Article Text

Abstract
Background Discrepant attitudes about teamwork among nurses and physicians exist in operating rooms and intensive care units. Little is known about teamwork attitudes on general medical services.
Objective To assess ratings of teamwork by providers on inpatient medical units and barriers to collaboration.
Design and participants Nurses, primary hospital physicians and medical subspeciality consultants on four general medical units were surveyed.
Measurements Providers rated the quality of communication and collaboration experienced with their own and other disciplines. Providers also rated potential barriers to collaboration. Differences between providers in ratings of collaboration and barriers were tested using analysis of variance.
Results Of 230 eligible providers, 159 (69%) completed the survey. Teamwork ratings of nurses were similarly high across provider types. Ratings of physicians differed considerably by provider type (p≤0.001). Whereas the vast majority of physicians rated the quality of collaboration with nurses as high or very high, a minority of nurses rated collaboration with physicians as high or very high. Nurses perceived the biggest barriers to interdisciplinary communication to be difficulty identifying patients' providers and their roles. Primary hospital physicians rated not having physicians and nurses on a single telecommunication system as the biggest barrier.
Conclusions In a general medical inpatient setting, discrepancies among nurses and physicians existed in ratings of collaboration and barriers to teamwork. Whereas physicians rated the quality of teamwork with nurses favourably, nurses perceived teamwork as suboptimal.
- Patient safety
- communication
- teamwork
- interdisciplinary communication
- medical errors
- physician–nurse relations
Statistics from Altmetric.com
- Patient safety
- communication
- teamwork
- interdisciplinary communication
- medical errors
- physician–nurse relations
Effective communication between nurses and physicians is essential to providing safe and effective care, as poor communication represents a major aetiology of preventable adverse events in hospitals. A Joint Commission study of 3548 sentinel events reported from 1995 to 2005 indicated communication failures were the root cause for two-thirds of them.1 Another study found that communication failures of one kind or another contributed to 91% of the medical mishaps reported by residents.2
A potential barrier to effective communication is discrepant views about teamwork among disciplines involved in patient care. A study of physicians and nurses in intensive care units found that whereas the majority of physicians gave high ratings to the quality of collaboration with nurses, the majority of nurses rated collaboration with physicians as poor.3 A similar study of surgeons, anaesthesiologists and nurses found discrepant views about teamwork in operating rooms.4 Thus, whereas physicians may perceive teamwork and collaboration as adequate, nurses consistently are not so sanguine. Despite studies demonstrating that a considerable amount of physician and nurse time in the general medical inpatient setting is dedicated to communication and coordination of care,5–7 we know little about teamwork attitudes there. Unlike an operating room, physicians and nurses on general medical units care for multiple patients simultaneously and are seldom in the same place at the same time. Paging and other telecommunication systems allow ongoing communication throughout the day but may result in an interruptive environment.8
We conducted this study to assess ratings of teamwork by providers on general medical inpatient units and perceptions of barriers to collaboration unique to this setting.
Methods
Design
We performed a cross-sectional survey of nurses, primary service physicians and medical subspeciality consultant physicians during the month of November 2007.
Setting and participants
The study was conducted at a 753-bed academic hospital in Chicago, Illinois. The institutional review board of Northwestern University approved the study. All nurses, primary service physicians and medical subspeciality consultant physicians caring for patients on four general medical units were eligible. Two primary physician services provided care for general medical patients during the study period: a teaching service and a nonteaching hospitalist service. Teaching service physician teams consisted of one attending, one resident, one or two interns, and one or two third-year medical students. Physicians on the hospitalist service cared for patients independently without the assistance of housestaff physicians or mid-level providers. Although primary service and medical subspeciality consultant physicians cared for patients on multiple units, nurses were assigned to specific units.
Unidirectional alphanumeric paging to physicians was accessible from all computers in the hospital. Nurses were also issued alphanumeric pagers, but on a separate system only accessible from one computer on the nurse's unit. All providers used a fully integrated electronic medical record (EMR) and computerised physician order entry system. A form within the EMR listed the hospital service and names of hospital physicians for each patient. Physicians were prompted to complete this form within the EMR upon patient admission.
Provider survey
Eligible participants included all nurses, teaching service physicians (housestaff and attendings), hospitalist service physicians and medical subspeciality consultant physicians (fellows and attendings) on service during November 2007. The first portion of the survey was based on previously published surveys assessing teamwork attitudes among providers.3 4 We asked providers to rate the quality of communication and collaboration they had experienced with their own and other disciplines (ie, nurses, physicians on the teaching service, physicians on the hospitalist service and physicians on medical subspeciality consulting services) using a 5-point Likert scale (1=very low, 2=low, 3=adequate, 4=high, 5=very high).
The second portion of the survey asked providers to rate perceived barriers to collaboration and communication using a 4-point Likert scale (1=not at all a barrier, 2=not much of a barrier, 3=somewhat a barrier, 4=major barrier). An initial list of potential barriers was created by the investigators and reviewed by institutional nursing and physician leadership for content validity. This review prompted the inclusion of an additional item assessing “not having a way for patients to get updated information on the names and roles of their providers” as a potential barrier. At the end of the survey, we invited respondents to provide additional comments on communication and teamwork.
We administered the survey to all eligible participants in a web-based format using an internet link (www.formsite.com from Vroman Systems, Inc.) delivered via email. Respondents entered the survey website using a unique login, which allowed for identification of non-responders. However, survey responses were deidentified. We sent non-responders a reminder email in the third and fourth week of the month.
Data analysis
Demographic data on providers were obtained from administrative databases and complemented information from surveys. We used analysis of variance to test for differences in the ratings of communication and collaboration providers gave to one another. We also used analysis of variance to test for differences in ratings of potential barriers among providers.
Results
Participant characteristics
Of 230 eligible providers, 159 (69%) completed the survey. The response rate was 71% for nurses, 91% for teaching service physicians (14 of 15 eligible housestaff and 16 of 18 attendings), 63% for hospitalist service physicians, and 55% for medical subspeciality consultant physicians. Characteristics of respondents are shown in table 1.
Provider characteristics
Teamwork ratings by provider type
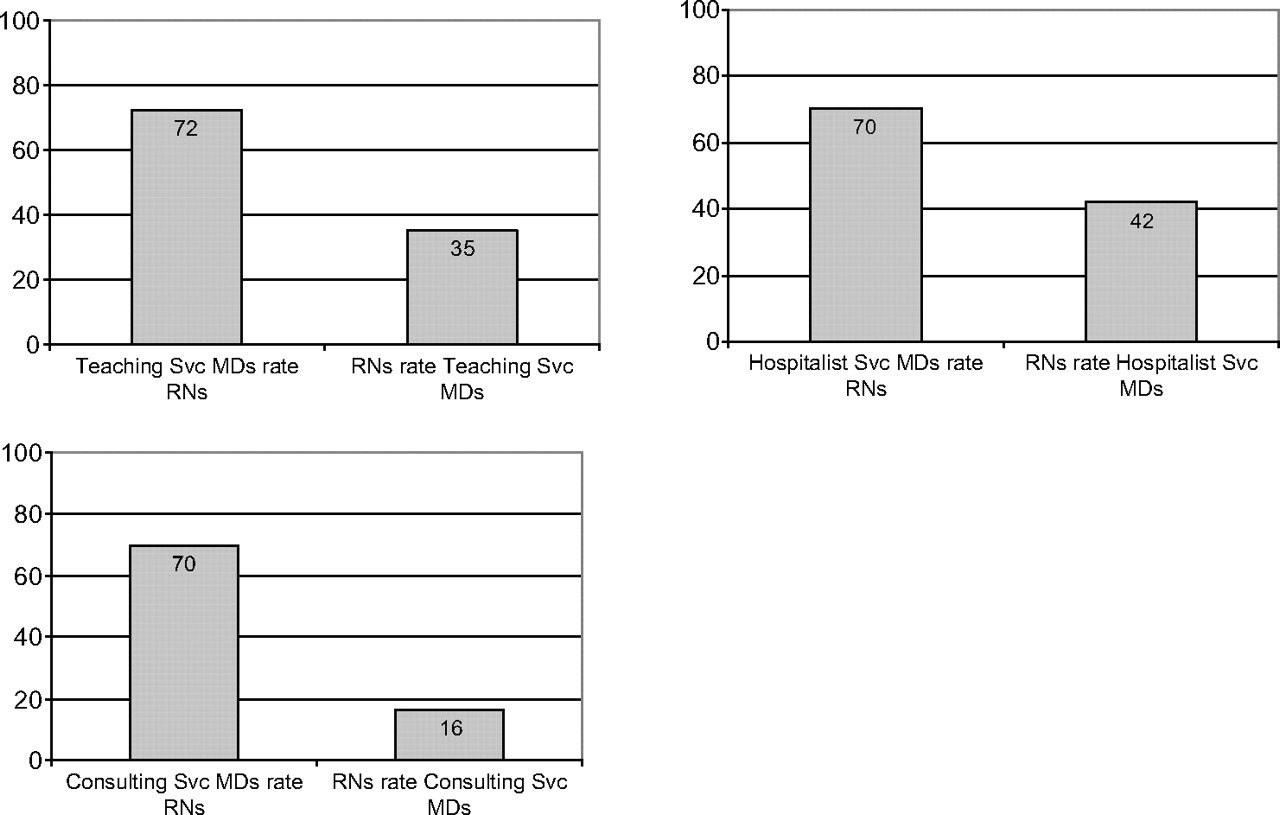
Mean ratings of the quality of communication and collaboration are shown in table 2. Physicians in each category (teaching service, hospitalist service and medical subspeciality consultants) gave nurses similarly high ratings. The ratings of physicians differed considerably by provider type (p≤0.001 for each), with nurses giving worse ratings for collaboration as compared to physicians. Medical subspeciality consultants received the lowest overall rating of collaboration (mean=3.11). As shown in figure 1, the vast majority of physicians rated the quality of collaboration with nurses as high or very high. Far fewer nurses rated collaboration with physicians as high or very high. Ratings of collaboration between consultant service physicians and primary service physicians are shown in figure 2.
ANOVA results for teamwork ratings by and of medical service provider type

Rating of teamwork between nurses and each physician type. Figures show the percentage of providers rating quality of collaboration as high or very high.

{kind=link}
{kind=link}
Rating of teamwork between consultant and primary services physicians. Figures show the percentage of providers rating quality of collaboration as high or very high.
Barrier ratings by provider type
Ratings of perceived barriers to communication and collaboration are summarised in table 3. Providers differed in their rating of certain barriers. Nurses perceived the biggest barrier to communication to be not having a way for patients to get updated information about the names and roles of their providers. Another barrier rated highly by nurses was difficulty in knowing who to call about a particular patient. Primary service physicians felt the biggest barrier was not having physicians and nurses on the same paging system. Subspeciality consultant physicians felt the biggest barrier was not knowing who to call about a patient.
ANOVA results for barrier ratings by medical service provider type
Comments
Forty-three of 159 (27%) respondents provided comments. A sample of representative comments is shown in table 4. Although a comprehensive qualitative analysis of survey comments was beyond the scope of our study, comments generally supported dissatisfaction with current communication practices, including the failure of nurses and physicians to share information on patients' daily plans of care. In addition, providers commented on barriers related to communication tools, including paging system issues and incomplete information in the EMR designating the primary service and names of physicians caring for patients.
Selected comments from provider survey
Discussion
We found that physicians and nurses have widely discrepant views on the quality of communication and collaboration on general medical services. Although physicians were generally satisfied, nurses felt collaboration with physicians was suboptimal. This finding mirrors that of previous studies in intensive care units and operating rooms. The discrepancy is worrisome because miscommunication is a major contributor to preventable adverse events in hospitals.1 2 If nurses perceive collaboration as poor, they may be reluctant to express concerns to physicians. Physicians may not appreciate that collaboration is suboptimal and therefore may not elicit additional information from nurses about their patients.
Perceptions of several barriers to communication differed depending on provider type. Nurses perceived the biggest barrier to communication to be not having a way for patients to get updated information about the names and roles of their often numerous providers (eg, residents, attending, consultants). Previous research shows that hospitalised patients frequently have trouble identifying their providers.9 10 Patients are particularly challenged in teaching settings,11 12 partly because physicians are rarely specific about their level of training and role in patient care.13 In our study, no process was in place to provide patients with reliable information on the names and roles of their physician providers.
Comments from nurses suggested that they were frustrated with explaining tests and procedures to patients and that explanations would have more appropriately come from physicians. Nurses appeared to be a liaison between patients and physicians, which was problematic because of suboptimal communication between physicians and nurses. Compounding the problem, nurses indicated that not explicitly knowing the primary hospital physician for a particular patient acted as another major barrier to collaboration. The EMR did not serve as a dependable source for the nurse to identify which service and physicians were caring for a patient.
Primary service physicians felt the biggest barrier was not having physicians and nurses on the same paging system. Although alphanumeric paging to physicians was readily accessible, alphanumeric paging access to nurses was restricted to one computer on the nurse's unit. One physician expressed frustration in having to “go to the desk, find the name of the nurse, look around for the nurse, then ask the secretary to page the nurse, and then wait around some more”. It appears nurses were able to initiate contact with physicians relatively easier than vice versa. Although it might be tempting to conclude that efforts should be taken to facilitate initiation of contact between providers, research has demonstrated that the hospital setting is already full of interruptions and distractions.6 8 Because interruptions are an important potential cause of medical error,14 15 the consequences of modifications to telecommunications systems must be carefully considered before implementation.
Medical subspeciality consultants received the lowest overall ratings for collaboration, particularly from nurses. The explanation for this is not entirely clear. Perhaps nurses were frustrated because consulting service physicians communicated recommendations to primary service physicians, who in turn did a poor job of communicating those recommendations to nurses. Consultants, like nurses, rated not knowing who to call about a particular patient as a barrier to communication, providing additional support that this information was not adequately updated in the EMR. Nonetheless, consultants rated overall teamwork and collaboration highly despite the reciprocal assessment from their colleagues.
Our study provides strong evidence that collaboration and teamwork between providers on general medical units is suboptimal and serves as a call to investigate potential interventions. Teamwork training has been used in emergency medicine and labour and delivery units with variable success.16 17 Intensive care units have successfully used daily goals of care worksheets during bedside rounds to clarify and communicate care plans.18 19 In light of the fact that hospital-based physicians and the nurses with whom they work are seldom in the same place at the same time, teamwork training and bedside rounds with nurses may not be feasible. Studies have evaluated the use of regularly scheduled interdisciplinary rounds (IDRs) as a method to assemble patient care teams and collaborate on the plan of care for general medical patients. Curley et al20 demonstrated a reduction in cost and length of stay with the use of IDR on a general medical teaching service. O'Mahony et al21 demonstrated improved housestaff perceptions of relationships with nurses and reduced lengths of stay using IDR. Nurses' perceptions of collaboration were not assessed.
Our study has several limitations. We conducted surveys of nurses, primary service physicians, and medical subspeciality physicians at a single site. It is possible that ratings of collaboration between physicians and nurses on general medical units differ in other hospitals. Because studies of providers in other settings have shown similar findings,3 4 we feel that discrepancies in collaboration between nurses and physicians on general medical units are likely to be present in most hospitals. In addition, we did not assess ratings of collaboration by additional members of the general medical healthcare team, including social workers and therapists, because we were unable to obtain an adequate sample size for meaningful comparison. Larger studies, including ratings of collaboration by social workers, therapists and other consulting services, are warranted.
In summary, discrepancies exist in the ratings of collaboration between physicians and nurses on general medical units. While studies have found similar discrepancies in other settings, unique barriers to collaboration exist on general medical units that appear to affect providers' communication patterns. Future research should assess methods to remove barriers to collaboration and interventions designed to bring providers together to develop a shared plan of care.
Footnotes
Funding Funding support received from the Northwestern University Department of Medicine.
Competing interests None.
Ethics approval This study was conducted with the approval of the Northwestern University.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.