Article Text

Abstract
Background Family-activated medical emergency teams (MET) have the potential to improve the timely recognition of clinical deterioration and reduce preventable adverse events. Adoption of family-activated METs is hindered by concerns that the calls may substantially increase MET workload. We aimed to develop a reliable process for family activated METs and to evaluate its effect on MET call rate and subsequent transfer to the intensive care unit (ICU).
Methods The setting was our free-standing children's hospital. We partnered with families to develop and test an educational intervention for clinicians and families, an informational poster in each patient room and a redesigned process with hospital operators who handle MET calls. We tracked our primary outcome of count of family-activated MET calls on a statistical process control chart. Additionally, we determined the association between family-activated versus clinician-activated MET and transfer to the ICU. Finally, we compared the reason for MET activation between family calls and a 2:1 matched sample of clinician calls.
Results Over our 6-year study period, we had a total of 83 family-activated MET calls. Families made an average of 1.2 calls per month, which represented 2.9% of all MET calls. Children with family-activated METs were transferred to the ICU less commonly than those with clinician MET calls (24% vs 60%, p<0.001). Families, like clinicians, most commonly called MET for concerns of clinical deterioration. Families also identified lack of response from clinicians and a dismissive interaction between team and family as reasons.
Conclusions Family MET activations were uncommon and not a burden on responders. These calls recognised clinical deterioration and communication failures. Family activated METs should be tested and implemented in hospitals that care for children.
- Patient safety
- Healthcare quality improvement
- Hospital medicine
- Medical emergency team
- Paediatrics
Statistics from Altmetric.com
Background and significance
Rapid response systems are designed to reliably identify and act on deteriorating hospitalised patients outside the intensive care unit (ICU) setting. The system combines tools to identify deteriorating patients such as specific calling parameters and a response limb with a medical emergency team (MET).1 The effectiveness of rapid response systems in reducing arrests and in-hospital mortality for hospitalised children is demonstrated in two systematic reviews.2 ,3
Our hospital tested and implemented a clinician-activated MET in 2005 with the aims to reduce respiratory and cardiopulmonary arrests.4 Our MET is composed of five members: a nurse, respiratory therapist, resident physician, nurse manager and a critical-care fellow, a physician who is in critical care subspecialty training after completing a paediatric residency. The critical-care fellow is the designated team leader. Clinical staff can activate the MET if they have general concerns, or in the case of specific scenarios, such as if the patient has sustained tachycardia over 180 bpm or if the Paediatric Early Warning Score (PEWS) is elevated.5 While mechanisms such as PEWS assist clinicians in identifying signs of worsening illness, existing tools have moderate false negative rates.5 ,6
Families have a unique knowledge of their child's normal behaviour and temperament and may recognise significant changes before experienced clinicians.7 ,8 We believed that we were having failures to activate METs and that a mechanism for families to directly activate METs could improve our collective recognition of changes in the child's status, increase MET activations and reduce preventable codes. Family activation of METs is supported by a variety of patient safety and family advocacy groups including the US-based National Patient Safety Foundation and the Josie King Foundation. Recent studies of US children's hospitals with METs in place found that 69%–77% have some form of family activation process in place.9 ,10 While the experience with patient-activated and family- activated teams reported in the literature is generally positive, only a small number of studies exist, of which few present outcomes data.11–17 At our centre, we did not include direct family activation when we initiated our MET in 2005 due to three related concerns. First, clinicians worried that family activation would lead to a dramatically increased number of MET calls that might have an opportunity cost in care provided for other patients both for the nursing unit on which the MET was called as well as the responding team from the paediatric intensive care unit (PICU). Second, some worried that calls would be made for non-emergency medical issues (eg, late pain medication) and non-medical issues (eg, ‘dinner was cold’). Finally, leadership was concerned about the time burden for front-line clinicians to educate families about the MET, and the group did not want this to potentially distract from the success of a clinician-activated MET.
In the fall of 2007, our hospital leadership agreed to allow families to activate METs and made changes in our relevant policy. Our improvement team's aim was to develop a reliable process for—and education on—family activation of the MET. The improvement team gauged success, and tailored testing, through the count of family-activated METs per quarter, and qualitative data from nurses and families involved with family-activated METs. Now with a 6-year experience with family activation, we have three aims in this paper. To evaluate the burden of family activation on the clinicians involved, we describe our quality improvement intervention's effect on the number of family-activated METs. To better understand the outcome of METs, we compare the rate of PICU transfer for family versus clinician-activated MET calls. Finally, to begin to understand why families call METs, we compare the reason for MET activation by families with a set of age-matched and nursing unit-matched clinician-activated calls.
Methods
Context
Cincinnati Children's Hospital Medical Center is a 577-bed academic, freestanding children's hospital. At this project's start, the organisation had an infrastructure to support quality and safety interventions, an active family advisory council, and a history of partnering with patients and families on quality improvement interventions.18 ,19 Our hospital, including several members of our improvement team, performed additional improvement work aimed to improve clinical team situation awareness, beginning in late 2009 and continuing throughout the study period.20 Family activation of the MET was never a goal or measure for this improvement work.
Improvement
Improvement interventions
Our team developed and tested interventions to target our overall aim to make the family activation process better understood, reliably used, and accepted by our staff. We used the model for improvement and sequential plan-do-study-act cycles to develop and test changes.21 The interventions consisted of (1) mapping the family activation process with families, (2) an educational orientation for families on arrival at the nursing unit, (3) a poster that was displayed in the child's room and (4) a redesigned process of hospital operators answering phone calls. Collectively, our interventions targeted our programme theory that families have a unique expertise in identifying deterioration in their children and that family activation of MET would only be effective if families understood how and why to activate the MET. We undertook a series of improvement interventions in order to improve family understanding of, and then appropriate use of the MET.
Mapping the activation process with families
Our improvement team leaders worked with two groups of families: (1) the Family Advisory Council, which was made up largely of parents of children with chronic and often complex diseases and (2) a sample of families on our general paediatrics unit, where many of the hospitalisations are for acute illnesses in otherwise healthy children. We invited families of children hospitalised in our general paediatrics unit to an informal focus group where lunch was provided. Family input was sought in both venues in several specific areas: (1) how should families be educated on the MET and its calling? (2) when and how should this education best occur? (3) how should families activate the team? We then mapped out the education and activation process with families and elicited feedback to make focused changes.
Education to families on MET and activation process
Families told our team that the MET and its activation should be discussed on admission to the unit and that nurses should remind family about the team periodically. We educated bedside nurses on a step-by-step process to orient families to the poster and the MET during the admission assessment. We developed a brochure describing the MET and made it available on nursing units.
Poster displayed in each room
The families told our team that information on the MET should be present in each room. Our improvement team designed a poster that was displayed in each patient room (figure 1). We did not prototype the first poster with families. The posters were placed in each room in the initial test unit and then throughout the hospital. The poster was later changed significantly (figure 2) based on feedback from families that the initial message was confusing.
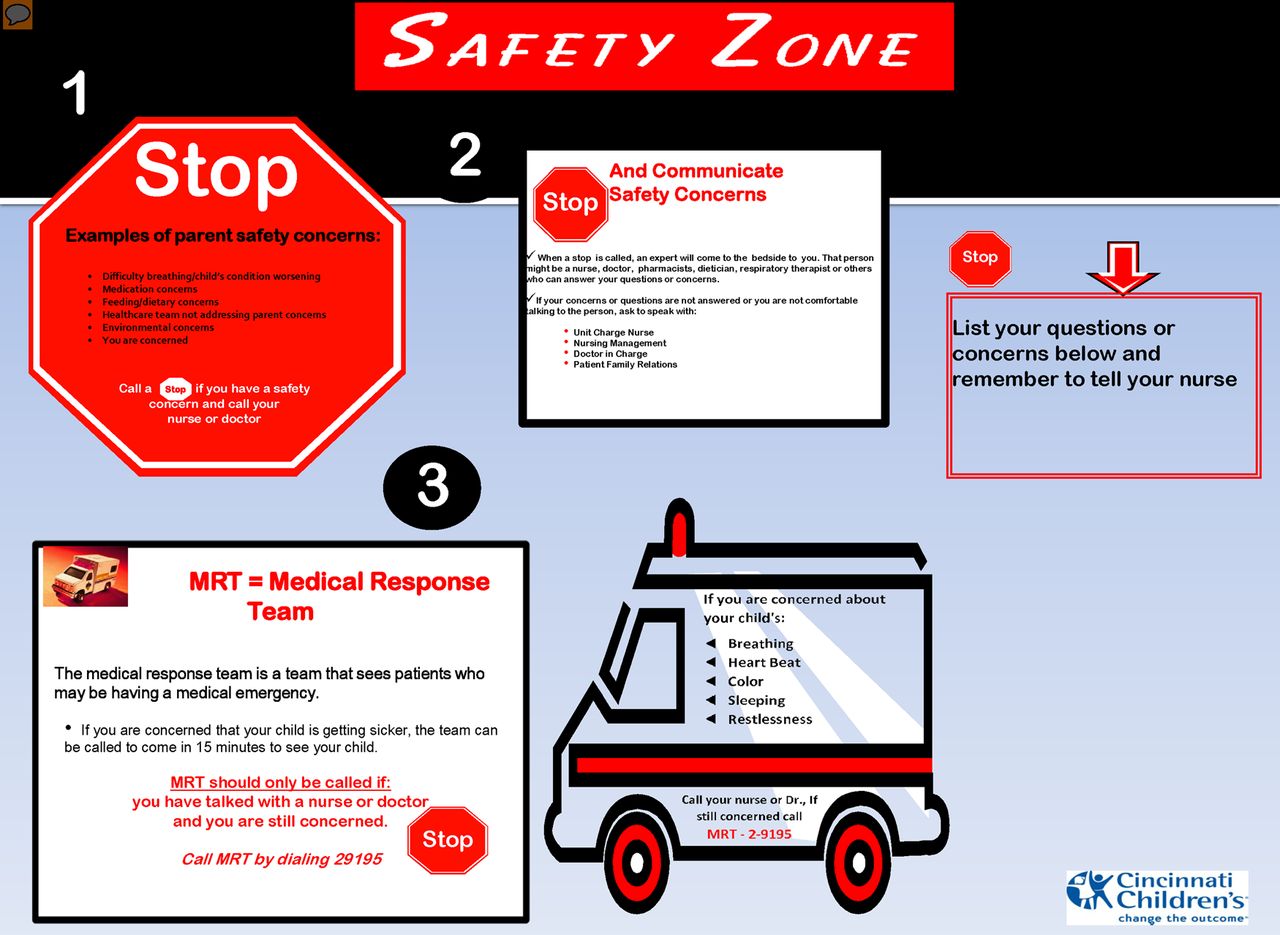
Initial version of medical emergency team poster in patient rooms.

Revised version of medical emergency team poster after family feedback.
Redesigned process for hospital phone operators
Families felt that they should activate the MET through the phone line system and that the same number should be used for families and clinicians. Nurses and physicians on the team caring for the patient were concerned that they might not know about MET calls placed by families, potentially delaying communication between the primary team and the MET. To mitigate this risk, an additional step was added to the telephone operator's workflow. The operator asked if the call was placed by clinician or family (with the name entered into a database). If the response was family, the operator would call the nursing unit to make the primary team aware.
Study of the improvement
We used quality improvement methods and statistical process control charts to assess our improvement interventions on rate of family activation of METs. Our study period was from 1 January 2008 to 31 December 2013. In a subset of MET calls (from 1 January 2008 to 31 August 2012), we additionally performed a retrospective cohort study to determine the association between family (versus clinician) activation and transfer to the ICU. In this subset, we then performed a nested case–control study to describe the reason for calling MET among family-activated METs and a 2:1 sample of clinician-activated calls matched by nursing unit and date of MET call.
Measures
Our primary measure for our improvement work was the process measure of family-activated MET calls. We collected these data through weekly review of medical records of all MET activations. The PICU fellow identified the caller of the MET using data from the hospital operator and the activating team. The fellow recorded the caller through a checkbox in a paper form from the start of our project until 10 January 2010 when our new electronic health record (EHR) included progress notes. This form was adapted into a templated note in the EHR at that time. Members of our study team (PWB, JZ and KG) validated the MET caller using other data in the EHR. Additionally, we collected data on whether a family concern was documented in the EHR for MET calls that were activated by clinicians. The rationale was that this might represent a second form of success in which the clinical team partnered with families to activate the MET or, alternatively, that this might have represented opportunities where families may have activated the MET themselves if they had better education on its function. We were unable to validate that family concern data were collected consistently.
For the purposes of this study, we also measured and reported on disposition to ICU after MET assessment as a percentage of all MET calls as stratified by family calls and clinician calls. We pulled these data from chart review. Finally, we performed a structured chart review to determine the reason for MET call for all family-activated calls and a 2:1 matched (on nursing unit and month of call) sample of MET calls that were activated by a clinician. Two reviewers (JZ and KG) reviewed each chart. Any disagreements were arbitrated by a third reviewer (PWB).
We tracked one context measure throughout the course of the project: nursing unit on which the MET occurred. Nursing ward was tracked through chart review as we believe that both culture and orientation processes at the microsystem level may ultimately influence success or failure.
Analysis
We used statistical process control with our primary process measure of family activated METs displayed on a u-chart.22 We used established rules for differentiating special versus common cause variation for this chart.22–25 Aditionally, we described family activated METs as a percentage of all METs. We next calculated the proportion of family-activated versus clinician-activated METs which was associated with transfer to the ICU within 4 h of activation. We compared these proportions using χ2 tests. For our determination of why the MET was activated, we first compared the agreement in reason identified by our two independent reviewers and generated a kappa statistic for agreement. The disagreements were arbitrated and a consensus reason, or reasons, chosen for each MET call. Finally, for family-activated METs related to clinical deterioration, we identified the clinical concern that prompted the call.
Results
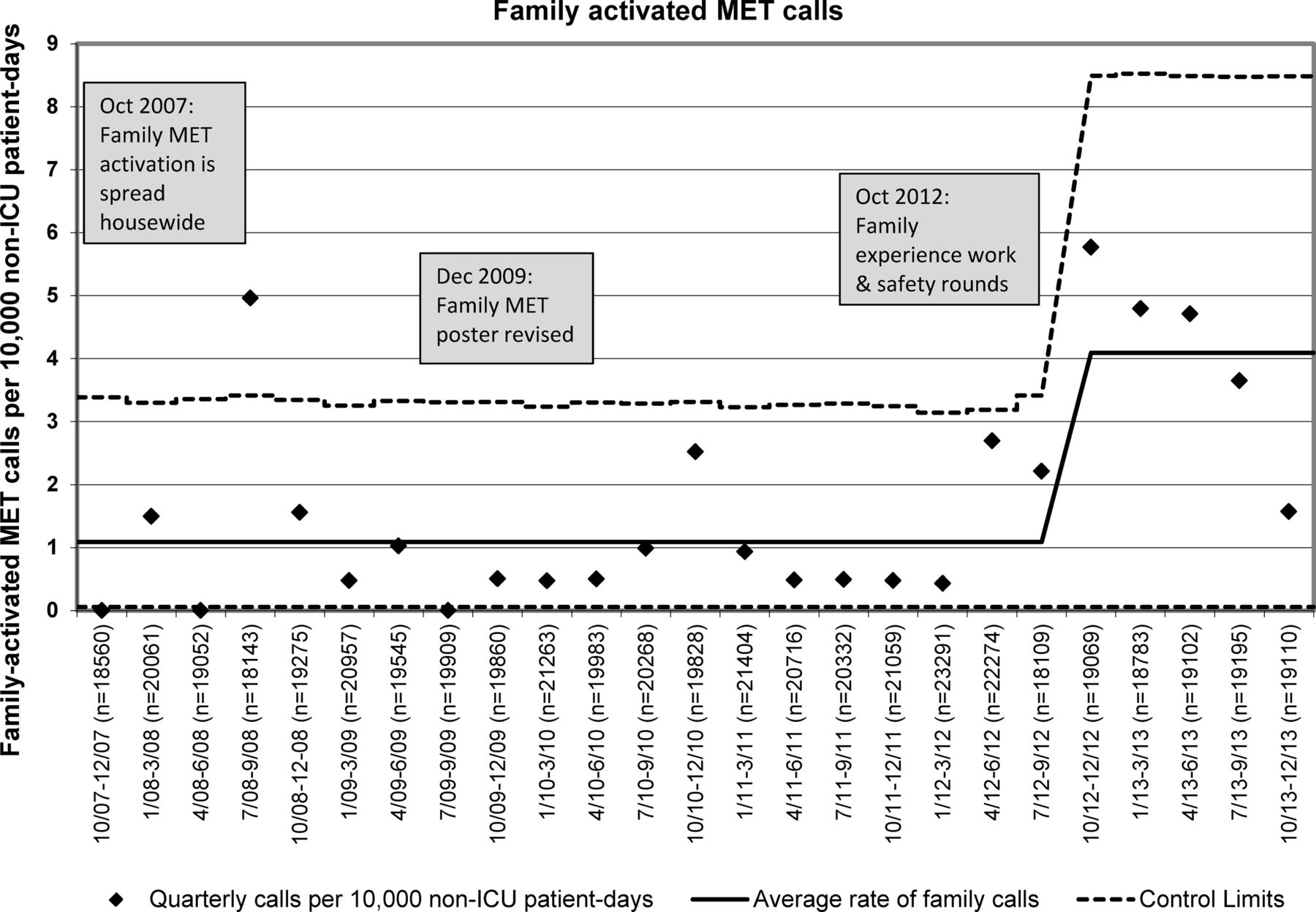
Over the 6-year study period, we observed a total of 83 family-activated MET calls. On average, families called 1.2 METs per month and 1.7 METs per 10 000 non-ICU patient days. Family MET calls, as a rate per 10 000 non-ICU patient days are displayed in figure 3. An increase in the rate of family calls was noted in the fall of 2012 as indicated by four consecutive points that fell outside the original control limits. The centre line was adjusted at this time as it was clear that special cause variation was occurring.22 The interventions were not part of our initial change package and were part of systems-level work in improving patient and family experience, specifically: (1) increased safety rounds by microsystem unit leaders where safety and MET activations were often discussed, (2) addition of a family advocate to our three-times daily huddle26 and (3) efforts to improve the detection and mitigation of threats to family experience. While the latter two interventions targeted family experience as the outcome measure, it may be that these efforts had the unintended but welcome consequence of increased family activation.
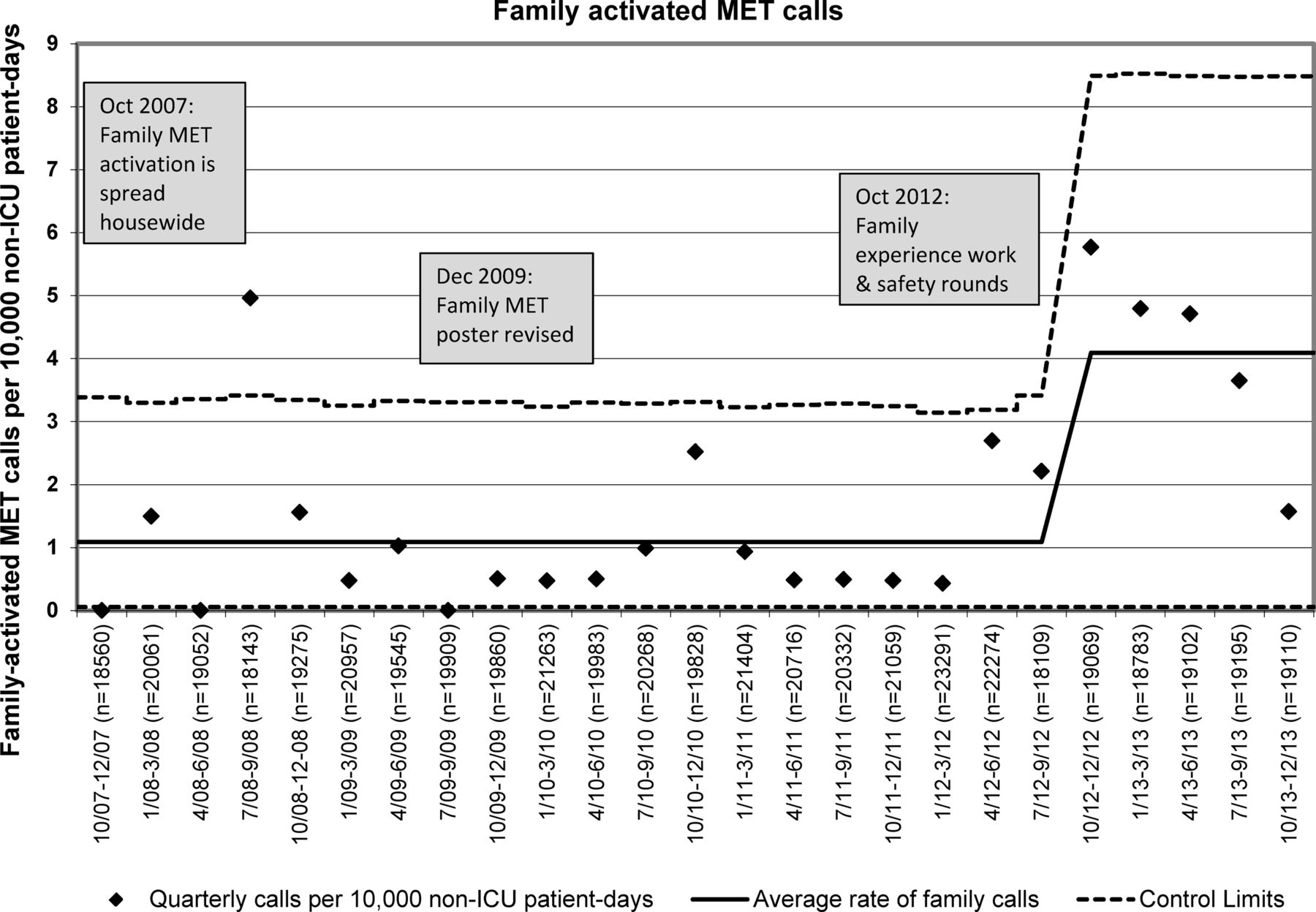
Family-activated MET calls over study period. ICU, intensive care unit; MET, medical emergency team.
Over this time period, we had a total of 2814 MET calls (average of 39.1 per month) with 2731 called by clinicians. We did have a large and significant increase in overall MET calls which is presented on an annotated run chart in figure 4. This occurred in October 2009 after elimination of informal ‘curbside’ ICU consults, requiring MET calls for any scenario where clinicians wanted to ask for ICU expertise as well as for all transfers from the floor to the PICU. A second increase occurred in our overall MET call rate after related but separate improvement work targeting clinician situation awareness as well as making the MET call necessary for transfer of cardiology patients to our cardiac ICU. Overall, family calls represented 2.9% of all MET calls. Our rate of codes outside the ICU per 1000 non-ICU patient days remained low and unchanged before and after our quality improvement interventions. Three of the eight MET-preventable codes had a family concern documented in the medical record but no MET activated before the event. Of the 2731 METs called by clinicians, 162 (5.9%) had family concerns noted in the MET note.

Total MET calls over study period. ICU, intensive care unit; MET, medical emergency team; PICU, paediatric intensive care unit.
During the 4.5-year period for which we examined the association between family versus clinician calling and disposition to ICU, 45 families called METs (table 1). We found complete data from chart review for 40 (89%) of these calls. During 2013, our busiest year to date of family activated METs, families called 2.3 METs per month. This is less than our average of 8.7 false-alarm calls per month of our code team that occurred during this same time period.
Disposition of family-activated versus clinician-activated METs
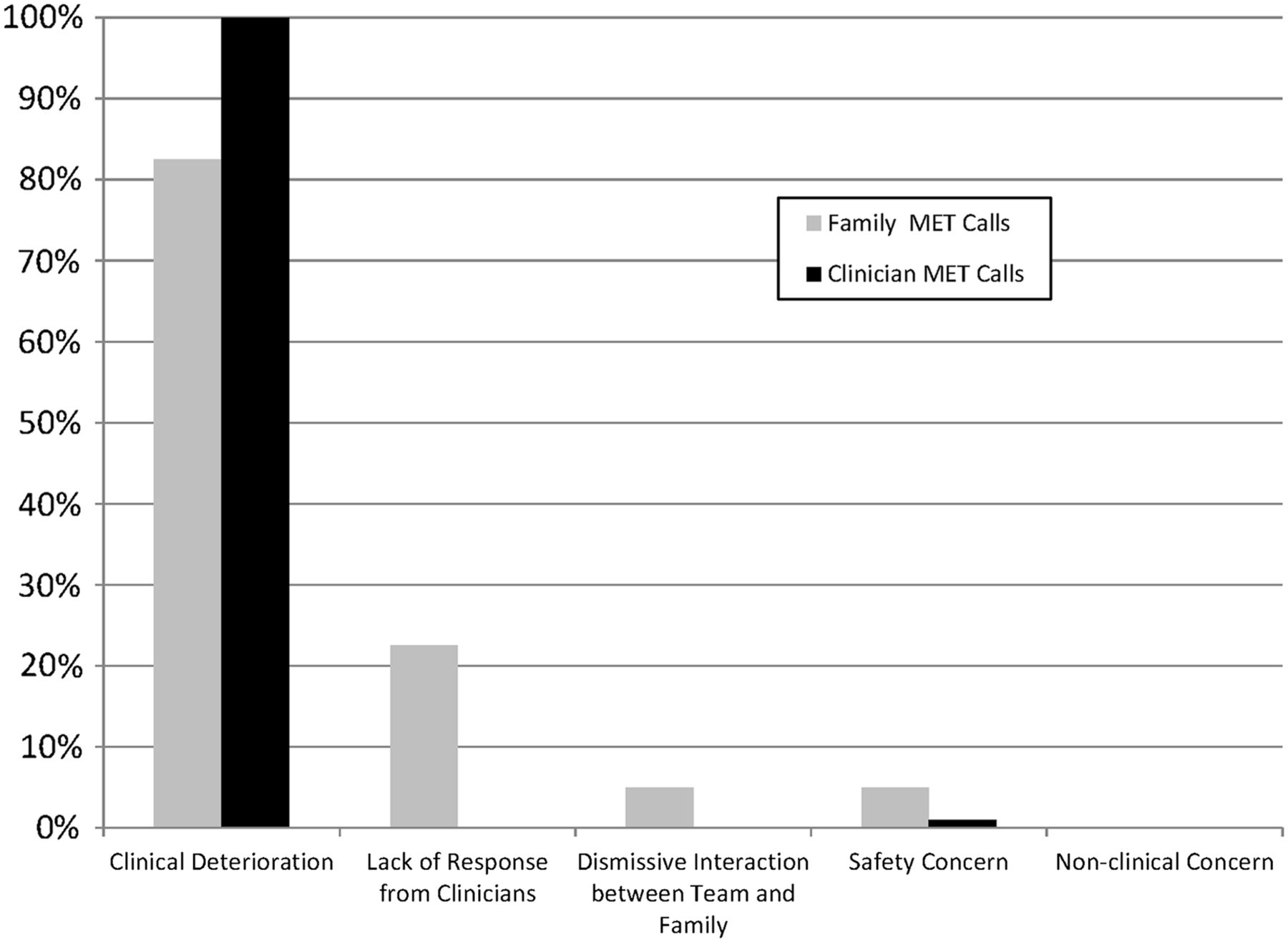
Families and clinicians activated METs for largely similar reasons (figure 5). Clinical deterioration was more commonly the reason for clinician-activated than family-activated calls. Families, but not clinicians, identified lack of response from clinicians (23% of calls) and a dismissive interaction between team and family (5%) as reasons for MET calls. Of the 37 family calls with clinical deterioration identified, 22 (59%) had the family's clinical concern identified. Families most commonly called on account of mental status change/agitation (n=6), breathing concerns (n=6) and pain (n=4). The kappa for classification of clinical deterioration was 0.67 for family-activated calls. For clinician-activated calls, one reviewer identified clinical deterioration as the reason for all calls and the other reviewer 99 out of 100. This resulted in near-perfect concordance and a kappa of 0.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Reasons (as percent of all medical emergency teams (METs)) of family-activated versus clinician-activated METs. Categories add up to more than 100% as seven METs had more than one reason identified.
During the study period, 14 of our 17 nursing units had family MET calls placed. No unit had more than six calls.
Discussion
In our 6-year experience with family-activated METs, families uncommonly activated METs. In the most recent and highest-volume year, families called 2.3 times per month on average. As a way of comparison, the hospital had an average of 8.7 accidental code team activations per month over this time. This required an urgent response from the larger team. Family activation less commonly resulted in ICU transfer than clinician-activated METs, although 24% of calls did result in transfers. This represents a subset of deteriorating patients that the clinical team may have missed. In both family-activated and clinician-activated MET calls, clinical deterioration was a common cause of MET calls. Families more consistently identified their fear that the child's safety was at risk, a lack of response from the clinical team, and that the interaction between team and family had become dismissive. To our knowledge, this study is the largest study of family-activated METs to date, both in terms of count of calls and length of time observed. It is also the first to compare reasons for MET calls from families with matched clinician-activated calls.
Over the 6-year study, families activated <3% of all METs. This represented just over one call per month and did not pose a substantial burden on the activating or responding MET. We are unaware of any reports on the ‘correct’ number of family MET calls, and we suggest that this number is likely quite context-dependent and related to organisational and microsystem culture, and how it promotes engaged and empowered families. In an organisation or microsystem culture where physicians and nurses often struggle to recognise a family's unique expertise on their child's status, a rational improvement goal would be more family-activated METs. Such activations would ensure that all of the team's (family's and clinicians’) expertise was used to escalate care, while broader safety culture interventions targeted better partnerships between families and the clinical teams. In this context, family-activated MET calls could be used to create a learning system around failed partnerships between families and clinicians. We have also observed at our centre that the ‘threat’ of a family calling an MET can empower a nurse to do so even when the physician team disagrees with the MET's necessity. An organisation with a more mature safety culture may view family-activated METs as a failure mode of family and clinical team partnership and see value in these calls being rare. At our centre, we are careful to not ever disincentivise anyone calling an MET, while learning from potential latent failures that preceded the call.
Family-activated METs less commonly resulted in transfer to the ICU than clinician-activated METs. A notable subset of family MET calls that did not transfer to the ICU, however, related to clinically relevant information (eg, difficulty breathing, worsening abdominal pain) that may not have been shared with the primary clinical team without family MET activation. This is one of several ways in which family activation of an MET may improve care without reducing MET-preventable codes outside of the ICU. The final main finding in our work was that families called METs for reasons related to changes in clinical status. Similar to clinician-activated METs, the most common reason families called METs was concern of clinical deterioration. Families also identified two subsets of concerns that would be quite difficult for the clinical team to identify and that could be associated with adverse safety outcomes: lack of response from the clinical team and an interaction between family and team that had become dismissive. A system that more reliably identified and mitigated such concerns from families would improve the quality and safety of care delivered. A previous study used the term ‘false positives’ to describe family-activated or patient-activated METs where a significant clinical concern was not identified.13 This may not be the most useful way to frame as we found that even when there was no clear evidence of clinical deterioration, family calls were very much ‘true positives’ for communication breakdowns that worsened family experience and increased the likelihood for safety events.
In other studies, MET calls from families or patients were uncommon. Activation of response teams in children's hospitals has been reported through two mechanisms: (1) direct activation by families of the same MET that responds to the clinician's calls (as used in our centre) and (2) activation by the family of a Condition Help team, which has distinct staff from the MET. The Help team consists of a patient advocate, unlike our MET team, and its calling criteria were more focused on communication breakdowns than clinical changes. In the largest paediatric study of family activation, Dean and colleagues found 42 patient and family calls of a Condition Help team at Children's Hospital of Pittsburgh.12 Another study of paediatric Condition Help reported two calls over a pilot period of 12 weeks.14 A family-activated MET programme at North Carolina Children's Hospital was activated just two times over its initial year.17 A similar family-activated programme at the Children's Hospital of Philadelphia had one activation over its first year.27 The longest study of patient and family activation found only 25 calls by patients or families over 2 years.13 As identified in a recent systematic review, there have been quite few rigorous efforts to promote family engagement in the acute care setting.28
Our study had several limitations. Our study of family MET activations compared performance with our historical controls, and we were unable to adjust for secular trends or unmeasured confounders. Our improvement team included leaders of our MET committee and patient safety, and we are not aware of any ongoing improvement work or systems change that might have affected family MET calls. We performed our interventions in a large tertiary care children's hospital with a history of improvement in patient safety and patient-centred and family-centred care. Additionally, it is uncertain and likely very context-dependent as to what is the ‘correct’ level of family-activated METs. This may limit generalisability to other centres, although the consistently low rate of family MET calls in the literature in a variety of contexts should reduce concerns related to responding team workload. We do not have process measures of how often MET education occurred for families and of how often families understood this information or felt empowered to call. This results in a limited understanding of the next best steps to improve family calling. Our data were collected in the course of clinical care with chart abstraction from structured clinical notes. Given this, it is possible that notes were not written for family MET calls that were judged ‘non-clinical.’ From our knowledge of the MET system, we are confident such calls are quite few, but we lack the data to quantify this. Our chart review for the reasons families called did not use a validated classification tool as we do not believe one exists. This is somewhat mitigated by our double independent reviews that demonstrated the reliability of our classification scheme.
In conclusion, our team developed a family MET calling programme that resulted in an increased but still quite modest number of family calls. Adding to the existing literature, family activation has not substantially increased the burden on our MET. Family-activated METs resulted in transfer to the ICU less commonly than clinician-activated METs; however, 24% of family-activated METs resulted in ICU transfers and substantial clinical deterioration may have been missed without this activation mechanism. Given the growing evidence of modest cost and potential benefits, we advocate for testing and adaptation of family-activated METs in all contexts. While other centres may choose different responding MET compositions or activation mechanisms, successful replication of our interventions should include partnering with patients and families in the design of the process and careful focus on how the MET activation process is introduced to families and then carried out. We found that many family calls that did not result in transfer identified critical communication concerns. We continue to have a number of family concerns that do not result in METs and believe we have not fully leveraged families’ unique expertise in identifying changes in their children's health status. More detailed understanding of why families do and do not activate METs is needed to better empower families. This understanding could lead to opportunities for co-production, with patients and families using design thinking.29 ,30 Such an approach will likely lead to broader and deeper clinician–family partnerships than our education and poster interventions.
Acknowledgments
We would like to thank our Family Advisory Council and all families that gave their time and expertise to improve this process. We also would like to thank Greg Ogrinc, Louise Davies, and the entire Standards for Quality Improvement Reporting Excellence (SQUIRE) writing group for their willingness to allow our writing team to use an in-draft version of SQUIRE (V.1.6) on this quality improvement report. The SQUIRE 2.0 development is jointly funded by the Health Foundation (UK) and the Robert Wood Johnson Foundation (US).
References
Footnotes
-
Contributors PWB had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. PWB: led the conception and design of the study and performed the analysis and interpretation of data. He drafted the initial manuscript and contributed in its revision for important intellectual content. JZ: contributed to the conception and design, analysis and interpretation of data, drafting of the initial manuscript and its revision for important intellectual content. She reviewed the family-activated and matched clinician-activated medical emergency team call charts. RB: led the improvement team on family activation of the medical emergency team and contributed to the conception and design of the study. He also reviewed and edited the manuscript for important intellectual content. DSW: contributed to the conception and design of the study and interpretation of data. He reviewed the entire manuscript for important intellectual content. KG: contributed to analysis and interpretation of data and reviewed the manuscript for important intellectual content. She reviewed the family-activated and matched clinician-activated medical emergency team call charts. MJG: contributed to the study design and execution and reviewed the manuscript for important intellectual content. KD: contributed to the design and execution of the initial improvement project and drafted the interventions section of the methods. She contributed to the manuscript for important intellectual content and reviewed the full manuscript. UK: contributed to the study design and execution and critically reviewed the manuscript for important intellectual content. SM: contributed to the study design and execution and critically reviewed the manuscript for important intellectual content. KT: worked with PWB in the conception and execution of the study and critically reviewed the manuscript for important intellectual content.
-
Funding Portions of this project were supported by cooperative agreement number U19HS021114 from the Agency for Healthcare Research and Quality. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality.
-
Competing interests None.
-
Ethics approval This study was reviewed by Cincinnati Children's Institutional Review Board (IRB) and deemed exempt research. Families that participated in the initial mapping of the MET activation process were approached by QI team leads and invited to participate in a brief discussion. No informed consent was sought for this QI process. A waiver of informed consent was sought and given by the IRB for the retrospective chart review on ICU transfer and reasons for activating MET.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement We have included in this manuscript our best and most relevant data to this work and do not have unpublished data of likely interest to your readership.