Article Text

Abstract
Objectives (1) To improve quality and equity by increasing utilisation of mammography screening among Israeli Arab women. (2) To explore effectiveness of designing interventions with a combined top-down and bottom-up approach.
Design Retrospective study at two periods of time: 2004—intervention's preliminary stages; 2005—intervention's implementation.
Setting Maccabi Healthcare Services (MHS), an Israeli health plan serving 1.7 million members at study period; 7% of them are Arabs by 139 branches, 13 of which serve Arabs exclusively.
Macro-organisational intervention (top down) Development of a computerised Mammography Promotion System, phone contacts with non-respondents and intraorganisational reporting of screening rates.
Intensive intervention (bottom up) A local analysis of barriers to care and implementation of tailored solutions. This intervention was initiated and documented in three Arab branches, with spillover to the entire Arab sector.
Measure definition Biennial breast cancer (BC) screening of eligible women.
Improvement measures Changes in BC screening rates in Arabs and comparisons with overall MHS BC screening rates for 2004 and 2005.
Results In 2005, average BC screening rates in Arab branches increased from 26.7% to 46.2% (73% improvement), while overall MHS screening rates increased from 49.0% to 63.1% (29% improvement). Analysis of the relative differences between 2004 and 2005 BC screening rates indicated statistically significant differences (p<0.006) in rates between the Arab and other branches. These results did not change after adjustment for branch size, region and branch average age.
Conclusions Combined top-down interventions and bottom-up initiatives are effective for formulating programmes to reduce inequality.
- Quality improvement
- breast cancer screening
- healthcare disparities
- equity
- Arab women
- Israel
- chronic disease
- quality of care
- Arab women
Statistics from Altmetric.com
- Quality improvement
- breast cancer screening
- healthcare disparities
- equity
- Arab women
- Israel
- chronic disease
- quality of care
- Arab women
Setting
Breast cancer (BC) is the leading cause of cancer-related deaths among Arab and Jewish women in Israel.1 Israel's Arab population, currently numbering 1.3 million (20% of total population), resides primarily in rural villages and small towns. The Arab population is characterised by large disparities in education, income, employment as well as health status when compared with the Jewish population.1–4 These social factors, in addition to other cultural and behavioural factors, are well documented as influencing health and healthcare utilisation among Israeli minorities, including Arabs.5–7 Maccabi Health Care Services (MHS), under the National Health Insurance Law (NHIL) and Israel's universal healthcare system, insures 7% of the Arab population; the rest are insured by Israel's three other health plans.
MHS was providing services for 1.7 million members in the period covered by the study. Services were and continue to be delivered by self-employed physicians and other health professionals affiliated with the plan's 139 local branches, distributed among six regions; 13 of these branches are located in Arab towns and villages, and thus serve primarily Arab population. In 2004, MHS instituted a system of performance measurement throughout the organisation to promote quality improvement; results have been published internally and externally to promote transparency.8
In 2003–2004, the national biennial breast cancer screening rate (BC screening rate) among Arab women aged 50–74 was 32%, compared with 54% among Jewish women in the same age group.9 These trends were similar to those observed in the US (age 40+) and the UK (age 50–74), where women belonging to ethnic minorities or to low- to medium-income groups exhibit lower BC screening rates and thus more advanced disease at diagnosis.10 ,11
Increased BC screening has been a national objective in Israel since 1997, with personal invitations to undergo mammography screening sent biennially to all women aged 50–74; this service is supplied free of charge.12 Yet, by 2004, the BC screening rate among the national target population stood at 52.0%, with significant gaps between the rates of women from low socio-economic backgrounds and other women (45.8% and 54.8%, respectively).13 Among female members of MHS, the global screening rate was 49.0%. This figure was slightly lower than the national average yet much below the 73.4% reported by US commercial health plans for women aged 52–69 in the same year.13 ,14 The BC screening rate for MHS branches serving the Arab population was particularly low when compared with the health plan's regional and total screening rates for 2004. This screening rate became our call for action.
In tandem with macro-level (top-down) organisational efforts, local branch staff initiated focused (bottom-up) attempts to improve screening rates, based on their field experience. The intervention recounted here pertains to these intensive efforts, which began in three branches in 2004 and continued throughout 2005. The efforts and results were well documented, with spillover to other Arab branches accompanied by little or no documentation.
Objectives
To improve quality of care and equity by increasing utilisation of mammography screening among Israeli Arab women aged 52–74, a group insured by MHS and considered to be low users of BC screening.
To explore the effectiveness of designing top-down and bottom-up interventions, which combine macro-organisational with more focused local programmes.
Design
Key improvement measures
Measures were devised to reflect the two quality-improvement goals: changes in absolute biennial BC screening rates in the Arab population and changes in those rates, between the two periods of time, in comparison with changes in overall BC screening rates in MHS:
Absolute rates of BC screening (defined as the proportion of women aged 52–74 who had had at least one mammogram in the last 2 years) were measured per branch in two time periods: September 2004 (R2004) and December 2005 (R2005) (figure 1). The measure of change was defined as the relative difference (RD) in BC screening rates, calculated as
To facilitate direct comparison of the 13 Arab branches with overall MHS rates, we calculated a standardised rate ratio (SRR) for each target branch, defined as Oi/E*i, where Oi is the rate of women in branch i=1, …, 13, who had performed BC screening, and Ei* is the expected rate for that branch based on the age-specific screening rates among the organisation's entire female population. An age-adjustment factor was introduced into the formula because this type of screening rate changes with a woman's age.
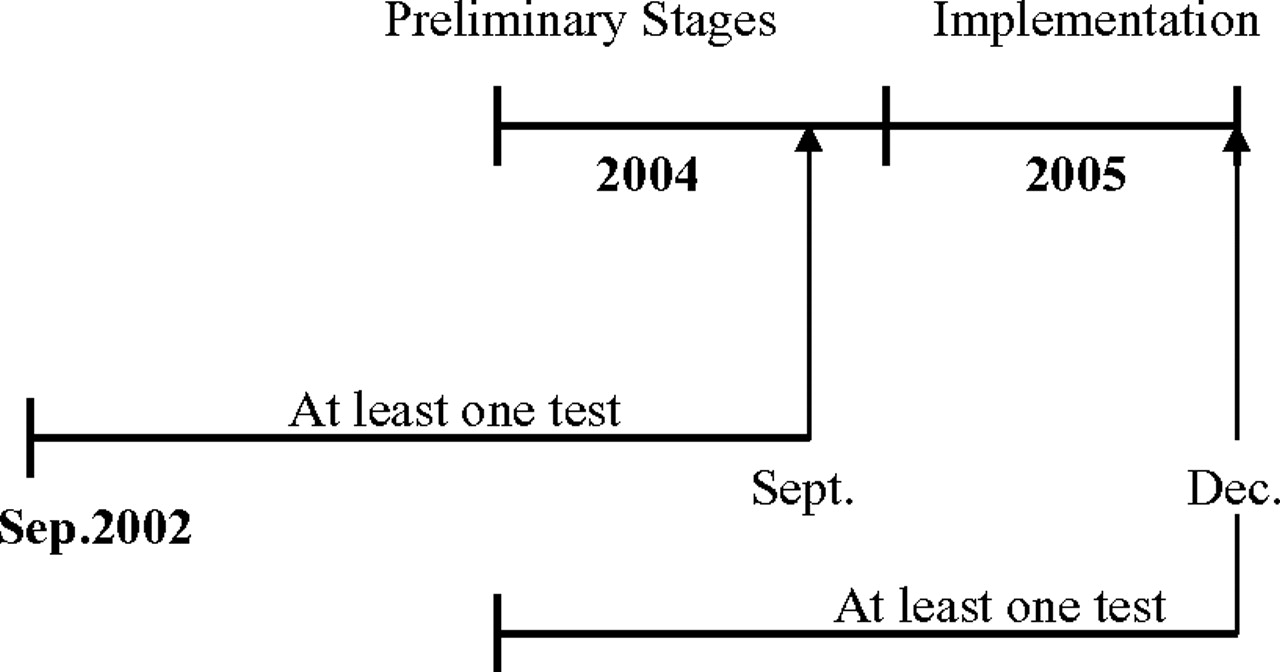
Study time periods.
We considered 2004 as the period of the intervention's preliminary stages (planning and fieldwork) and 2005 as the period of the intervention's implementation.
Data collection
To gather the data, we used the ‘Mammography Indicator,’ implemented in the organisation's ‘Performance Measurement System,’ which derives its data from the operational database housed in the organisation's main computer. The ‘Mammography Indicator,’ was defined as: ‘Woman aged 52–74 who received at least one BC screening during the last 2 years.’ BC screening rates were assessed at two points in time—September 2004 and December 2005.
Selection criteria
Ethnicity
At the time of the intervention, the organisation's operational database did not permit precise identification of populations by ethnic affiliation, religion or socio-economic status. Because the 13 branches serve the Arab population exclusively, branch location was chosen as a proxy for ethnic identity. In September 2004, a total of 1429 Arab women were members of the 13 respective branches. Relevant data on all these women were collected and analysed by branch. For purposes of comparison, data on all MHS's 125 063 women aged 52–74 were also analysed by age and branch.
The data were extracted from the operational database using the organisation's main computer (IBM-AS400). In three out of the 13 Arab branches—Al-Tira, Tayibe and Kalanswa located in central Israel, together known as the ‘Triangle’—a local effort was initiated to intensify the macro-organisational intervention. These special activities are describes bellow.
Data analysis
Relative differences in BC screening rates were calculated for each branch (RDi, i=1,…,139) using a regression model for log-transformed measurements. Non-parametric methods were also used. The results are presented for the three intensive intervention branches (nos 9, 11, 12), for the other 10 Arab branches (nos 1, 2, 3, 4, 5, 6, 7, 8, 10, 13) and for all other 126 MHS branches to allow for comparison between the two intervention populations: MHS Arab members and the entire MHS insured population. The SRRs were calculated separately for each year, as overall mammography screening rates changed dramatically between 2004 and 2005. Confidence Intervals (CIs) were calculated based on Poisson assumptions regarding the rates and Bayer approximation.15 SRRs closer to 1 indicate that branch rates did not differ significantly from expected rates based on the health plan's total female population adjusted by age. Similarly, SRRs far from 1 indicate greater differences between the observed and expected screening rates. Since we know retrospectively that there was a spillover of ideas from the ‘Triangle’ to other Arab branches and that spillover was not documented but reported later upon request, we decided to analyse the 13 branches as one group. All analyses were performed with STATA software (STATA, College Station, Texas).
Intervention
Macro-organisational intervention (top down)
As part of macro-level organisational quality-improvement initiatives, a steering committee composed of representatives from the six MHS regions, covering all 139 branches, was mandated to formulate a strategy to improve the BC screening rate. Efforts were guided by a facilitator who had been trained to apply quality improvement methods and tools. Previous efforts to improve screening were reviewed to identify the most effective features for integration into the current intervention. On the macro-organisational level, the following actions were instituted:
A Mammography Promotion System was developed using the MHS main computerised system. This system scanned the population monthly to construct a list of members requiring mammography screening and produced invitations, in the form of postcards, to do so.
Non-respondents to invitations were identified at the branch level and contacted by phone. The steering committee created various ‘scripts’ to facilitate dialogue.
Computerised decision-support tools were developed to notify the primary physician, when entering an eligible patient's electronic file during a medical encounter, as to whether she had undergone screening.
To encourage peer comparison, physicians also received information comparing their patients' screening rate with regional and organisational rates.
Intensive local intervention (bottom-up)
In early 2004, A Gabali, a nurse and manager of Maccabi's ‘Triangle’ branches, constructed a team composed of herself, a physician and the manager of the Kalanswa branch with the aim of identifying the barriers to local implementation of the national programme. The barriers identified were:
Accessibility—The nearest screening facility was located 30 km outside the ‘Triangle,’ with access constrained due to transportation difficulties.
Social norms—Numerous families disapprove of women leaving the city unaccompanied by a male relative, acting as chaperone. During the screening facility's working hours, few male family members were available to do so.
Moral values—Due to their religious upbringing, women were often embarrassed by the prospect of a male physician conducting a breast examination. Many women were also fearful of social stigmatisation if it became known that they had undergone screening.
Lack of Self-Care Values—BC, like other diseases, has traditionally been perceived as a ‘natural’ life event. Hence, the majority of Arab women in the target age group have not internalised pro-active self-care values.
Inadequate Information—Arab women, like other ethnic minorities, lacked sufficient information about the disease, the examination, the benefits of early detection and their membership in the national programme's target population. One source of this gap: information is rarely distributed in their mother tongue, Arabic.
Postcard failure—An unknown proportion of screening invitations did not reach their targets: Because more than one person in Arab extended families bear the same first and last names, delivery errors often occurred.
The ‘Triangle’ team chose to implement the following solutions:
Personal contacts were initiated with community leaders to mobilise their support for the programme.
The team leader (A Gabali) personally went from door to door to convince women to participate in the programme.
A compact ‘treatment package’ was constructed for transmission during patient meetings with staff. It included A Gabali's explanation of the examination and its importance, an examination by a physician—always in the presence of a female nurse—and the making of an appointment at the screening facility.
To remove barriers to care, flexibility was introduced into the clinical protocol as dictated by patient needs. For example, the male physician's examination could be waived if it caused distress.
Local branch staff organised group transportation to the screening facility for branch members.
Their efforts reached 80% of the women eligible for BC Screening. The activities of the ‘Triangle’ branches were facilitated by members of the MHS BC Screening Steering Committee who were involved in other Arab branch activities and acted as the platform for the spillover of ‘Triangle’ ideas to other Arab branches. In addition, these actions were supported by the organisation's infrastructure—for example, computerised decision-support tools and centralised production as well as delivery of screening invitations.
Results
In 2004, MHS membership included 125 063 women aged 52–74, with an overall BC screening rate of 48.98%. The Arab members of the 13 branches included 1429 women in this age group, only 26.73% of whom had undergone screening in the previous 2 years. The median age of the total population was 59 (mean 60.42), and the IQR was 55–66; the overall SRR for the Arab population in 2004 was 54.59%.
By 2005, the overall female health plan membership in the 52–74 age group had increased slightly, to 133 372; of these, 63.07% had undergone screening in the previous 2 years. Among the 1516 Arab women in the respective age group, 46.17% had undergone screening. The overall SRR for the Arab population in 2005 was 73.22%.
The age distribution of female MHS members, including Arabs, remained virtually the same in 2005 as in 2004.
Statistical analyses indicated a significant improvement in BC screening rates in the 13 Arab branches.
Table 1 shows age-specific screening rates for 2004 and 2005 as well as the differences in those rates.
Breast cancer (BC) screening rate (%) by selected age, total female membership, Maccabi Health Care Services, 2004–2005
Figure 2 shows the relative difference (RD) between 2004 and 2005 BC screening rates per branch. The figure shows very low rates for many of the Arab branches in September 2004, with a very large change apparent by December 2005. Regression analysis (not shown) on the log-transformed RD indicated a statistically significant difference (p<0.006) between Arab and other branches. These results did not change after adjustment for branch size, region and average age of the women in each branch.
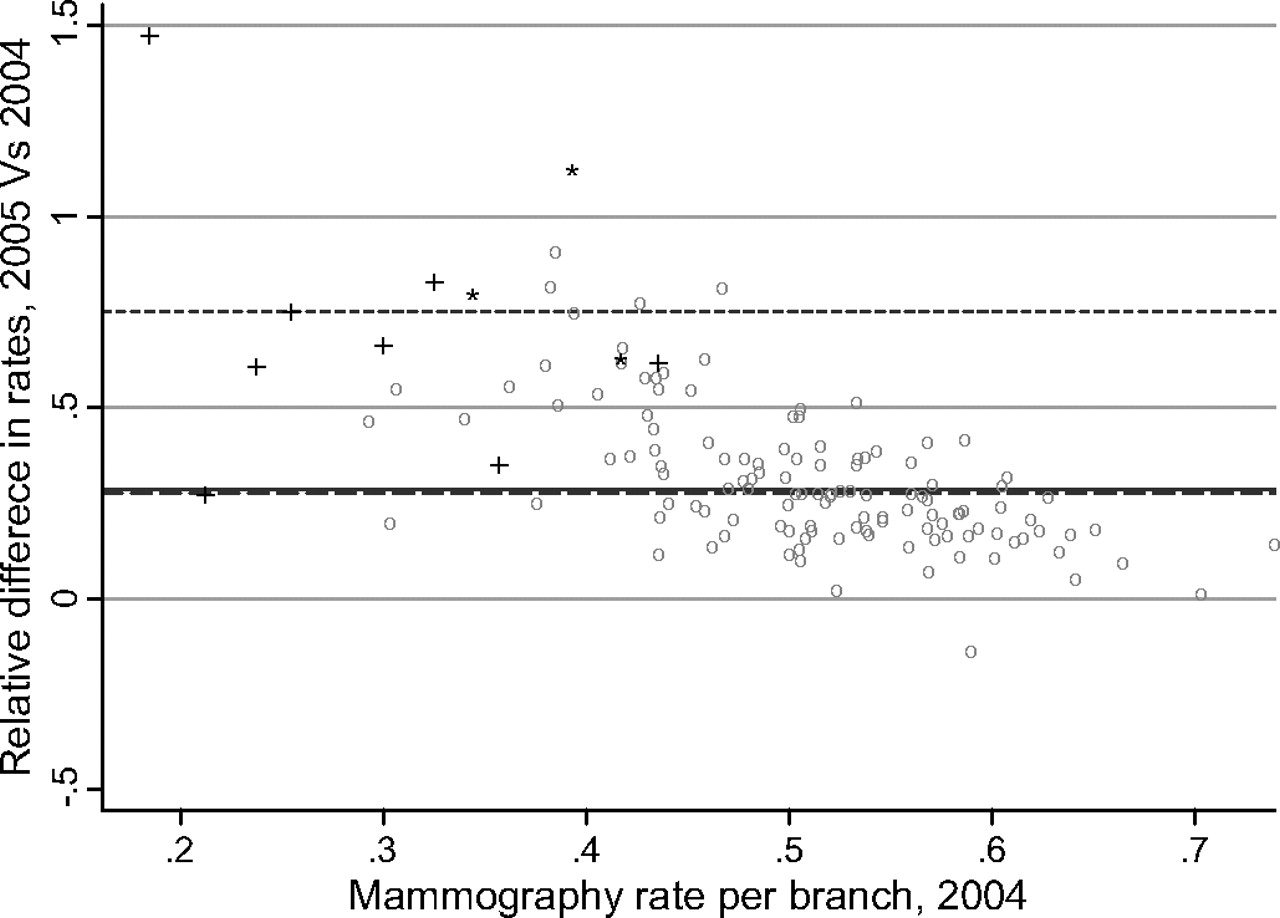
Comparison of relative change in breast cancer screening rate (mammography rate), 2004–2005, by Maccabi Healthcare Services branch without the two branches with relative difference≥2.
Figure 3 shows the SRRs at the 95% CI for the 13 Arab branches in 2004 and 2005. In 2004, most branches exhibited preintervention SRRs well below expected rates, whereas in 2005, some branches displayed SRRs not significantly different from total MHS rates (at an SRR of 1). Branches 9, 11 and 12, the ‘Triangle’ branches participating in the intensive intervention, demonstrated a significant change. Branches 4 and 8, located in the Bedouin rural settlements of Rahat and Kseife, also presented a significant change, presumably due to the spillover effect.

{kind=link}
{kind=link}
{kind=link}
Comparison of breast cancer screening rate among Arab women, members of the 13 target branches and all female members of Maccabi Healthcare Services 2004 (in grey) and 2005 (in black), using standardised rate ratios (SRRs) and 95% CI.
Discussion
Initial performance data revealed a significant disparity in quality of care, expressed as differences in BC screening rates. The local team chose to preferentially allocate organisational resources to reduce disparities based on two factors: (1) the organisational effort to promote utilisation of BC screening among all population groups given MHS overall rates, which were lower than national and international benchmarks; and (2) the team's in-depth familiarity with the special needs and barriers to care characterising the local population, coupled with a readiness to invest additional resources. These two factors formed the foundations of the top-down combined with the bottom-up approaches. The organisation's extensive activities in this field culminated in the creation of a dialogue, a learning process and a solid infrastructure on which local (bottom-up) initiatives could develop.
The uniqueness of this three branches' intervention effort rests primarily in the fact that the barriers were explored by local people, all of whom are Israeli Arab health professionals, well respected and trusted by their staff, the local population and community leaders. Added was the encouragement and facilitation provided by the organisation. The spillover to other Arab branches was enabled by concurrent horizontal activities initiated by the BC Screening Steering Committee, which nurtured a dialogue between and within the organisation's Arab branches.
The process implemented in the ‘Triangle’ became a ‘big story’ in the organisational discourse and produced several important organisation-wide benefits. Disparities in healthcare were no longer viewed as trivial and now acknowledged as calls for strategic action; an ‘equity discourse,’ instituted throughout the organisation, has led to further actions. Among the latter was the introduction of a combined approach to reduce disparities within other clinical domains, an approach that rested on field confirmation of the salience of bottom-up input for the tailoring of quality improvement efforts to priority populations. In addition, dissemination of the transparent performance measure heightened management recognition of and commitment to the screening programme's equitable implementation.
This case has confirmed once more that careful analysis of the place-specific context is essential for understanding differences across communities stemming from various causal factors.16 It demonstrates that specific contextual characteristics—education, family income and continuous health insurance—are independently associated with BC screening. Ethnicity, as reflected in socio-economic status, access to healthcare and life style disparities, was likewise found to be associated with BC screening utilisation and stage of BC at diagnosis.17 These variables can therefore be used to identify populations in which women are at increased risk for delayed BC diagnosis. They can also inform the planning phase of initiatives meant to enhance BC screening and reduce disparities in treatment outcomes.18 We would therefore recommend that organisational efforts to increase equity and reduce disparities in healthcare utilisation and health outcomes consider these variables when planning interventions, especially those targeted at populations at risk.
The local intervention was developed during the experimental learning phase without any notice given to similar activities elsewhere. This may explain what happened in branches 4 and 8, two geographically distant Bedouin settlements. News of the ‘Triangle's’ experience had been disseminated to other Arab branches where it promoted undocumented local activities, what can be considered a spillover effect. Retrospectively, we learnt that staff in the latter two branches also negotiated with local community leaders, used a mobile screening facility to enhance accessibility and spread invitations door to door.
The ‘Triangle’ case also invites evaluation of the two major attitudes to performance recognition and reward: (1) an emphasis on absolute performance, which is advantageous to stronger units, and (2) recognition of relative improvements in performance, which provides incentives to weaker units beginning at lower levels of performance and therefore more prone to achieving greater relative change. Because equity is an important dimension of quality, we concluded that there was great value in recognising the Arab branches that had begun with lower screening rates and made greater relative progress in consequence.
Limitations of the research
The study's limitations relate primarily to the employment of proxies—the local plan branch—for identification of the research population. Because the study focused on women from the local branches serving almost exclusively Arab populations, Arab women in ethnically mixed cities such as Nazareth, Acre, Jaffa and Haifa were unrepresented. We assume that in mixed cities, screening rates are higher, and barriers to care somewhat differ. This does not, however, undermine the validity of the results or the approach taken in the selected homogeneous branches.
Lessons learnt and interpretation
Based on the experience reported, invitations for mammography as well as other screening were recently translated into Arabic and Russian, the two major languages spoken in Israel other than Hebrew. We expect this effort to facilitate contact with plan members and improve transmission of educational materials.
It has also been decided to investigate expansion of the organisation's operational database. We are interested in adding parameters such as ethnic affiliation and socio-economic status, to be correlated with performance indicators so as to broaden opportunities to identify target populations and decrease disparities.
Despite the significant improvement observed, BC screening rates among the Israeli Arab population remained far from optimal by the end of 2005. However, in subsequent years, disparities became a managerial concern, with equity issues accepted as an integral part of the organisational discourse. In 2008, MHS adopted equity in service provision and health outcomes as a major strategic goal. Analysis of performance measures according to socio-demographic profile supported identification of member populations at risk, which led to construction of the first MHS Organisational Equality Report.19 A wide range of disparities in clinical and prevention domains, characterising the Arab minority as well as other population segments with a low socio-economic status, were consequently revealed. The age-adjusted BC screening rate among the Arab population in 2008 was 0.88 of the rate among the Jewish population. As a result, it was decided to allocate preferential resources to populations at risk, and decisions relevant to care provision were taken. These included training of health professionals and administrative staff in the cultural adaptation of health services, an increase in the linguistic accessibility of educational materials and so forth.
As this initiative has shown, quality-improvement measures can reflect as well as respond to equity considerations. Whitehead has proposed an ‘action spectrum on inequalities in health,’ beginning with measurement, continuing through recognition, awareness-increasing, willingness to take action, local initiatives, more-structured development and comprehensive coordinated policy.20 This approach is being more stringently adopted throughout the organisation.
The reported intervention increased organisational receptiveness to the synergy emerging from adjustment of top-down policy to bottom-up implementation requirements, based on recognition of the legitimacy—and necessity—of each approach for quality healthcare delivery. This outcome is being incorporated into the plan's organisational culture as a cornerstone of equity-oriented strategic planning and implementation. We anticipate that these measures will alter the prognosis that ‘geography is destiny.’
What did not work?
We now know that a few elements in the top-down intervention did not work. For instance, the feedback that physicians regularly received regarding BC screening performance was ineffective, mainly because a structured, non-judgemental dialogue between managers and physicians following these reports did not take place throughout the organisation.
Finally, we assume that our experience and study results can be beneficial for other Israeli and non-Israeli health services interested in closing health disparities in BC screening utilisation as in other clinical domains where low use among ethnic and cultural minorities is a reality. As this case has taught, we assume that each organisation should tailor interventions to its own population.
What is already known on this issue
Ethnic minorities and low socio-economic status groups underutilise health services and display poor health outcomes.
Careful analysis of the place-specific context is essential for understanding differences across communities stemming from various causal factors.
Avoidance of a ‘one size fits all’ policy can improve equity by setting the stage for heterogeneity in intervention planning and implementation, necessary for programme adjustment to community characteristics and health needs.
What this study adds
Field staff can contribute significantly to reducing healthcare disparities due to their familiarity with local barriers to quality care and input when constructing tailor-made solutions.
The power of local stories lies in its potential to increase organisational awareness of healthcare disparities and stimulate corrective action.
Intuitive responses to messages from the field and ‘outside the box’ thinking can lead to innovative solutions. This approach should be considered an addition to the quality ‘toolbox.’
Acknowledgments
We would like to thank J Hatib, branch medical director, and A Marae, branch manager, Kalanswa, for their determination and dedication in supporting the project and in bringing this story to the organisation's attention.
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.