Article Text

Abstract
Objective—To evaluate the use of a multidisciplinary record held by patients with cancer in the community.
Design—Pragmatic randomised controlled trial.
Setting—The environs of Swansea in south west Wales.
Participants—501 patients under the care of the Department of Oncology, Singleton Hospital, Swansea.
Intervention—A patient held record used by the patient and healthcare professionals.
Main outcome measures—Health related quality of life (EORTC QLQ-C30) measured at entry into the study and at 6 months; patients' views at 6 months; healthcare professionals' views collected after the completion of patient follow up; NHS resource and booklet use.
Results—1148 patients were eligible for the study; 501 were recruited (44%) and 344 completed the study (172 in each group). There was no significant difference between the two groups in change in quality of life or NHS resource use. The patient held record did not have an impact on communication but was significantly helpful to patients in preparing for appointments, reducing difficulties in monitoring their own progress, and helping them to feel more in control (p<0.05). Fifty three percent of patients would have preferred not to have a patient held record. There was a low level of use of the record by healthcare professionals but most of those who remembered using it indicated that they would prefer patients to have it.
Conclusions—The patient held record is valued by some patients and professionals but has no significant impact on the quality of life of patients or NHS resource use. It has a positive impact on quality by helping patients feel more in control and prepare for meetings with healthcare staff. Patients who find it useful tend to be younger and have more professionals involved in their care. It is recommended that it should be made available to patients on request and used by them according to need.
- cancer
- patient held records
- patients' views
- professional views
Statistics from Altmetric.com
Shared care record cards commonly carried by the patient—where the exchange of information is made through a booklet or “cooperation card”—have been found to be a popular way of integrating primary and secondary services, particularly in paediatrics and in maternity care.1 The positive benefits to the quality of care of patients with cancer include giving patients control over information, ensuring that medication and other records are contemporaneous, and obviating the need for the medical record to be immediately available in an emergency.2–5 However, some patients feel stigmatised and do not want this constant reminder of their condition, while others use it as a therapeutic diary, disclosing their reflections on disease progression and on encounters with healthcare personnel. Others use it primarily as an aide-mémoire to taking medication.67 In a randomised controlled trial in Oxford8 the value to patients with cancer was shown to be similar to conventional record keeping, but the views of health professionals other than general practitioners were not documented. This is important as previous studies have shown that healthcare professionals can influence patients' use of their own records.6 When the professional appears to be busy or distracted in using the document, patients cease offering it in a consultation.7
The aim of this study was to evaluate whether a patient held record improved the overall quality of care of a patient with cancer. This was addressed under five objectives which evaluated:
change in patients' quality of life;
patients' views on issues relating to coping with their illness and their preference with regard to record keeping;
the extent to which the patient held record is used by patients and healthcare professionals;
healthcare professionals' views and preference;
any effect of the patient held record on NHS resource use.
Method
The study was a single centre pragmatic randomised trial performed in the Department of Oncology at Singleton Hospital, Swansea which serves a population of approximately 800 000 in south west and west Wales. Patients seen at this cancer centre are referred from hospitals in Neath, Swansea, Llanelli, Carmarthen, Haverfordwest, and Aberystwyth which serve urban and rural populations including some of the most deprived areas in Europe. The day to day management of the patients involves a broad range of hospital and community based healthcare professionals.
STUDY SUBJECTS
Patients aged 18 or above were recruited through their treating oncologist over a 16-month period from January 1998 to April 1999. Patients were excluded from the study if their malignancy was a basal cell carcinoma of the skin, if they were not able to be responsible for the patient held record, did not have a carer who was able to take this responsibility, or were registered at one of the six general practices involved in a pilot project.
Patients potentially suitable for inclusion in the study were identified from sequential oncology clinic lists and notified by post before they attended. In the clinic the study was explained in detail before consent was obtained. Recruitment included new patients and those already under care. Randomisation after consent and study registration was by an independent computer randomised schedule. Those randomised to the intervention were given the booklet with a full explanation of its use, supported by the following instructions which were printed inside the front cover: “Please use this booklet to note: questions you want to ask; all your current medication; problems with changes of medication; anything else you feel is important as a memory aid. Please take this booklet with you when you go to any hospital or to your doctor's surgery and ask whoever you see to write in it. If a doctor or nurse visits your home please also use this booklet”.
The booklet is A6 size with four different coloured sections for (i) free text entries by the patient, (ii) free text entries by health professionals, (iii) details of medication, and (iv) dates of appointments. This simple four sectioned format was considered easier to use than a blank booklet2 but retained the convenience of being pocket sized. It emerged from a previous study in which a multi-compartment booklet was compared with a more simplified design.7
The study was approved by the West Glamorgan and Dyfed Powys local research ethics committees and all patients gave written consent following oral and written explanation.
PATIENT QUALITY OF LIFE
Quality of life was measured using the EORTC QLQ-C30 questionnaire9 which was completed in the clinic at recruitment and by telephone or post at 6 months. This is a 30-item questionnaire which incorporates nine multi-item scales covering subjective functioning (physical, role, cognitive, emotional and social), symptoms (fatigue, pain and nausea/vomiting), and global health and quality of life. It also includes single item measures covering dyspnoea, sleep disturbance, appetite loss, constipation, diarrhoea, and financial impact.
PATIENTS' VIEWS AND PREFERENCES
Patients were interviewed 6 months after recruitment to ascertain their views and preferences regarding the patient held record using a semi-structured questionnaire. They were asked to indicate the degree of difficulty they encountered in the understanding of what was happening to them; remembering what healthcare staff said; preparing for sessions with healthcare staff; asking about worries; monitoring their progress; keeping information private; and keeping in control. The questionnaire offered four options for answers: no difficulty at all; a little difficulty; quite difficult; very difficult. The opportunity was also given for free comment. Patients were also asked their perception of communication between professionals; their preference regarding health record keeping; and the reason for this preference. Those allocated a patient held record were asked their views about the design and use of the booklet including the usefulness of being able to refer to it; the value of being able to write their thoughts down; the ease or difficulty of remembering to take it to appointments; and the ease or difficulty of asking healthcare staff to write in it.
BOOKLET USE
The frequency with which the booklet was used by patients and healthcare professionals and the mode of use was studied by examination of booklets recalled at the end of the 6 month period of use. Patients were asked to send in their booklets, which were photocopied and returned immediately. Data were collected on the number of entries in each section, by whom these entries were made, the number of times direct communication between healthcare professionals and patients was noted, changes in medication, deterioration in health, and the number and type of appointments recorded. It was noted whether the patient had used the booklet as a diary or an aide-mémoire and whether professionals had used it to communicate with other professionals, to give written explanation to patients, or as a clinical record. The data collection process was piloted on five randomly selected booklets to identify any problems and/or improvements. The data were extracted by two researchers working independently. After 20 booklets had been scrutinised, findings were compared and inconsistencies or problems resolved. Inter-rater reliability was assessed by a third researcher.
HEALTHCARE PROFESSIONALS' VIEWS AND PREFERENCE
Healthcare professionals' satisfaction with and preference for the patient held record was assessed after completion of patient follow up. Professionals were identified from entries in the booklets and sent a semi-structured questionnaire by post. Non-responders were sent one reminder. The questionnaire, which was piloted before use, asked for views on the impact of the patient held record on paperwork, patient anxiety, litigation, interprofessional communication, and patient communication, as well as covering the issues included in the semi-structured interview with patients. Healthcare professionals were also asked whether they felt use of the booklet altered consultation time and by how much.
NHS RESOURCE USE
The interviews with patients at 6 months were also used to collect data on contacts with health professionals, including at hospital during the 4 weeks preceding the telephone interview.
SAMPLE SIZE
A sample of 500 patients was planned to allow for an attrition rate of 48%, giving an 80% chance of detecting a 10 point difference in the EORTC subscales and a difference of approximately 20% in the proportion of patients preferring a patient held record compared with the control group. We did not consider a difference of less than 20% between the two groups to be clinically significant.
DATA ANALYSIS
Quality of life data were stored using a generic clinical information system (GeneCIS)10 and exported for analysis on SPSS (Release 8.0.1, Chicago, 1998) by “intention to treat”.11 To counteract the effect of possible differences in baseline health related quality of life scores, changes in individual scores from baseline were analysed using t tests. Interview replies were also stored on GeneCIS in coded form and as free text comments. Answers relating to “degree of difficulty” were coded from 1 to 4 and analysed by χ2 test. Preference data were analysed by χ2 and Mann-Whitney U tests. For those allocated a booklet, the strength of association between their views on its use and their preference was analysed by Goodman and Kruskal tau (τ).12
Patient recall has been shown to be a reliable source of resource data.13 However, as a check against possible recall bias, a validity exercise was performed on a sample of 58 patients to compare patient recall with data abstracted from GP records for the same time period. Additionally, an inter-rater reliability exercise was performed to assess agreement on interpretation of resource use data recorded in the telephone interviews. Kappa statistics and paired t tests were used to establish agreement between data collected from the two sources (validity) and two independent assessors (inter-rater reliability). As descriptive statistics suggested the presence of skewness in the resource data, 1000 bootstrap replications14 of the original data were performed and mean differences assessed by t test.
Results
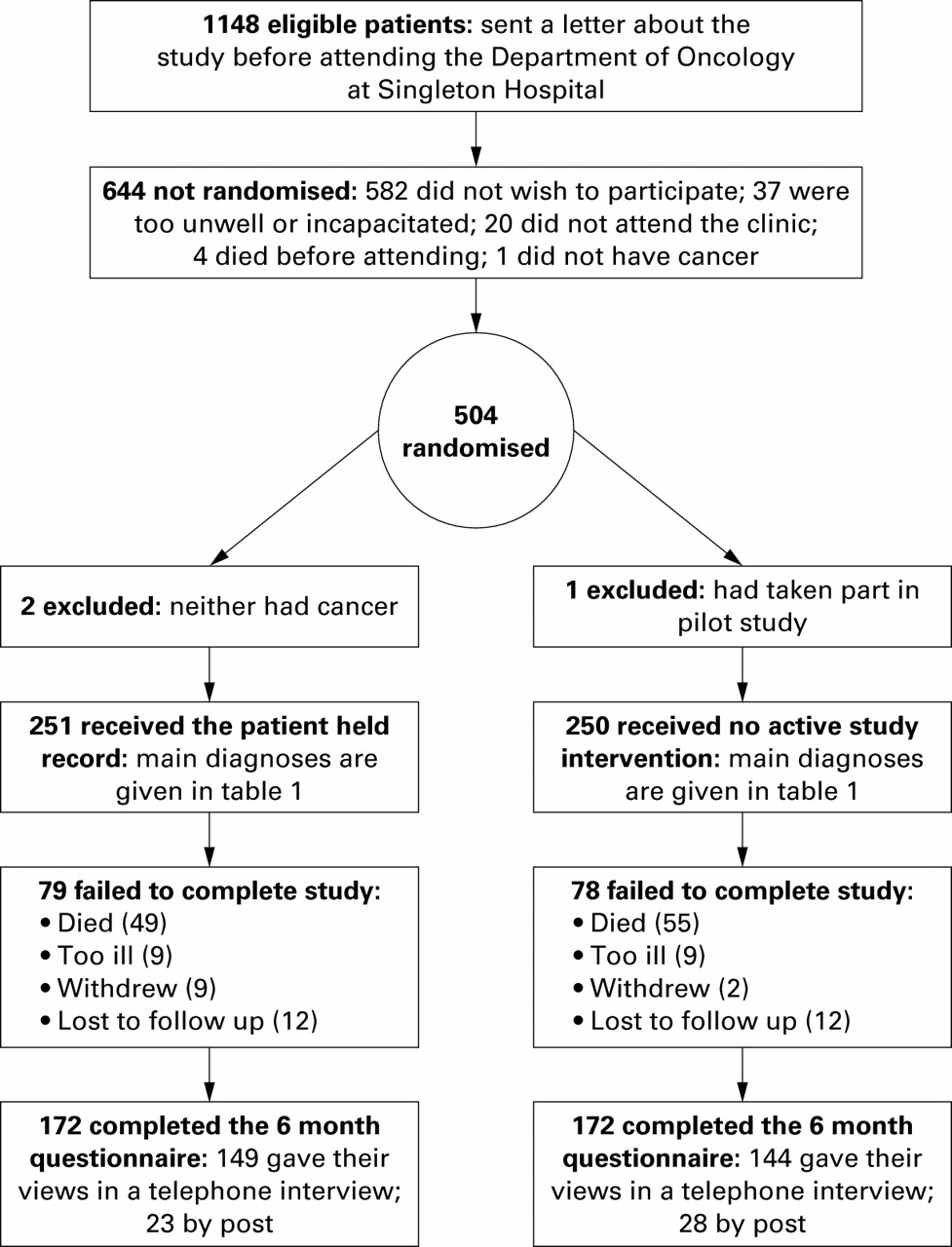
The numbers participating and their progress through the trial are shown in fig 1. There was no difference between the two groups in baseline demographic data or diagnoses (table 1) or in quality of life, except for the nausea and vomiting subscale of the EORTC (mean score patient held record group 10.09; control group 14.20; p=0.03; table 2).
Basic demographic characteristics and diagnoses of subjects in the study
Health related quality of life at recruitment

{kind=link}
Flow of patients through the trial.
CHANGE IN QUALITY OF LIFE
There was no statistically significant difference between the two groups in change in quality of life in any subscale over the 6 months of the study, although the change in score tended to be better in the group with the patient held record for all six subscales relating to function (table 3).
Mean differences between groups in changes in EORTC subscale scores at 6 month follow up (calculated as change in intervention patients minus change in controls; n=172 in each group)
PATIENT VIEWS AND PREFERENCES
There was no significant difference between the two groups in the number of patients reporting difficulty in understanding what was happening, remembering what healthcare staff said, asking about worrying things, or keeping health information private. However, significantly more of the patients allocated patient held record booklets reported no difficulty in preparing for their encounters with healthcare staff (table 4). When the degree of difficulty was taken into account, patients in the group with patient held records were significantly less likely than control subjects to find it “quite” or “very” difficult to monitor their own progress (23% v 12%; 95% CI of the difference 3 to 19; p=0.009). Those with a patient held record were also more likely to feel in control (73% v 84%; 95% CI of the difference 2 to 19; p=0.03). There was no significant difference between the two groups of patients in their perception of healthcare staff's knowledge of what was happening to them.
Patient perceptions (number (%) agreeing with structured statement)
One hundred and sixty four patients (48%) expressed a preference for the booklet (91 (53%) in the patient held record group v 73 (42%) in the control group; 95% CI of difference 0 to 21; p=0.052). Patients who preferred to have a booklet were younger (median 60 v 66 years; 95% CI of difference –7.95 to –2.55; p<0.001) and had more professionals involved in their care (median 2 v 1; 95% CI of difference 0 to 1; p<0.005). The reasons given by the 180 patients (52%) who preferred not to have a patient held record are summarised in table 5.
Preference comments made by patients
There were moderate and significant associations between patients' preference and how useful it was for them to refer to the patient held record (τb=0.48, p<0.001) or how helpful it was for them to write their thoughts down (τb=0.41, p<0.001). The association between patients' preferences and how easy it was for them to ask healthcare staff to write in their record booklet was significant but weak (τb=0.08, p=0.006).
USE OF PATIENT HELD RECORD
Of the 251 booklets given to patients, 150 (60%) were returned. The booklet was not recovered if the patient had died or could not be contacted (n=80); it had not been used (n=13); had been lost or stolen (n=7); or was too private (n=1). Six of those returned had also not been used and 144 were therefore analysed. The mean (SD) number of entries in the patient pages of each booklet was 13.56 (21.78), range 0–173). Seventy seven patients had used it as a diary and 43 as an aide-mémoire. In 115 booklets at least one professional entry was written as a record of the consultation, but only eight contained written explanations to patients. Forty four showed evidence of entries being used to communicate with other professionals.
Overall, evidence of deterioration was noted in 21 booklets. This was found in both the patients' and professionals' entries in 10 cases, only in patient entries in nine, and only in professional entries in two.
HEALTHCARE PROFESSIONALS' VIEWS AND PREFERENCES
Entries by 256 healthcare professionals were identified from the patient held records. However, not all of the entries could be distinguished, some were illegible, and some were initialled only. In some cases the professionals identified had retired or moved on to new jobs. As a result, 166 were sent a questionnaire. Of these 166 professionals, 74 remembered seeing the record and were asked to complete further questions. The professional disciplines are listed in table 6.
Number and percentage of different professional groups who had seen the patient held record (PHR)
Possible advantages identified included helping patients to remember what had been said to them (n=72 replies), facilitating communication between professionals themselves, (n=70) and facilitating communication with patients (n=69). Potential negative aspects included the possibility of greater litigation claims (n=19), increased patient anxiety (n=28), difficulty for patients who wish to keep information private (n=29), and an increase in paperwork (n=61). Fifty eight (78%) of those who remembered seeing the record indicated that they would prefer their patients to have it.
NHS RESOURCE USE
With regard to validity testing, paired t tests on continuous variables (number of GP surgery and home visits) showed no significant differences between the two data sources. Similarly, kappa statistics on dichotomous variables (GP surgery/home visit, yes or no) showed good agreement between data sources. Analysis of resource use was thus undertaken on patient recall data. Kappa statistics in the inter-rater reliability exercise varied between 0.54 and 0.90 for dichotomous variables, showing broadly good agreement.
Full resource use data were available on 344 patients. The results are reported in table 7 and show no significant difference in the number of contacts with any health professionals.
Resource use: mean (SD) face to face contacts over 4 week period
Of the 74 professionals who completed the questionnaire, 51 stated that the patient held record had no effect on length of consultations, 18 stated that it had lengthened consultation time (mean 5 minutes), and six that it had reduced it (mean 6 minutes). Overall, the use of a patient held record did not seem to affect consultation time.
The physical production cost of the booklet was £317 for 500 copies or roughly £1.26 per patient in the intervention group.
Discussion
This study has shown that, in patients with cancer, use of a patient held record does not affect quality of life but has a positive impact on quality by helping patients to feel more in control and to prepare for meetings with healthcare staff. It was used by patients primarily as a diary and an aide-mémoire. Although more than half the patients in the study expressed a preference not to have a patient held record, among those who had been allocated it there was a tendency to prefer it. Professionals tend to use it to communicate with other professionals rather than with patients. Of those professionals who remembered using it, most felt it was beneficial and preferred patients to have it, perceiving that this was of benefit in communication with patients, although evidence for this was found in only 28% of booklets. It had no impact on the number of contacts between patients and professionals.
Recruitment of patients to a study of this sort is not easy. Patients and relatives are often bemused and distressed by their diagnosis, and apprehensive about treatment and the future. We sought participation sensitively and did not try to persuade hesitant patients. As a result, many potential patients were not recruited (fig 1) but, nevertheless, the distribution of cases by cancer site (table 1) was representative of the workload of the oncology department. We gained no impression that refusal was due to any aversion to the principle of a patient held record. Our sample size predicted we would have 260 evaluable questionnaires at 6 months. In the event, 344 were analysed.
Our findings confirm those of Drury et al8 who found, in a shorter study in patients attending radiotherapy outpatients, no effect on satisfaction with communication, participation in care, or quality of life after 3 months. In addition, our study has shown the patient held record has a significant impact on aspects of communication associated with a greater involvement by patients in their own management, but no impact on those aspects which are more related to information seeking, retention, and understanding.
The overall involvement by professionals in the study was disappointing. Ninety of the 256 professionals who had used the booklet could not be identified, and only 45% of those contacted remembered seeing it. Although this is a relatively low percentage, it compares favourably with Drury et al8 who found that only 27% of GPs remembered seeing it. Despite little involvement, most professionals thought a patient held record would be of benefit to patients. The fear that it would increase paperwork echoes the findings of Teng Liaw15 but there was little anxiety that consultation times would be affected. It is likely, but not proven, that better education of both patients and professionals of the potential value of the patient held record might extend and enhance its use.
Since the intervention was not intended to influence clinical management, the failure to demonstrate any differences in NHS resource use is not unexpected. There was no effect on the number of face to face or telephone contacts, nor any clear influence on the length of consultation. These results are consistent with the Oxford study8 which also found no differences in major resource use categories between groups. The only cost attributable to the intervention is the cost of producing the booklet.
In conclusion, the patient held record is valued and helpful to some patients but has no significant impact on quality of life or NHS resource use. From our findings, we do not believe that patients should routinely be given a standard patient held record. We suspect the same benefits may be obtained by encouraging patients to use a notebook to write down their thoughts, worries or questions, and to keep their own record of medications and appointments, offering them the choice of a more structured patient held record if they so desire. In this way its use would be patient led rather than constrained by a professional agenda. We hope that greater awareness by professionals of the potential benefits to patients will extend the use and evaluation of patient held records to other areas of care.
What is already known on the subject
-
Patient held records give patients control over information, ensure that medication and other records are contemporaneous, and obviate the need for the clinical record to be immediately available in an emergency. Patient held records in cancer do not have any impact on quality of life or NHS resource use.
What this paper adds
-
Patient held records are valued by some patients with cancer, particularly those who are younger and have more professionals involved in their care. Some patients find the record burdensome.
-
The patient held record helps cancer patients to feel more in control and to prepare for meetings with healthcare staff.
-
Professionals tend not to use the record but, when they do, they find it of value.
Acknowledgments
JGW helped to develop the protocol, led the study team, and drafted the paper. WYC developed the protocol, supervised data collection, validated and analysed the data, and edited the paper. NC recruited patients, collected study data, and edited the paper. DRC designed the health economics data collection, monitored study progress, and edited the paper. SES reviewed the protocol, liaised with colleagues in oncology, monitored the progress of the study, and edited the paper. IF piloted the patient held record booklet, reviewed the protocol, advised on the qualitative content analysis, monitored the progress of the study, and edited the paper. BL reviewed the protocol, monitored study progress, validated data analysis, liaised with colleagues in primary care, and edited the paper. ML validated and analysed resource use data and edited the paper. KM collected and analysed data on booklet use and health care professional views and edited the paper.
The authors thank all colleagues in primary and secondary care who supported this study and used the patient held record in the care of patients, in particular Dr C Askill, Consultant Oncologist, Swansea NHS Trust, Singleton Hospital; Professor J Chamberlain, Chairman, South West Wales Cancer Institute, Swansea NHS Trust; Dr S Closs, Consultant in Palliative Medicine, Tŷ Olwen, Swansea NHS Trust, Morriston Hospital; Dr V Gajek, Consultant Oncologist, Swansea NHS Trust, Singleton Hospital; Dr T Joannides, Consultant Oncologist, Swansea NHS Trust, Singleton Hospital; Ms MT Noonan, Superintendent Radiographer, Department of Radiotherapy, Swansea NHS Trust, Singleton Hospital. Mrs M Buckley, Oncology Development Nurse, Velindre Hospital, Cardiff designed the original patient held record on which the study booklet was based. Ms Penny Wyatt piloted and refined the booklet. Dr Gordon Avery co-authored the original application and secured funding for the study. Drs Gilbey and Thevamanoharan, Cwmllynfell, Dr Hilliard and Partners, Scurlage, Gower, Drs Mathur and Patel, St Thomas, Swansea, Drs Smith and Rohman, Kings Surgery, Water Street, Port Talbot, Dr Weatherill and partners, Fforestfach, Swansea, Dr M Williams, Tabernacle Street, Skewen took part in a pilot evaluation of the patient held record and we are most grateful for their feedback following this. Mrs J Tomlinson, Mrs M Greer and Dr S Sullivan provided invaluable advice in the early stages of the study; Mrs Fiona Murphy, Project Manager of the Wales Office of Research and Development, provided continuing support throughout the study; and Mrs Gaynor Demery provided excellent clerical support. The authors would like to thank all patients, their carers, and health care professionals who took part in the study.
Funding: Wales Office of Research & Development.
Conflict of interest: none.