Article Text

Abstract
Introduction: Hospital-acquired venous thromboembolism (VTE) is a potentially fatal complication of hospitalisation, with meta-analyses and guidelines supporting the use of proven prophylactic measures (graduated compression stockings (GCS) and anticoagulants). Despite this, prophylaxis is underutilised and represents one of the largest gaps between evidence and current clinical practice.
Methods: All episodes of VTE complicating hospitalisation were ascertained prospectively as part of a quality improvement programme over 3.5 years with a view to designing interventions to improve the use of prophylaxis and reduce the rate of VTE. Interventions initially centred upon highlighting the burden of VTE, the extent of failure to apply guideline evidence into practice, and the development and application of a hospital-wide risk assessment tool. Later interventions sought to build the risk-assessment tool into routine clinical care and enhanced feedback on VTE to clinical teams.
Results: The annual rate of VTE fell in all the years following the intervention (2001), from 2.57 per 1000 cost-weighted separations to a nadir of 1.87 in 2003, with the difference being statistically significant (RR 0.68, 0.47 to 0.99, p = 0.04). The proportion of patients receiving anticoagulant prophylaxis increased (48% to 74%, p = 0.01) but there was no change in the measured use of GCS. There was a marked increase in the use of risk assessment for VTE in the ward setting (7.7% to 100%, p<0.001) during the programme.
Conclusion: Affordable and accessible interventions can improve the application of VTE prophylaxis guidelines into daily hospital care and are associated with reductions in this potentially life-threatening complication.
Statistics from Altmetric.com
Venous thromboembolism (VTE) is a well-recognised complication of hospital admission,12 with hospitalised patients described as being at 100 times greater risk than people in the community.2 Far from being a benign disease, pulmonary embolism constituted almost 5% of deaths in a longitudinal Swedish study3 and was seen in 31% of one series of autopsies in surgical patients;4 and in patients dying from pulmonary embolus having an autopsy, the diagnosis was not suspected ante-mortem in around 70% of patients.56 A recent UK Parliamentary report7 suggested that up to 25 000 deaths per annum arose from thromboembolic disease complicating hospitalisation alone, outstripping the mortality from road accidents, breast cancer and HIV/AIDS combined.
Measures to prevent VTE have been well studied, with meta-analysis level evidence that graduated compression stockings8 and heparin, in unfractionated and fractionated forms,9 are highly effective, producing risk reductions in the range of 40–80%. The evidence for mechanical pumping devices is less clear.8 Arising from this evidence has been the development of a number of guidelines for the prophylaxis of VTE, including an International Consensus Statement,10 the American College of Chest Physicians guidelines11 as well as national working parties in various countries, including Australia.1213 Published retrospective medical record reviews and the UK Parliamentary Report have highlighted the fact that these guidelines are not being applied.7141516
This programme originated from a coronial enquiry into the death of a patient from VTE who was considered to have not received adequate VTE prophylaxis, along with ongoing concerns from senior staff at The Canberra Hospital (TCH) regarding the adequacy of use of such prophylaxis across the hospital. This programme ran between June 2001 and March 2005, with the primary objective being to increase the use of VTE prophylaxis that was consistent with consensus guidelines using a series of interventions, with the hope that this would also reduce the incidence of VTE complicating hospitalisation at TCH.
Methods
TCH is the largest tertiary teaching hospital within the Australian Capital Territory (ACT), servicing Canberra (∼300 000 people) and a large surrounding rural area. Staff from the Clinical Health Improvement Programme (CHIP), a quality improvement Unit, managed this quality improvement project across TCH, with the assistance of a project team involving a respiratory physician and an intensive care specialist.
Data collection
The project first sought to capture all diagnoses of VTE arising from hospitalisation in TCH. Due to the nature of health services within and around the ACT, it was felt that the vast majority of VTE is diagnosed or managed at TCH rather than surrounding centres. Quality improvement staff attended the Medical Imaging Department of TCH at least weekly to ascertain all radiological studies performed as an investigation for a possible diagnosis of VTE (eg, lower limb venous Doppler studies, Nuclear Ventilation:Perfusion studies, CT Pulmonary Angiograms). The reports of all these studies were reviewed, and those that were positive or equivocal for VTE recorded. The medical records of all patients with a positive or equivocal test result were reviewed, and if the patients were treated for VTE by the clinical team they were deemed as having VTE and a datasheet initiated.
If the patient was an inpatient in TCH at the time or had been within 60 days prior to the diagnosis of VTE, they were considered as having hospital-acquired VTE. In such cases the review of the record was more extensive, with completion of the datasheet recording the clinical context, up to three risk factors for VTE, details of recent hospitalisations, the documentation of an assessment of patient risk for VTE, calculation of the number of days during which the patient was at risk (inpatient days only), along with the number of days of use of graduated compression stockings (GCS) and heparin (either unfractionated or low molecular weight) or therapeutic anticoagulation. Contraindications to the use of prophylactic measures at any point during the admission were recorded. Where possible, all data were collected prospectively, and medical record reviews were completed during the patient’s admission.
This medical record review was done by experienced nursing staff from the CHIP with all completed datasheets reviewed by the same three staff (two nursing, one medical) over the 3.5 years of the study. Prophylactic treatment for the majority of a hospitalisation in high-risk patients was defined as treatment for ⩾66% of the “at-risk” days. Following review, the data were entered into an Access database (Microsoft, Redmond, Washington).
Statistics and ethics
The ACT Human Research Ethics Committee agreed that this project satisfied the Australian National Health and Medical Research Council criteria for a quality improvement project that did not require formal independent ethical review.
In order to adjust for the activity and acuity of patients admitted to TCH during the study period, incidence of VTE figures are divided by the total of cost-weighted separations (CWS, or casemix-adjusted separations). This figure of total CWS is derived by adjusting all separations following coding using the International Statistical Classification of Disease and Related Health Problems (10th Revision), Australian Modification (ICD-10-AM).17
Data on the incidence of VTE are presented over time, with comparison of proportions using χ2 statistics. Comparisons of non-parametric data were made using the Mann–Whitney test. Analyses were performed using Epi Info (US Centers for Disease Control and Prevention) with differences at p<0.05 considered statistically significant.
Interventions
Interventions were made during the course of the project in response to the data and feedback from clinicians. The initial interventions (table 1) included presentations across the hospital at Grand Rounds, Junior Medical Officer Education Sessions and individual Unit sessions to highlight the burden of disease and the extent of under use of prophylaxis. A whole of hospital Deep Venous Thrombosis and Pulmonary Embolus Risk Assessment Tool (fig 1) was developed in both poster and portable card form, the latter version being distributed to all junior medical staff. This tool formed the basis of subsequent measurement and reporting on the use of VTE prophylaxis.
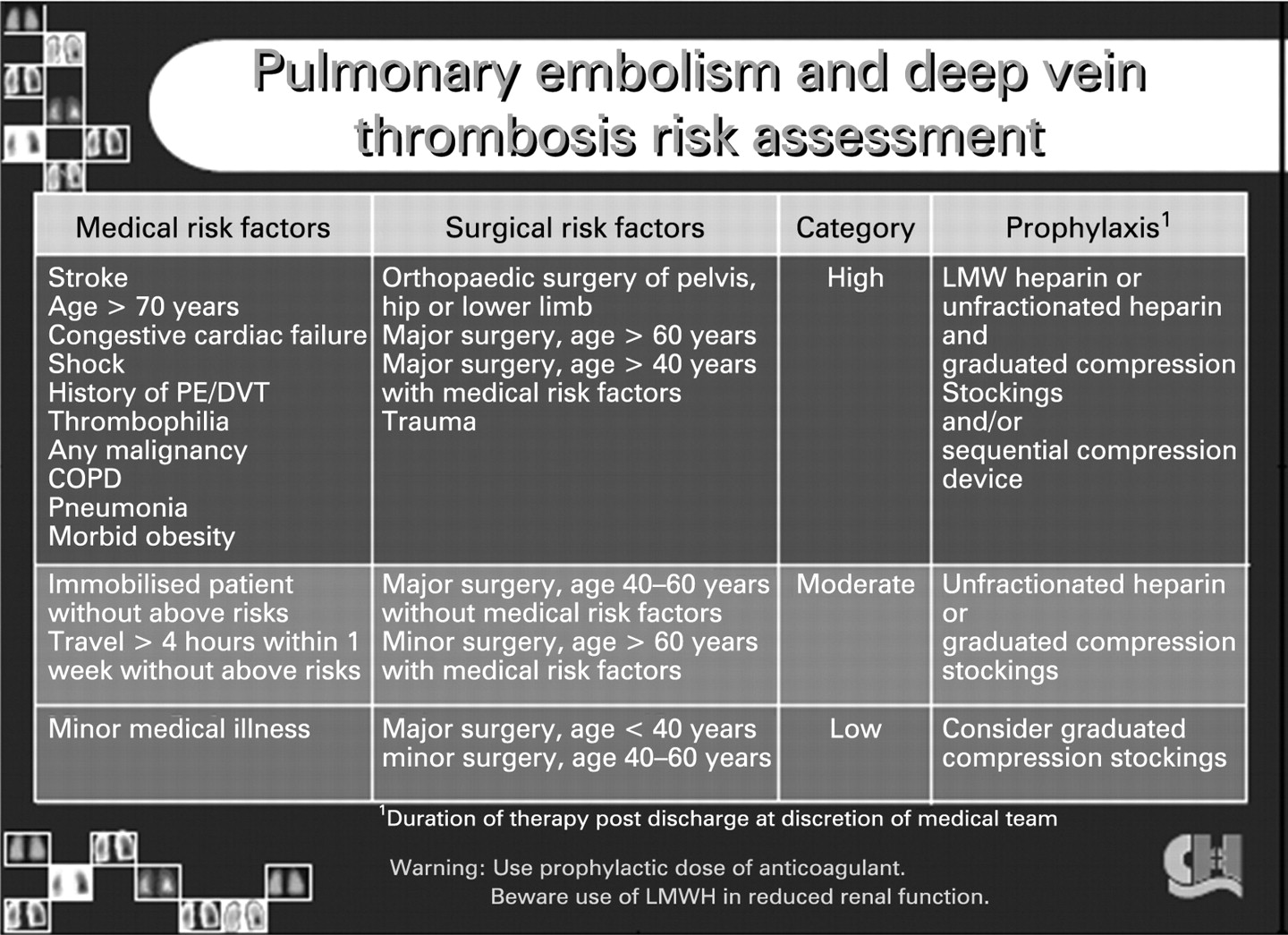
Pocket card risk-assessment tool introduced as part of the project. COPD, chronic obstructive pulmonary disease; DVT, deep venous thrombosis; LMW, low molecular weight; LMWH, low-molecular-weight heparin; PE, pulmonary embolus; VTE, venous thromboembolism.
Summary of interventions employed during the project
Later interventions were designed to build the use of the risk-assessment tool into routine clinical practice, most notably into the Nursing Care Plans and the Observation Charts of the hospital. Another deficiency in VTE care, which was highlighted in the UK Parliamentary Report,7 was the absence of feedback to the initial caring team when a patient previously under their care developed VTE. From early 2003, formal letters of notification were sent to the Attending Medical Officer and Head of Department when a patient developed a VTE having previously been under their care.
Results
The initial data collection documented a notable burden of VTE at TCH, with 46 cases in the first 6 months, of which over 50% (24/46) did not receive any compression stocking prophylaxis, and 54% (25/46) did not receive any anticoagulant prophylaxis. These data also highlighted the absence of clear policies within TCH to assess patient risk, to respond appropriately to that risk and against which to measure the performance of the organisation.
The vast majority (81%) of patients developing VTE were high risk for VTE on the basis of the hospital risk-assessment tool (table 2). The primary risk factors were similarly distributed between medical and surgical conditions (165 vs 144, table 3), highlighting the need to address the issue across the whole of TCH. Surgical risk factors, however, were more likely to be classified as the primary risk factor rather than a secondary risk factor (RR 1.55, CI 1.36 to 1.77, p<0.01).
Risk, contraindications and use of prophylaxis in patients with deep venous thromboembolism
Risk factors for venous thromboembolism (VTE) recorded throughout the project
In the index year, 2001, the mean monthly rate of VTE was 2.57 per 1000 CWS and lower in all the following years (fig 2A), 1.98 in 2002, 1.87 in 2003 and 2.17 in 2004. The reduction in the incidence of VTE was statistically significantly in 2003 when compared with 2001 (RR 0.68, 0.47 to 0.99, χ2 test, p = 0.04).

Changes in process measures over the duration of the project. (A) Quarterly rate of venous thromboembolism (VTE) per 1000 (blue line) with annual median rate (red line). (B) Percentage of patients who had a documented ward risk assessment for VTE (red line) and those where the risk assessment was performed by the project team (blue line) by quarter. CWS, cost-weighted separations.
Of the 285 VTE events that occurred in patients who were deemed as being at high risk for such an event, 32% (90 patients) had a contraindication to either anticoagulant or compression stocking prophylaxis recorded at any time during their admission (table 2). In the high-risk patients without a contraindication to the use of prophylaxis, there was a clear failure to deliver such prophylaxis for the majority of their time in hospital (table 2). Those high-risk patients without contraindication to anticoagulant prophylaxis had an average of 13.6 days at risk and received anticoagulant prophylaxis for an average of 8.3 of those days. In the analogous situation of high risk and no contraindication to GCS prophylaxis, patients had an average of 13.6 risk days and received prophylaxis for an average of 6.2 days. There was, however, a significant improvement in the extent of coverage of patients with anticoagulant prophylaxis as the project proceeded (fig 3A), with the proportion of patients receiving such prophylaxis for the majority of their hospital stay increasing from 48% to 74% between the first and last three-quarters of the project (p = 0.01). There was no appreciable increase in the use of GCS (fig 3B) in the high-risk patients with VTE during the project.

{kind=link}
{kind=link}
{kind=link}
Changes in use of anticoagulant and graduated compression stocking (GCS) usage over the duration of the project. (A) Percentage of “high-risk” patients with venous thromboembolism (VTE) who received anticoagulant prophylaxis for the majority (>65%, green bars) and minority (⩽65%, red bars) of their at-risk days in each quarter. (B) Percentage of “high-risk” patients with VTE who received GCS prophylaxis for the majority (>65%, green bars) and minority (⩽65%, red bars) of their at-risk days in each quarter.
There was also a profound increase in the use of the risk-assessment tool in the ward setting (fig 2B), rising from only 7.7% of patients with a VTE event having evidence of being risk assessed in the ward setting to 100% (RR 0.08, CI 0.01 to 0.51 p<0.001) in the most recent cases (first quarter of 2005).
Discussion
The largest challenge in the area of VTE prophylaxis remains the application of existing evidence into everyday practice. This project confirms the failure to implement the evidence seen elsewhere but also illustrates that interventions can improve the use of risk assessment and the use of prophylaxis, and in doing so may reduce the incidence of hospital acquired VTE. Fundamental to such improvement is a locally agreed policy on appropriate prophylaxis in each healthcare setting and measurement against this standard.
Despite giving rise to numerous guidelines,10111213 the VTE literature is limited in its ability to inform interventions that may improve the evidence–practice gap. Two studies have focused upon electronic and computer-based decision-support systems,1819 interventions that are not readily available in all settings and that require significant investment. One study of 15 short-stay hospitals20 has suggested that audit and education are effective, and a more recent systematic review advocated multifaceted interventions21 such as those employed in this project. At TCH, many of the barriers to improving VTE prophylaxis were only clarified when the data started being widely presented across the hospital, with ideas coming from staff about how to address the issues such as incorporation of the risk assessment into existing clinical forms.
One of the major difficulties in reporting and comparing hospital-based rates of VTE without randomised allocation is that the underlying burden of disease and clinical practices do vary over time, unrelated to project interventions. We have sought to reduce this by deriving an incidence ratio (episodes per 1000 CWS) based upon an international standard for hospital activity and acuity. This project also used medical, nursing and clerical staff in an active and prospective manner to detect and review all cases, rather than relying upon coding staff to detect cases. Attempting to detect all VTE cases is difficult and, in view of the robustness of the evidence for VTE prophylaxis, it is debatable whether the incidence of VTE should even be an outcome measure in such a project. However, at the time of initiating the project, measuring against such an end point played an important part in building the case for change within TCH.
The most striking effect of this project was the increase in documented risk assessment by ward staff. Undoubtedly the development and distribution of a pocket guide (fig 1) played a major part, and the alacrity with which it was taken up by Junior Medical Officers at our earliest education sessions highlighted the need and desire for such a guide. In addition, the incorporation of risk assessment into routine daily clinical forms reinforced the importance of VTE and facilitated measurement. Nonetheless, despite such a project running over 4 years providing good-quality data, there remain significant gaps between the evidence and current practice. The Canberra Hospital is now engaged in the National VTE Prevention Programme coordinated by the National Institute of Clinical Studies (NICS) which focuses upon development of local guidelines, risk assessment against these guidelines for all patients and audit of all levels of this process.
The changes implemented as part of this project are affordable, have application in most hospital settings and have been associated with significant improvements in application of the evidence for VTE prophylaxis into clinical practice. However, further work needs to be done on our health systems if a potentially fatal and eminently preventable condition is to be significantly ameliorated.
REFERENCES
Footnotes
Competing interests MG has received a speaker’s fee from Aventis Pharma, a manufacturer of anticoagulants used in VTE prophylaxis.
Ethics approval Ethics approval was provided by ACT Human Research Ethics Committee.