Article Text

Abstract
The importance of learning from medical error has recently received increasing emphasis. This paper focuses on prescribing errors and argues that, while learning from prescribing errors is a laudable goal, there are currently barriers that can prevent this occurring. Learning from errors can take place on an individual level, at a team level, and across an organisation. Barriers to learning from prescribing errors include the non-discovery of many prescribing errors, lack of feedback to the prescriber when errors are discovered by other healthcare professionals, and a culture that does not encourage reflection on errors together with why they occurred and how they can be prevented. Changes are needed in both systems and culture to provide an environment in which lessons can be learnt from errors and put into practice.
- patient safety
- adverse drug events
- medication errors
Statistics from Altmetric.com
After several decades in which it seemed that many healthcare professionals did not admit that medication errors happened, suddenly the opposite is true. Journals are running special features on errors, hospitals are setting up error reporting schemes, and the NHS is making reducing errors a priority. The increasing concern over medication errors has also resulted in a notable increase in research published on the subject in the last 10 years, as a Medline search reveals (fig 1).

Hits obtained using the search term “medication errors” on the Medline database for the years 1996–2000. Only those articles for which “medication errors” was the focus were included; all subheadings were also included.
From large studies of adverse events, based on reviews of the medical notes,1–4 we can estimate that 1–2% of inpatients are harmed as a result of medication errors.5 Another more detailed US study of drug related adverse events6,7 suggests that, of the different types of medication error (prescribing, dispensing and administration), prescribing errors account for the most harm. In the UK the Department of Health has recently set a target that serious errors in the use of prescribed drugs should be reduced by 40% by 2005.8 But how are we to achieve goals such as this?
One theme emphasised in recent documents produced by the Department of Health8,9 is the importance of learning from errors. The idea of learning from our errors is a laudable goal, but can we achieve it? This paper considers this question in relation to medication errors in general and prescribing errors in particular, and suggests that we have a long way to go.
LEARNING FROM ERRORS
The concept of learning from errors can be applied on many levels. Firstly, at the level of the individual we can reflect on our own errors and why they occurred and alter our practice accordingly. Secondly, at a team or department level we can learn from the errors of our colleagues in a similar way. Finally, on a larger scale the wider organisation—whether a trust, a health authority, or the entire NHS—can learn from errors reported collectively. Each of these aspects will be considered in turn.
Learning from our own errors
To learn from our own errors we first need to be aware that we have made them. There are two practical reasons why the nature and culture of healthcare organisations currently mitigates against healthcare professionals being aware of their errors.
Firstly, with some exceptions, there is an inherent lack of feedback with respect to medical treatment. In many other situations an error made will be immediately obvious to the operator—for example, when steering a car, any error will be instantly apparent and can be compensated for. However, the effects of drug treatment generally take longer to become apparent. Together with inevitable variation between individual patients in their response to drug treatment, this means that all but the most serious and immediate errors are not obviously identifiable from their outcomes.
Secondly, even where errors are discovered, this is often by someone other than the person originally involved. The systems of prescribing, dispensing, and administration of medication generally involve many different people, often of different professions. A doctor prescribes, a pharmacist or pharmacy technician dispenses, and a nurse administers. The dispensing and administration stages may also be checked by a second person. This is one of the strengths of such systems—there are many opportunities to identify and rectify errors before they reach the patient. However, this also means that details of errors identified are often not fed back to those who made them. This is particularly true for prescribing errors, where a pharmacist, nurse or patient may identify the error some time after the prescription was written.
Whenever prescribing errors are identified, the primary aim is to resolve them. The wrong dose will be corrected, the drug intended will be clarified with the patient or another healthcare professional and, in most cases, the error will be rectified before harm results. Feeding back to the prescriber is a lower priority. From a practical point of view this may be because of lack of time to identify and contact the prescriber concerned, or it may relate to feeling uncomfortable with the idea of pointing out a colleague's errors. Regardless of the reasons, the result is that the prescriber who has made an error is often completely unaware that this is the case and has no opportunity to learn from it.
Even where healthcare professionals are aware that they have made errors, many do not reflect on their errors and why they occur, or make changes to practice. The Department of Health publication “An organisation with a memory”8 emphasises the importance of distinguishing between passive learning (where lessons are identified but not put into practice) and active learning (where lessons are embedded into culture and practice), and suggests that active learning is what is needed. Active learning has parallels with “reflective practice”, an essential part of continuing professional development with which all healthcare professionals should now be familiar. It is therefore surprising that errors are not reflected upon to a greater extent. In a recent study of prescribing errors we identified doctors who had made potentially serious prescribing errors and interviewed them, asking why they thought the error occurred and how it could have been prevented.10 Many commented that they had not previously thought about prescribing errors and why they occur. Several subsequently commented that they had changed their practice or way of thinking following the interview. This suggests that prescribers are willing and able to reflect on their errors and change their practice accordingly, but that without external prompting they do not currently do so.
Humans learn through reflexive processes—acting, observing the consequences, and reflecting on how they could do them differently next time. Increasing the feedback between prescribing and prescriber could help to increase the efficiency of learning from errors at the individual level.
Learning from the errors of our colleagues
Learning from the errors of others is also valuable and increases the number of learning opportunities for each individual. However, as well as being subject to the same barriers as learning from our own errors, an additional barrier to learning from the mistakes of others is a culture in which medication errors are seldom admitted to or talked about.11,12
We need to develop a culture in which we are more willing to talk about our errors with our colleagues and increase the opportunities to learn from them.
Organisational learning
Classic management textbooks such as “The fifth discipline”13 emphasise the importance of learning from experience at an organisation level. It is therefore of note that one of the key objectives of “An organisation with a memory”8 was to advise the government on how to ensure that the NHS learns from its experiences and minimises the risks of avoidable harm. In the report the current state of knowledge regarding serious failures in health care was reviewed, together with the extent to which the NHS can learn from them. It was concluded that, although there is a wealth of experience on analysing and learning from adverse events at an organisation level in industries such as aviation and nuclear power, there has been very little in health care. In the words of the report: “the NHS has no reliable way of identifying serious lapses in standards of care, analysing them [ . . .], learning from them and introducing change [ . . .] to prevent similar events from recurring”.
In order to learn from errors at an organisational level, errors must first be reported and then they must be analysed in a meaningful way.
Reporting of errors
Many hospitals and healthcare organisations have now set up schemes for multidisciplinary error reporting so that common errors can be identified and action taken to prevent them. With the advent of the National Patient Safety Agency, this concept will soon be extended throughout England. However, there is often an assumption that reported errors represent all errors.14–17 There is little research into reporting of prescribing errors. However, for medication administration errors the evidence indicates that no one is aware of most of them and, even where someone is aware that an error has occurred, there are many reasons why it may not be reported. These include lack of time, fear of disciplinary action, belief that only serious errors should be reported, and uncertainty over what constitutes an error.18–21 It has also been suggested that, if an incident is perceived to be no one's fault, then it may not be considered an error and therefore not reported.18 Other quantitative studies confirm that self-reporting grossly underestimates the numbers of medication administration errors that actually occur.19,22 There is no reason to suggest that the situation is any different for prescribing errors.
While data based on incident reports are useful for identifying the errors that are most commonly identified and reported, it must be remembered that these represent the tip of the iceberg and that many other errors are unreported. Alternative approaches are needed to identify a much higher proportion of the errors that actually occur. Observation is generally accepted to be the most reliable method of identifying medication administration errors,23 while prescription review can be used to identify prescribing errors.24,25
Analysis of errors
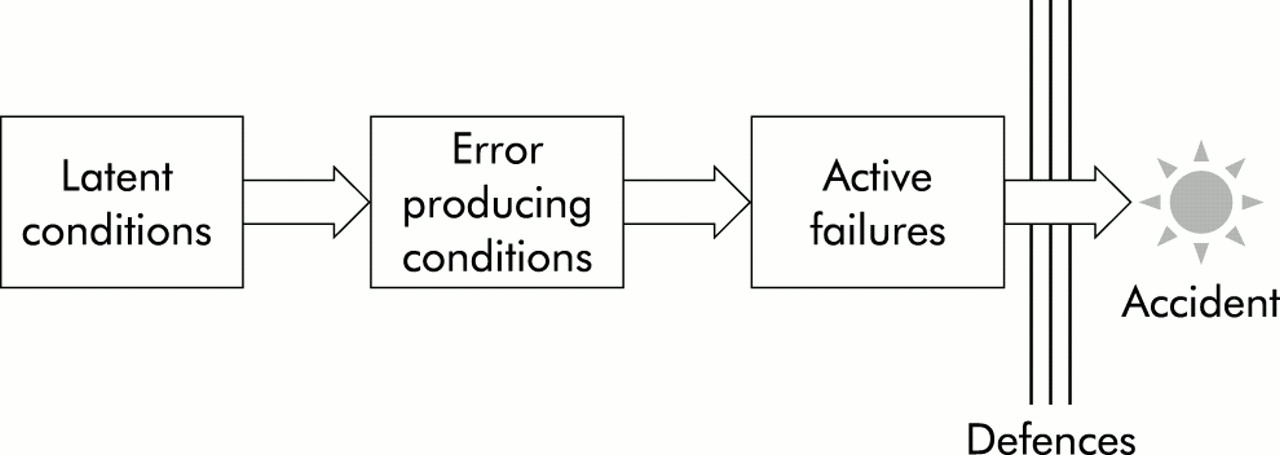
Once errors have been identified and reported in an organisation, the next stage is to identify the causes of the errors so that changes can be made in practice. This is not as simple as it first seems. Detailed investigations into a range of different industrial accidents often suggest that, while first impressions will suggest a specific cause—typically that an individual is “not doing his or her job properly”—further investigation reveals many deeper and more complex reasons. Models of human error such as Reason's “accident causation model” (fig 2)26 are helpful here. The accident causation model is based on the assumption that “active failures” on the part of front line individuals are largely the result of the conditions in which they work, often termed “error producing conditions”. These in turn are the result of fallible decisions at an organisational level known as “latent conditions”. Defences may or may not be able to prevent this chain of events from resulting in harm. There is therefore less focus on the individual who makes the error and more on pre-existing organisational factors. The advantage of using this approach is that it aids the identification of relevant latent conditions, the primary focus of intervention. Reason's model has now been used to investigate and analyse incidents in obstetrics,27 mental health,28 and other clinical settings. It has also been used to develop a protocol for the routine investigation of adverse incidents in hospitals29 and more recently it has been applied to prescribing errors.10
{kind=link}
{kind=link}
Reason's model of accident causation.26
NEAR MISSES
As well as learning from prescribing errors that reach and/or harm the patient, there is value in learning from “near misses”. Again, this applies at all three levels—the individual, the team, and the organisation.
Many accidents have the potential to produce serious injury but do not do so in practice, either because of some intervention or because of sheer good luck. By confining analysis and learning to the events that result in serious harm, we miss many important lessons for the future. There is no reason to expect that errors that cause harm differ substantially from those that do not. In industry it is generally accepted that, within a given domain, the incidence of events leading to major injury, minor injury, property damage, and minor incidents occur in a ratio roughly equivalent to 1:10:30:600, and that focusing on all events rather than just those that cause major injury results in more effective control of industrial accidents.30 While it would be expected that the ratio might be different in health care, the concept remains the same.
CONCLUSIONS
It has been argued that, while we need to learn from medication errors, there are many barriers that currently prevent this from occurring, particularly with respect to prescribing errors. To increase our opportunities to learn from errors the following three changes are required:
A more open culture is needed in which errors are openly discussed and reflected upon without fear of reprisal. Practical ways of increasing the opportunities to learn from our own and others' errors include discussing them at departmental meetings and circulating anonymised error reports.
A much wider appreciation is required of the value of focusing on the root causes of errors rather than on the individuals at the “sharp end” in preventing, analysing, and learning from errors.
Systems are needed that allow us to identify errors and feed them back to those involved. Without this, the other changes are worthless.
Key messages
-
Several recent publications emphasise the importance of learning from medical error.
-
Potential barriers to learning from prescribing errors include lack of awareness of errors, lack of feedback to the prescriber when errors are discovered by other healthcare professionals, and a culture that does not encourage reflection on errors and why they occur.
-
Changes in both systems and culture are needed to provide an environment in which lessons are learnt from errors and put into practice.