriate outcome measures.6 In addition, there have been relatively few descriptions of actual implementation.
Problem addressed
Performance measures for the clinic related to quality of diabetes care showed significant gaps. In addition, patients with poor glycemic, systolic blood pressure (SBP) and/or LDL-cholesterol control are at the highest risk for cardiovascular morbidity and mortality, and represent a major challenge to individual practitioners and the healthcare organisation.5,7 Evidence of the practical treatment challenges is manifest in the difficulty translating evidence-based therapy into practice.5,8,9,10,11 For example, the UK Prospective Diabetes Study showed the difficulty maintaining patients at target level of A1c over time.12 The gaps in control of these other risk factors were also important to address.
Purpose of change
The purpose of this quality improvement project was to improve intermediate outcome measures for diabetes (A1c, SBP, LDL-cholesterol) focusing on those patients at highest cardiovascular risk. We desired to utilise the chronic care model of Wagner13 in designing a diabetes SMA, to implement this system redesign, and evaluate our performance while identifying lessons that could be applied to future projects.
SETTING
The setting was a primary care clinic at a tertiary care academic medical center in the Veterans Healthcare System, an integrated healthcare system, and has employed a variety of strategies including performance measures to improve the quality of diabetes care.14–17 This clinic provides care for 9500 patients including 2200 with diabetes. Primary care is provided by 60 Internal Medicine resident physicians, 8 part-time staff MD’s (Internists), and 5 full-time nurse practitioners. Thus, this setting must provide both care and training. Usual care includes referral to a dietician, certified diabetes educator or diabetes specialty clinic at the discretion of the primary care provider. Targeted patients included those with type 2 diabetes enrolled in the primary care clinic at the highest risk for cardiovascular morbidity, that is, did not meet diabetes performance measure targets, that is, had one or more of the following: A1c >9%, SBP blood pressure (SBP) >160 mm Hg and LDL-c >130 mg/dl (approximately 400 patients). Targeted patients received a letter from the Clinic Director informing them that they had suboptimal diabetes measures and inviting them to call the clinic for an appointment. When the patients called, they were informed that the visit would be a group visit.
Function of the clinic
In addition to having a sophisticated electronic medical record, aspects of the Chronic Care Model routinely integrated into this clinic include nurse case management and a clinical reminder system with feedback on performance. Prior to the implementation of SMAs, patients with diabetes and poor cardiovascular risk factor control were identified as they were seen for routine appointments. Patients were typically referred to a nurse case manager, PharmD or dietician for more attention and were occasionally referred to a subspecialty diabetes clinic. Thus, patients who had been referred to an individual could now be referred to a group. A registry was developed so that patients could be identified and contacted prospectively.
The clinic culture was characterised by a focus on individual responsibility of physicians rather than system-based practice, and there was relatively little interdisciplinary care. Improvement efforts previously were primarily top down based on mandates from the front office. The committee formed to address the quality of diabetes care was an outgrowth of a day-long clinic retreat conducted off-site. Clinic staff who previously had little involvement in system redesign began to take part. The improvement process was patient-centred and included patients in the initial design. Patient feedback is used in an ongoing basis for continuous improvement.
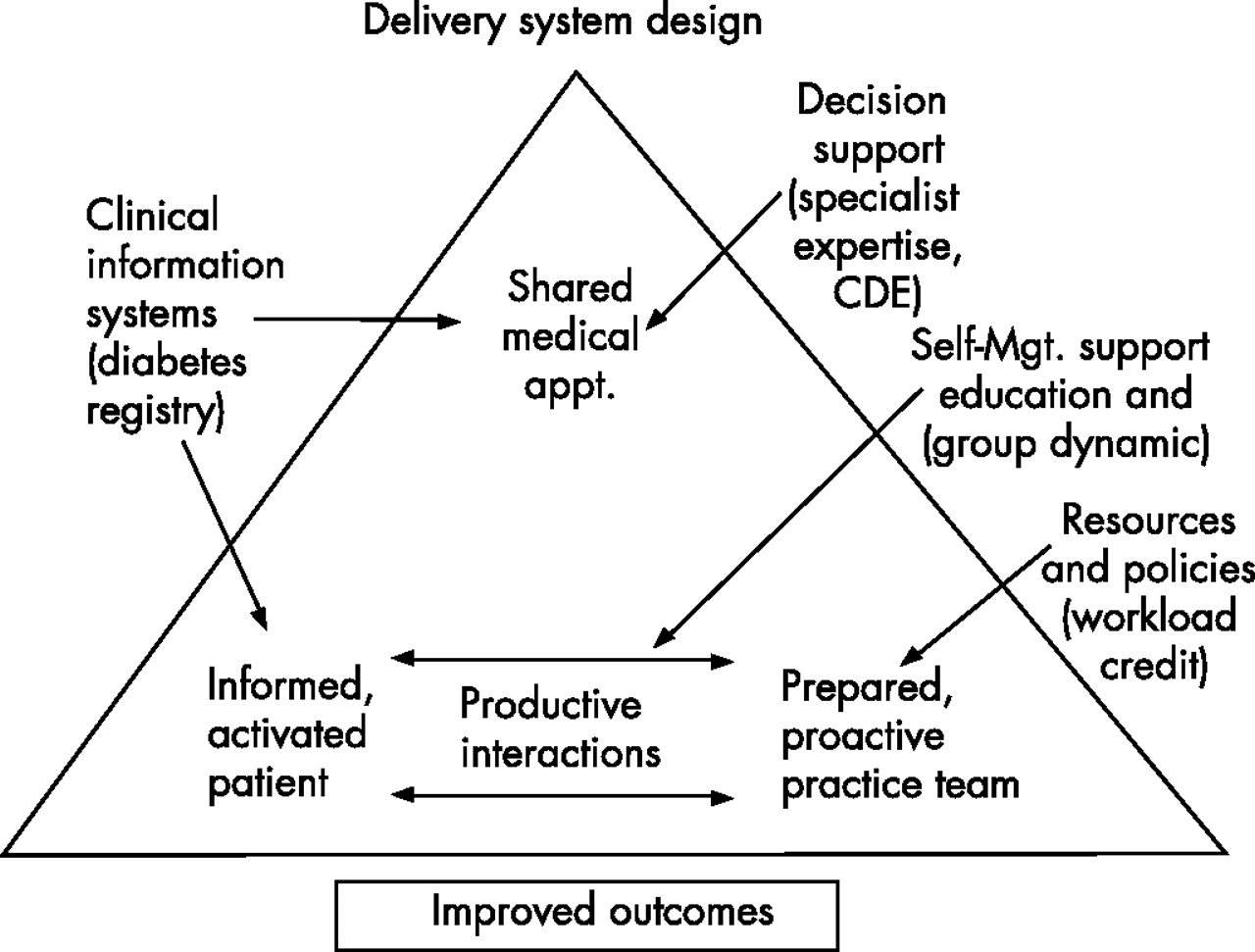
The conceptual model for our intervention, based upon Wagner’s chronic care model, is shown in fig 1. The SMA is a system redesign organised to foster productive interactions between informed activated patients and a prepared proactive team as well as peer support. We utilised the electronic medical record/clinical information system-based diabetes registry to identify target patients. Decision support (specialist expertise) was provided by VA/Department of Defense Diabetes practice guidelines, readily available on clinic computer workstations and by including a diabetes specialist in the team, a certified diabetic educator who is also an experienced diabetes nurse practitioner. Each patient who participated in an SMA interacted with a prepared proactive team comprising one general internist, one nurse practitioner, one pharmD, one clinical health psychologist and one nurse. There were no incremental personnel costs; the intervention involved personnel already assigned to the clinic. The delivery system redesign from traditional individual appointments to SMA allowed for greater self-management support. The process of informing and activating patients included didactic group education but also relied to a large degree on the group dynamic; patients were asked to be active participants in their care via participation in group and individual learning.
{kind=link}
Conceptual model for shared medical appointments. The delivery system design was the focus of the chronic care model that we changed. This figure demonstrates elements of the chronic care model we used in designing the SMA.
At each SMA, patients were apprised of their A1c, LDL-c, serum creatinine, SBP, use of aspirin, foot and eye examination status. This clinical information, and its importance to diabetic individuals, was displayed on a large flip chart, visible to all and discussed in the group. A facilitator reviewed goals for measures and assisted discussion regarding how self-management skills can improve these parameters. Patients were encouraged to ask questions of other patients and staff. Additional topics discussed included smoking, obesity, mood and erectile dysfunction, with emphasis on the relationship with diabetes. Through exchanging personal experiences, patients help others to understand sequelae of uncontrolled diabetes. Typical patient statements to group members included: “I never did pay attention to my diabetes until I had this kidney transplant” and “I have depression, and if I can exercise every day, so can you.” At conclusion of the SMA, each patient developed a behaviour-changing self-management goal and a specific plan for achieving diabetic goals, which was then documented in the medical record. Concomitantly, during the group process, patients were removed individually for medication adjustments as well as for discussion of issues where the patient preferred privacy.
We also integrated a quality improvement process into our model. After each SMA, the provider team debriefed and discussed how to improve clinic flow and efficiency. At first, patient medications were adjusted with group members present. A process re-evaluation and a system redesign occurred secondary to group-member lack of engagement. Allowing patients 5–10 min of individual provider (MD, NP, PharmD) time allowed for better patient feedback, and clearer provider instruction and plan. Individual time also allows for a clear individualised plan that patients take home
METHODS
Measures
Quantitative data included intermediate outcome measures (A1C, LDL-c, SBP); qualitative data were obtained from both patients and staff.
Analytical methods
Our initial study design was a pretest–post-test design. However, because of the concern that improvement in intermediate outcomes could reflect regression to the mean rather than true improvement, we identified a comparable series of control patients, thus changing the study design to a quasi-experimental study with non-randomised concurrent controls. Intervention subjects included all patients who participated in at least one SMA from 4/05 to 9/05. Control subjects included all patients who participated in at least one SMA from 5/06 to 8/06. Baseline measures for the intervention group were obtained prior to the initial SMA. The follow-up measures were obtained by using the values nearest to 8/06. For the control group, baseline measures were obtained by using the oldest time point close to 1/05. The follow-up measures utilised the last values prior to the SMA. Thus, in this retrospective analysis of the controls, only data obtained prior to their participation in an SMA were utilised. Paired t tests were used to evaluate the impact of the intervention on A1C, LDL-c and SBP within groups, and independent t tests were used for between-group comparisons. Changes in the percentage of patients meeting targets were analysed using χ2 or Fisher Exact tests. Baseline differences between groups for dichotomous variables were assessed with χ2 tests. Because the patients were distributed among a large number of primary care providers and because patients participated in a variable number of SMAs with constantly changing group composition, we did not use cluster analyses. All analyses were conducted using SPSS Version 13 (Chicago). The study was approved by the Institutional Review Board.
Situation analysis
Fifteen years previously, the clinic underwent a major redesign with the development of a Firm System.18 However, the interprofessional collaboration and esprit de corps of the Firm System had deteriorated over time as the clinic expanded significantly and personnel, including leadership, changed. Although the clinic personnel understood themselves as part of a functioning, interdependent system, there tended to be focus on local optima rather than a system optimum and workload credit as opposed to system throughput. With a change in leadership and the burning platform of suboptimal performance, the impetus for change was present.
Our first experience with group visits was in the Gastroenterology Clinic, and this was to a preprocedure clinic. These visits not only appeared to be an efficient use of limited resources, but also were successful based on a reduction of no show rates for GI procedures. Implementation of SMAs was mandated as an organisational performance measure and was placed under the purview of a committee tasked with improving access to care and quality of care. Some of the authors are members (SK and DA). Thus, SMAs were consistent with both central and local organisational priorities. Because of the mandates, resources were made available to implement SMAs on a more widespread basis. In order to address deficiencies in meeting diabetes performance measure goals, a quality improvement team was established, focusing specifically on high-risk patients.
OUTCOMES
One hundred and twelve patients met entry criteria by the time the study phase of the project was completed in September, 2005. All were contacted by letter, and 44 agreed to participate (39%). Baseline characteristics of participants are shown in table 1. The mean±1SD age of the patients was 60.6±8.9 years, and all but one were male (97.7%). Patients participated in the following number of visits: 38.6% participated in one visit, 25.0% participated in two visits, 13.6% participated in three visits, 9.1% participated in four visits, 2.3% participated in five visits, 4.5% participated in six visits, and 6.8% participated in seven visits.
Baseline characteristics of the study population
Each group had up to 8 patients. At the initial visit, 83.3% had A1c levels >9%, 30.6% had LDL-cholesterol levels >130 mg/dl, and 34.1% had SBP ⩾160 mm Hg. Mean±1SD follow-up times (from initial SMA) in months were 10.8±3.6, 9.5±4.5 and 11.5±3.7 for A1c, LDL-c and SBP, respectively. To evaluate the programme, we first assessed for changes in the SMA participants. Levels of A1c, LDL-c and SBP all fell significantly postintervention with a mean (95% CI) decrease of A1c 1.4 (0.8, 2.1)% (p<0.001), LDL-c 14.8 (2.3, 27.4) mg/dl (p = 0.022) and SBP 16.0 (9.7, 22.3) mm Hg (p<0.001). The proportion of patients meeting targets rose for A1c (16.7% preintervention vs 52.4% postintervention, Odds Ratio (95% CI) (0.78, 65.5) (p = 0.096 Fisher Exact Test), LDL-c (69.4% vs 83.3%, OR 6.6 (1, 43.8) (p = 0.057) and SBP <130 mm Hg (18.2% vs 43.2,OR 14 (1.5, 127.2) p = 0.014). Because aspirin is an over-the-counter medication whose cost may be less than the patient’s copayment so that aspirin might not appear in the patient’s medication list, we performed a chart review. Of those eligible to take aspirin, 88.4% had been prescribed at baseline, and 97.7% received prescription at the SMA.
We next assessed for differences between the participants and the control subjects. There were no significant differences at baseline between control and intervention groups in terms of age, baseline intermediate outcomes or medication use (table 1). We then assessed for an intervention effect. The reductions in A1c and SBP were greater in the intervention group relative to the control group: 1.44 vs –0.30% (p = 0.002) for A1c and 14.83 vs 2.54 mm Hg (p = 0.04) for SBP. The LDL-c reduction was also greater in the intervention group, 16.0 vs 5.37 mm Hg, but the difference was not statistically significant (p = 0.29). Differences in proportions of control patients meeting targets at baseline versus last measurement prior to SMA participation were not statistically significant for A1c (35.5% vs 45.2%, p = 0.153) and LDL-c (80.8% vs 65.4%, p = 0.057). The proportion of patients meeting the target of SBP <130 mm Hg decreased (26.5% vs 17.6%, p = 0.031).
The quality improvement project evolved. Additional clinic flow redesign occurred—for example, the order of tasks such as blood pressure measurement and foot examination. Patients now have these measures obtained in individual rooms when pulled out of a group as opposed to completion at check-in to the clinic; the latter caused delays in patients joining the group. The documentation process has also changed. Initially, clinic notes were entered into the electronic medical record at the end of the SMA. Currently, the SMA staff writes a templated note in which data are automatically downloaded into the registry when patients are seen individually.
DISCUSSION
Summary
We were able to initiate a programme of group visits in which participants achieved benefits in terms of cardiovascular risk reduction. Some barriers needed to be addressed. Concern was expressed by participating staff that because they did not see each patient individually, they could not appropriate credit for their work. Essential to their “buy-in” was the development of a mechanism to ensure workload credit. Additionally, other clinic providers were invited to observe SMAs in order to learn the process to increase comfort in recommending that their own patients attend. Primary care provider observation and participation in 1–2 SMAs were an opportunity to enhance provider skills in diabetic care, spread knowledge and increase referrals of patients who were at high risk for reasons not identified in registry data.
Context
SMAs have shown efficacy similar to or better than usual care, although positive results are by no means universal.19 A systematic review of self-management strategies for lowering A1c levels found effect sizes between 0.5 and 1%.20 Other types of system interventions—for example, nurse case management—have had comparable effect sizes.21–23 Our results are comparable and were achieved in a system of healthcare that already utilises many aspects of the chronic care model and has a robust performance measurement system for diabetes.
Interpretation
Several observations about the SMAs are noteworthy. The reduction in A1c by an average of 1, although modest, is clinically significant in terms of cardiovascular risk reduction. Some of the success may be attributable to the debriefing and refining after each SMA. In many ways, our interdisciplinary, prepared proactive team functions as a high-performing team.24 For example, all team providers have participated as group facilitators. Providers teach each other their expertise. In this way, the providers’ interactions are viewed as powerful agents of behaviour change toward self-management (for themselves as well as for the patients). This suggests that SMAs may be a useful venue for training other healthcare professionals in the disciplines of psychology, nursing, pharmacy and medicine. Patients benefit from the team approach by receiving care in different ways from different providers. Communication styles differ among health professionals, thereby enhancing patient education and engagement. We speculate that the team approach, the emphasis on patient self-management and patients themselves offering successful lifestyle management strategies have contributed to the success in these high-risk patients.
Within the “high-risk” patient group, there are several potential subsets of patients. There are patients in whom the system or the providers have not been able to optimally care for in a timely or aggressive enough manner, that is, the patients may be motivated, but the system has not provided good enough care to achieve target goals. There are also patients who have obtained good care, but were not sufficiently motivated to achieve the targets. Some of these high-risk and “non-adherent” group have become more engaged in their diabetes care via the peer support, team care and promotion of increased self-management by SMAs. A minority of patients come to one visit and do not become engaged in their care or never return to the SMA despite follow-up phone calls.
We also recognise that billing is less of an issue in the VA so that the difficulties of billing under a single physician’s name for a shared medical appointment with multiple patients in a group are basically irrelevant. While SMAs may or may not be efficient from a billing perspective depending upon the specific billing rules, SMAs can be very efficient in terms of productivity, In fact, this intervention did not involve incremental personnel costs. We kept group size relatively small at the initiation of the project, but we anticipate that with more experience, we can increase the number of patients per group, increasing the efficiency of resource utilisation.
Because our intervention involved a subset selected based on high baseline levels of A1c, SBP and LDL-c, our initial choice of a simple pretest–post-test design was problematic because of the phenomenon of regression to the mean. Regression to the mean is a pervasive statistical phenomenon affecting repeated data that can make natural variation in repeated data look like real change.25,26 Unusually high (or low) measurements tend to be followed by measurements that are closer to the mean. Although there are some statistical methods that can assess for regression to the mean, better study design represents the preferred approach. Quality improvement projects often target more affected subsets and usually lack control subjects. The inclusion of controls for what was started as a quality improvement project raises the issue of where one draws the line between quality improvement and research.27 However, we ignore this statistical phenomenon at our peril, lest we make and then act upon erroneous conclusions about the effect of our improvement efforts.
Limitations
Our study has a number of limitations. The sample size was relatively small and was carried out in a single facility by a single group of facilitators and, as a new project, could be subject to the Hawthorne effect. Thus, it should be considered a pilot project. Allocation to group was not randomised. This study took place in a context in which there are several efforts under way to improve diabetes care, so that the influence of secular trends cannot be excluded. However, because the control subjects all participated in an SMA, albeit later, had similar baseline characteristics, and had a concurrent period of observation prior to their SMA participation, they would seem to be comparable. Intervention patients participated in different numbers of visits. In fact, there were no two group visits with the exact same patients. We relied upon usual clinical practice for the blood tests. Thus, there was a variable period of follow-up data, and a few patients did not obtain postintervention lab tests. We have also not accounted for additional costs related to increased medication use, supplies, lab testing and consultations, but these should be part of good medical care. We have not surveyed patients who declined to respond to the invitation to make a clinic appointment. Our study involved a population of veterans, and we can speculate that the camaraderie that develops among veterans could have impacted the group dynamic, raising issues of generalisability.
CONCLUSIONS
Notwithstanding the project’s limitations, we have shown the feasibility of implementing effective shared medical appointments using a group interdisciplinary team approach to care for motivated high-risk patients with diabetes. Shared medical appointments for diabetes constitute a practical system redesign that may help to improve quality of care. This approach has accommodated even some of those who had previously been labelled as “non-compliant” and who would benefit greatly from lowering their high cardiovascular risk. Our results were promising enough to expand the use of SMAs to other chronic conditions—for example, hypertension and congestive heart failure. In addition, we have included SMAs in the ambulatory block curriculum for internal medicine trainees and the chronic disease advanced core clerkship for medical students. Future studies will be required to identify the “physiology” of SMAs to elucidate further what about them accounts for the clinical improvement seen.
Acknowledgments
This quality improvement project was undertaken in the context of our participation in the AAMC/RWJ-sponsored Academic Chronic Care Collaborative which began in June 2005. Funding: VA HSR&D grants to DA (REA 01-100). We thank Mr Scott Bieschel for management of the diabetes registry, Ms Stacey Hirth for data collection, Ms Michelle Davidson for manuscript preparation and Dr Katherine Thweatt for her assistance.
REFERENCES
Footnotes
-
Competing interests: None declared.
-
Presented in part at the Scientific Symposium of the Institute for Healthcare Improvement National Forum, Orlando, December, 2005.
The views expressed are solely those of the authors and do not necessarily reflect the views of the Department of Veterans Affairs.
Linked Articles
- Editorial
- Quality Lines