Article Text

Abstract
Introduction: Suboptimal communication between health professionals has been recognised as a significant causative factor in incidents compromising patient safety. The use of a structured method of communication has been suggested to improve the quality of information exchange. The aim of this study was to determine if the teaching of a communication tool, ISBAR (Identify, Situation, Background, Assessment, Recommendation), a modification of SBAR (Situation, Background, Assessment, Recommendation), improved the content and clarity of a telephone referral in an immersive simulated clinical scenario conducted in real time.
Method: Seventeen teams of final-year medical students were randomised into two groups. The intervention group participated in a 40 min education session about the ISBAR communication tool. A control group received no training. Each team of five students participated in a simulated clinical scenario using a patient simulator in a mocked-up clinical environment. During each scenario, one student made a telephone referral seeking assistance from a senior colleague. Audio data for the telephone referrals (n = 17 students) were captured during the scenario for both groups. During a blinded review of the data, communication was scored on both content and clarity.
Results: Communication content was higher from a mean score of 10.2 to 17.4 items (p<0.001) with the intervention. Clarity of the delivery of information on a 5-point scale was also higher in the intervention group (ρ = 0.903, p<0.001).
Conclusions: The teaching of a structured method of communication improved the communication during telephone referral in a simulated clinical setting. This research has implications for how healthcare professionals are taught to communicate with each other.
Statistics from Altmetric.com
Modern healthcare has been described as a “complex socio-technical system.”1 In addition to the highly technological nature of the work, coordination of activities often involves a complex social network of individuals often with differing backgrounds, training and viewpoints. The members of the multidisciplinary team of doctors, nurses and allied health professionals looking after a particular patient are often separated from each other both in time and space as they go about the work of caring for the patient. Furthermore, in a hospital environment, the members of this team change many times during the patient’s treatment. A crucial component of successful coordination of teamwork is effective communication within the team.2–5
Communication failures have been estimated to be a major factor in 60–70% of serious incidents.67 The patient’s current state may not be adequately conveyed between team members, and future events or goals are not anticipated or explicitly stated during the transfer of information.78
In other industries in which communication failures can have serious consequences—such as aviation, rail and the military—one safety initiative has been the use of standardised communication during the transmission of information. Advantages of such an approach may be that novices benefit from using a predetermined structure to reduce the omission of important information, and there is an expectation on the part of the recipient of the order in which information is given.9–11
One structure that has been suggested to improve communication is the situational briefing tool, SBAR (Situation, Background, Assessment, Recommendation).12 This tool was developed by the US Navy for standardising important and urgent communication in nuclear submarines. The Institute for Health Improvement (IHI) has recently suggested that SBAR be the model that health providers use to structure clinical communication.13 To date, no published data exist on the effectiveness of the tool to improve instances of real life or simulated clinical communication in healthcare. The aim of this study is to determine if the learning and practice of a modified version of this tool improves the transfer of clinical information in a standardised clinical scenario in a simulation environment.
METHOD
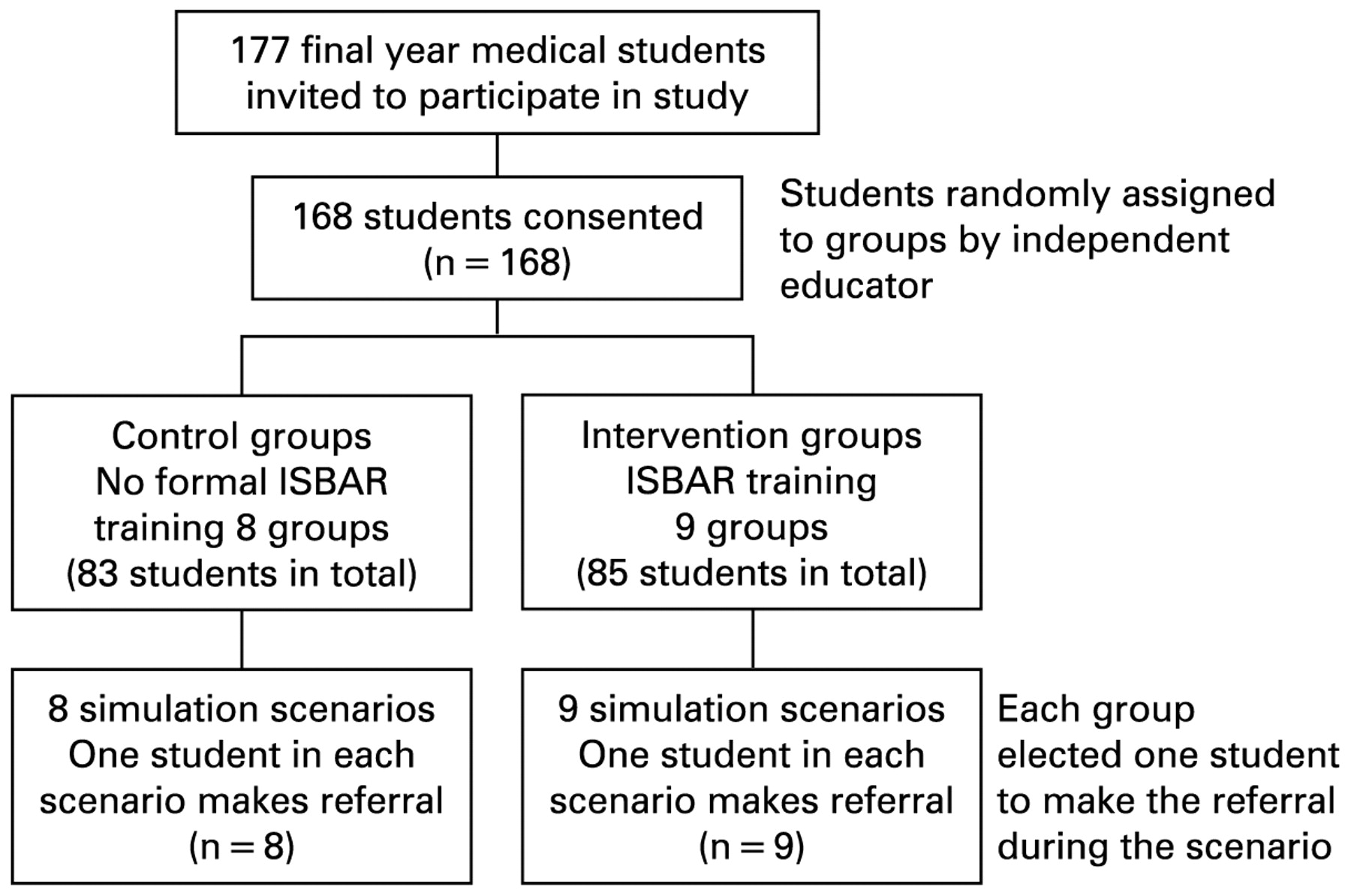
After institutional ethics committee approval, a trial was undertaken, involving 177 final-year medical students enrolled in an existing education programme on patient safety. After allocation by an independent educator not involved with the trial, half of the students undertook an ISBAR education session prior to participating in a standardised simulation scenario using a patient simulator in a replicated clinical environment. The other half of the students acted as a control group with no structured teaching of the ISBAR (Identify, Situation, Background, Assessment, Request) tool prior to undertaking the scenario (fig 1)—this group received the ISBAR education session after their simulation session. The scenario involved the management of an unstable 34-year-old male trauma patient (box 1). As part of the briefing to the scenario, students were informed that they had the option of calling for more senior help via the telephone.

Representation of the study design and participant numbers. ISBAR, Identify, Situation, Background, Assessment, Recommendation.
Box 1 Summary of tasks performed by teams in scenario
Receive handover from paramedic
Assess patient—airway, breathing, circulation
Plan and coordinate management
Give supplemental oxygen
Obtain intravenous access and take blood
Initiate fluid resuscitation
Request help via telephone from senior doctor
Administer blood products
Request and interpret radiology
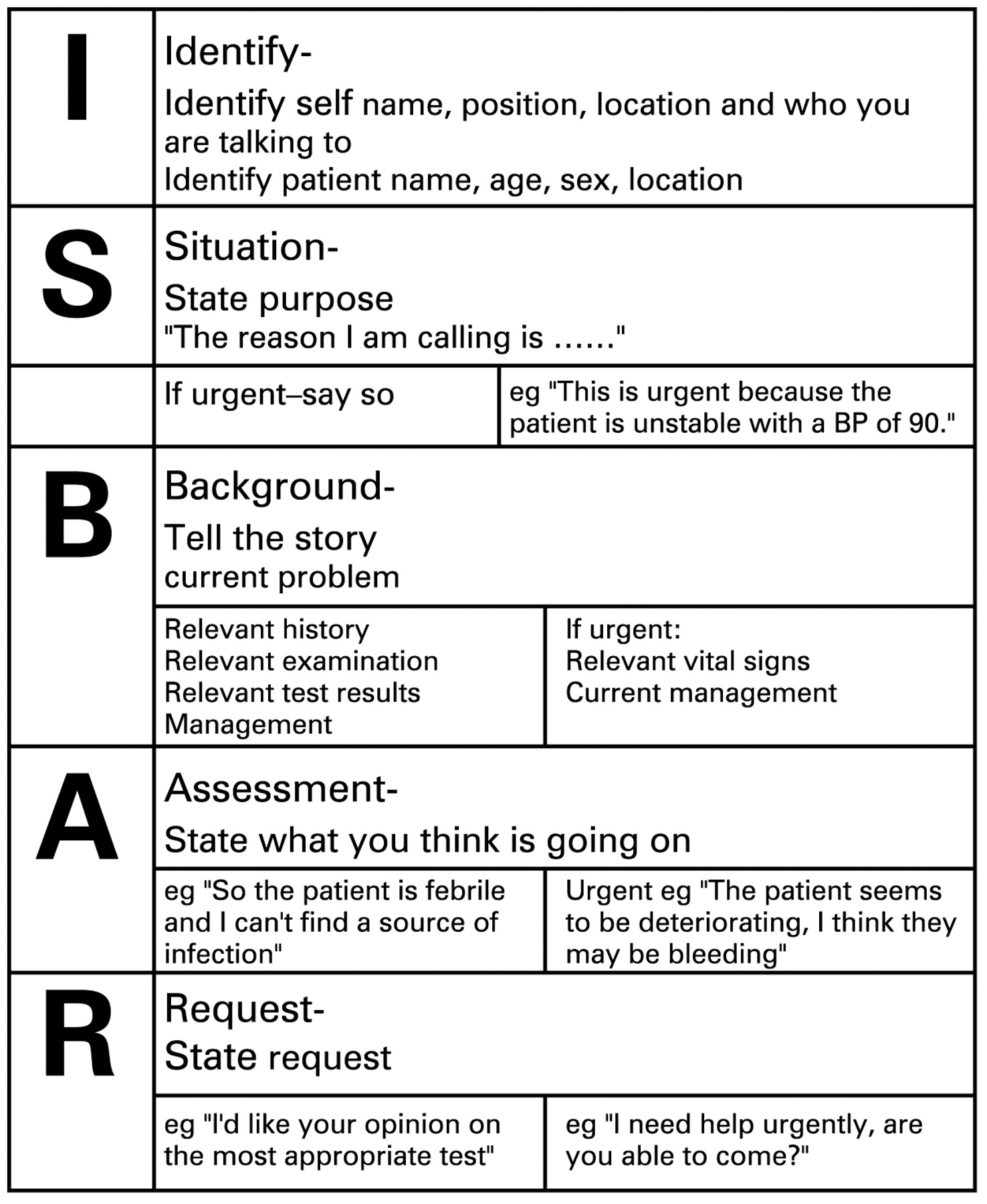
The situational briefing tool used was adapted from “SBAR” to “ISBAR” with the separation out of “Identification,” one of the subelements of “Situation,” into its own category. “Identification” refers to identification of self, the person to whom the information is being given, and the patient under discussion (fig 2). This adaptation was in response to a number of reports from the workplace and observation of performances in a simulated environment, in which the absence of explicit declaration of identity and location led to confusion in this regard.

{kind=link}
{kind=link}
ISBAR tool.
The 40-minute small-group teaching session consisted of: group discussion on the importance of effective communication during telephone referrals; critique of trigger videos of suboptimal telephone referral; introduction of the ISBAR tool; video demonstration of ISBAR in use; and paper-based scenarios and role plays in which all students practised using the tool.
In all of the recorded simulation scenarios, one of the investigators acted as the senior clinician receiving the telephone referral but was not blinded to the intervention by virtue of the timing of the education during the day. In order to standardise the interaction, the investigator was not able to visualise the students within the scenario, and provided minimal prompting to the students during their referral over the telephone. Video and audio recordings of the consenting students were taken during the scenarios using unobtrusive techniques. The recordings were identified with a unique code and given to two blinded observers at the completion of the study period to score the communication. A 20-item scoring sheet (listed in table 1) was used to identify the presence or absence of important aspects of content of the students’ telephone communication and the clarity. The scoring system was based on a score sheet previously developed by the investigators to formally assess final-year medical students’ telephone communication skills, as part of their end of year assessment. A global rating was also given, using a five-point scale (box 2). Primary end-points were the number of items mentioned on the 20-point list, and global rating scores of the communication. Inter-rater reliabilities for each item and the global rating score were analysed using Cohen kappa statistics.
Box 2 Global Rating Score for overall communication
1 mark: Requires frequent prompting, no economy of words, speaks too quickly, or pauses rarely, not structured or clear. Uncertain urgency.
2 marks: Requires significant prompting, recognises important aspects but includes irrelevant information. Urgency unclear.
3 marks: Some prompting required, concise at times, hesitant or too rapid periodically. Some logical order.
4 marks: Occasional prompting needed. Appropriate pace and pauses. Understanding of patient’s state, urgency and likely diagnosis. Some confusion about action required.
5 marks: Reasoned, coherent and concise delivery. No prompting needed. Pauses appropriately and clarifies (closes the loop).
RESULTS
From a possible 18 groups of students, 17 groups consented to take part in the study. The 168 students were allocated into groups of 10–12. For each group, five students (range 4–6) actively participated in the study scenario while the remainder observed the scenario. Eight participant groups acted as control groups, having no prior formal training on the ISBAR tool. The other nine groups undertook the teaching session on the ISBAR tool as previously described, as part of a lecture session 2–4 h before the simulation scenario. In all of the scenarios, one of the students (from the group of five active participants) called for help by means of a telephone referral to a “senior clinician” (actually one of the investigators).
Intercoder reliability
Two independent coders observed data from the first 10 of the 17 scenarios. The reliability of the individual items ranged from kappa values of 0.55 to 1.0 (table 1) with a mean of 0.87 (SEM = 0.038). Absolute agreement was obtained (K = 1.0, p<0.001) between the two observers on the five-point Global Rating Scale of clarity and delivery of communication. Once reliability had been established by having two coders rate the first 10 scenarios, one coder reviewed the remaining seven recordings.
Use of the ISBAR tool
The students in the groups who undertook the ISBAR education session prior to the scenario scored higher than students in the groups whose ISBAR education session was after the scenario. The intervention demonstrated higher total item scores from a mean of 10.2 to 17.4 (p<0.001) (table 1). Similarly, the clarity of the telephone communication was rated higher on the 5-point global rating score (Spearman rank correlation ρ = 0.903, p<0.001).
DISCUSSION
This study describes the positive effect of teaching ISBAR, a structured method of communication for telephone referrals, on students’ ability to make a clear referral in an immersive simulated clinical scenario shortly after a teaching session on ISBAR. The study population consisted of a very junior group of clinicians in which it would be expected that focused communication of important clinical detail might be lacking. This study does not validate the ISBAR tool as a method to improve the clarity and precision of communication in the real world; for that, an observational study based on actual clinical communication would be required. Nevertheless, it should be recognised that the major challenge of attempting to conduct such studies in the real world is the inability to standardise both the clinical situation and the conversation at the other end of the telephone. The strength of this study is the replication of the working environment as closely as possible with all its inherent uncertainties and complex nature, while maintaining a standardised interaction to assess. As would be the case in the real world, the simulation scenario required students to gather, interpret, process and organise clinical information in a dynamic, evolving situation, and manage distractions, clinical uncertainty and competing demands on attention and time. These elements of the simulation increase the relevance of our results to the work place and hence, in our view, strengthen the case for the applicability of the ISBAR tool in the real world.1415
Despite the many similarities between the simulation and the real-world environment, there are still many work place conditions that are difficult, if not impossible, to reproduce in a simulation. In the simulation environment the focus is on learning, but in the real world the consequences of one’s actions (and inactions) are much higher. This difference in the stakes may affect communication. In the real world, the communication of the person on the receiving end of a telephone referral is unpredictable and may not always be conducive to using ISBAR. Clinicians receiving referrals may interrupt, have varying degrees of helpfulness, may question, prompt or lead the conversation and may be unfamiliar with the ISBAR method.
The complex nature of the scenario also provided an opportunity to minimise performance bias, as the referral was just one of many communication activities students engaged in during the scenario. Although informed consent was obtained as to the nature of the study regarding the measurement of effectiveness of communication, the students were unaware that the telephone referral would be the research focus. Given that the students were not primed to request advice, but in each case did so, it suggests they were genuinely motivated to seek help in the scenario. It may be reasonable to speculate that under such circumstances, the students’ motivation to be as effective as possible with their telephone communication was high. If so, the significance of the results in this study is more pronounced.
We deliberately did not allocate the task of telephone referral to a particular student in the scenario, as all task allocation during the scenario was determined by the students. To do so would have been otherwise disruptive and may have highlighted the phone call as the purpose of the study. The student who made the telephone referral was usually one who was not involved in a technical task (see box 1) at the time that the referral was deemed necessary by the team. As this occurrence was seemingly entirely opportunistic, we have no way of knowing to what extent the callers constituted a biased sample of students in terms of ISBAR communication skills, but the situation was the same for both the control and intervention groups.
The item-based scoring system we developed to test the effectiveness of communication was originally derived from ISBAR and as such could potentially bias our results to favour the ISBAR trained group. Ideally, the system used to score the communication would be entirely independent of the communication tool. Unfortunately, there is no “gold standard” alternative to measure such interactions. The marking scheme underwent multiple iterations and revisions prior to its use that have separated it somewhat from the initial tool. The face validity of our scoring system is high, and improvements on the global rating score, which is not related to any of the items on the ISBAR tool, suggest that the overall effect is not merely a measurement bias.
Another constraint of this study is the short time of 2–4 h between ISBAR training and the simulated clinical scenario. Ideally the effects of an educational intervention are measured serially to determine consolidation or decay of learning over time. Following the simulation, students were provided with a lanyard card to assist and encourage the use of ISBAR when making referrals in their subsequent clinical placements. Many junior doctors, who had ISBAR training the previous year, continue to wear the lanyards and attest to the usefulness of the ISBAR tool.
This is the second year we have taught ISBAR to final-year medical students. A potential bias is that a number of our study participants had already heard of ISBAR, presumably from students in the year ahead, though none of the study participants had previously participated in a focused training session.
This study supports the contention that training in the use of ISBAR is feasible, effective and likely to result in improved communication in the clinical environment by junior clinicians when making telephone referrals. Fully immersive simulation scenarios have provided a controllable yet realistic environment to measure effects of ISBAR training. Further research into real-world performance and utility of the tool is warranted given the potential for widespread implementation and improvement in communication between healthcare clinicians. This work may also inform the development of structured communication tools for use in other identified high-risk periods such as during handover at the end of a shift as well as written communication in clinical notes.
Acknowledgments
The authors wish to acknowledge the Coordinators and Teaching faculty at the Southern Health Simulation and Skills Centre for their assistance with data collection, and to R Meek and J Griffith for statistical advice.
REFERENCES
Footnotes
Competing interests: None.
Ethics approval: Ethics approval was jointly approved from the Southern Health and Monash University Human Research Ethics Committees.
Patient consent: Obtained.
Linked Articles
- Quality lines