Article Text

Abstract
The role and value of theory in improvement work in healthcare has been seriously underrecognised. We join others in proposing that more informed use of theory can strengthen improvement programmes and facilitate the evaluation of their effectiveness. Many professionals, including improvement practitioners, are unfortunately mystified—and alienated—by theory, which discourages them from using it in their work. In an effort to demystify theory we make the point in this paper that, far from being discretionary or superfluous, theory (‘reason-giving’), both informal and formal, is intimately woven into virtually all human endeavour. We explore the special characteristics of grand, mid-range and programme theory; consider the consequences of misusing theory or failing to use it; review the process of developing and applying programme theory; examine some emerging criteria of ‘good’ theory; and emphasise the value, as well as the challenge, of combining informal experience-based theory with formal, publicly developed theory. We conclude that although informal theory is always at work in improvement, practitioners are often not aware of it or do not make it explicit. The germane issue for improvement practitioners, therefore, is not whether they use theory but whether they make explicit the particular theory or theories, informal and formal, they actually use.
- Evaluation methodology
- Social sciences
- Complexity
- Quality improvement methodologies
- Implementation science
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- Evaluation methodology
- Social sciences
- Complexity
- Quality improvement methodologies
- Implementation science
Introduction
Initiatives to improve quality and safety in healthcare all too frequently result in limited changes for the better or no meaningful changes at all, and the few that are successful are often hard to sustain or replicate in new contexts.1 Many of the difficulties of securing improvement lie in the enormous complexity of healthcare delivery systems, including their challenging technical, social, institutional and political contexts.2 But some challenges can be attributed to the persistent failure to take full advantage of informal and formal theory in planning and executing improvement efforts.3 It is of course possible to achieve high levels of quality and safety on the basis of intuition derived from experience alone, with little evident help from formal theory. The few successful examples that exist do not, however, help to build a science. In this article, we join others in arguing that the explicit application of theory could shorten the time needed to develop improvement interventions, optimise their design, identify conditions of context necessary for their success, and enhance learning from those efforts.4–9 The need for more effective use of formal theory in improvement is increasingly pressing, because personal intuition is often biased, distorted and limited in scope10 and the application of formal theory enables the maximum exploitation of learning and accumulation of knowledge, and promotes the transfer of learning from one project, one context, one challenge, to the next. We are concerned in this article with demystifying the nature of theory and making clear its many and various roles in carrying out and evaluating improvement, not with the place of theory in the vast (and often contentious) body of literature on the philosophy of science.
The users of theory
We begin by noting that the users of theory form a complex mix of constituencies with differing interests, both contrasting and complementary. Put simplistically, improvers—practitioners, managers and others at the sharp end—are interested in theory to the extent that it can help them do their work better. If they want theory at all, it is for its potential in helping them design and implement interventions with the greatest possible impact in their particular context, which is often small and local. For academic researchers, in contrast, theory itself is frequently the object of study, and their aim is to confirm, disconfirm or refine it. The working practices of researchers and improvers may be as different as their interests. Where hypothesis-testing clinical research may demand the development of and rigorous adherence to, fixed study protocols and invariant interventions, the same is not true of improvement work. Such work may instead rely on the repeated adjustment and refinement of interventions, often in a series of experiential learning cycles, and deploy interventions that are intentionally adapted in light of emergent information and evaluation.11–13 It is in part these differences in the interests and practices of improvers and researchers that explain the underlying distinctions between improvement projects and research studies.14 Yet it is possible and often very productive, to reconcile and combine them:
Understanding how individuals solve particular problems in field settings requires a strategy of moving back and forth from the world of theory to the world of action. Without theory, one can never understand the general underlying mechanisms that operate in many guises in different situations. If not harnessed to empirical problems, theoretical work can spin off under its own momentum, reflecting little of the empirical world.15
We also acknowledge that the term ‘theory’ itself can make people's eyes glaze over, because ‘theory’ is seen as something abstract, intimidating and irrelevant, especially when their immediate and true concern is the hard work at the sharp end of providing care, rather than theory itself. Yet the urge to find and use reasons—and thus to theorise—is irresistible; people look for explanations, understandings and causes easily and almost automatically, virtually every minute of the day, to the point where the social scientist Charles Tilly has suggested “We might…define human beings as reason-giving animals”.16 It is useful to understand as ‘theoretical’ any account that simply asserts that a meaningful interaction exists between variables (since this is a causal theory),17 as is any account that provides a coherent picture, in the form of a map or model, of a complex phenomenon or interaction, and that may describe how an independent variable changes the behaviour of a dependent variable (since this is an explanatory theory).18 (Prominent explanatory theories in natural sciences include the theory of evolution, the periodic table of the elements, and the double helix structure of DNA.) Thus, an improver who tells us that “Introducing a new guideline on care of urinary tract infections will reduce the rate of infection” is making a (causal) theoretical claim; she is making a different (explanatory) theoretical claim when she adds that “the guideline will do this by describing and justifying to practitioners the correct standards of care”.
The key challenge for practitioners is not simply to base their work on theory (they always work from implicit assumptions and rationales, whether or not they do so consciously), but to make explicit the informal and formal theories they are actually using. In this regard, Tilly usefully distinguishes a spectrum of theories.16 At the least structured end, reason-giving consists mainly of stories, an everyday ‘informal’ resource that is routinely drawn on as people seek to explain what they see, experience and learn. At the other, most structured, end are technical or ‘formal’ accounts: the specialised concepts that underpin the scholarly disciplines, especially the pure and applied sciences. How these more formalised theories might improve improvement, particularly when they are combined skilfully with informal, often unarticulated, theories based on personal experience, is our focus of interest.
Grand, big and small theories
For both improvers and researchers, we can make a very useful and important—though heuristic (rule of thumb)—distinction between grand theory, mid-range theory (‘big theory’) and programme theory (‘small theory’). Grand theory—such as a theory of social inequality, for example—is formulated at a high level of abstraction; it makes generalisations that apply across many different domains. Although such abstract or overarching theory does not usually provide specific rules that can be applied to particular situations, it does supply a ‘language from which to construct particular descriptions and themes’,19 and can reveal assumptions and world-views that would otherwise remain underarticulated or internally contradictory.
Middle (or ‘mid’)-range theories (in the vernacular, ‘big’ theories), were described initially by the sociologist Merton20 as theories that are delimited in their area of application, and are intermediate between ‘minor working hypotheses’ and the ‘all-inclusive speculations comprising a master conceptual scheme’. The initial formulation and reformulation of grand and mid-level theories tends to be the preserve of academic researchers, but such theories are often useful to improvers as frameworks for understanding a problem or as guides to develop specific interventions. For example, the theory of the diffusion of innovations21 ,22 is a mid-range theory whose use has become second nature to many improvers when, for example, they recruit opinion leaders, work through social and professional networks, make innovations easier to try and tailor innovations to make them consistent with existing systems. Similarly, Normalisation Process Theory,23 which describes how practices can become routinely embedded in social contexts, can play an important role in orienting people designing improvement interventions towards what is likely to be important, relevant and feasible in making their efforts successful.
Programme theories, on the other hand, provide what Lipsey24 terms a ‘small theory’ for each intervention. Pioneered by evaluation scientists,24–27 such theories are purposefully practical and accessible; they are also specific to each programme or intervention, even if they share much in common with other, similar, programmes and interventions. Ideally every improvement effort should have one. Concrete working models more than abstractions, programme theories typically accomplish two things. First, they specify the components of a programme (or intervention) intended to mitigate or solve the problem, the intervention's expected outcomes and the methods for assessing those outcomes (box 1), often in the form of a logic model or driver diagram.28 Second, they offer what the evaluation scientist Carol Weiss27 describes as a programme's ‘theory of change’, by which she means the rationale and assumptions about mechanisms that link a programme's processes and inputs to outcomes—both intended and unintended, as well as specifying the conditions (or context) necessary for effectiveness. A fully specified programme theory for an improvement intervention thus combines an (often diagrammatic) account of the intervention's components together with a narrative about the structures, behaviours, processes and contextual features that will be needed to achieve the aims and actions of the intervention (box 1 and figure 1).
Well-articulated programme theory
A Canadian programme sought to engage front-line health professionals in continuously improving the services they offered to people with chronic conditions.29 A programme theory-driven evaluation approach was used to describe the processes that might lead to the programme outcomes, and the conditions under which these processes were believed to operate. Using multiple sources—literature review, programme documents, committee meetings, observations, focus groups and interviews—a programme theory was developed. This took the form of a diagram (figure 1) and a narrative account of the theoretical basis of the intervention. The narrative identified relevant mid-range theories—including work motivation theory and reflective learning—as well as the importance of dissonance between actual behaviour, pursued goals and outcomes. It showed the relevance of these to components of the intervention, which included feedback, reflective learning and action planning.
The articulation of this theory helps in characterising the programme components, the mediating processes through which they work and the moderating factors related to participants and contexts, as well as improving the ability to measure the intervention's impacts on practice change.

Programme (impact) theory of an intervention to improve care of people with chronic medical conditions.
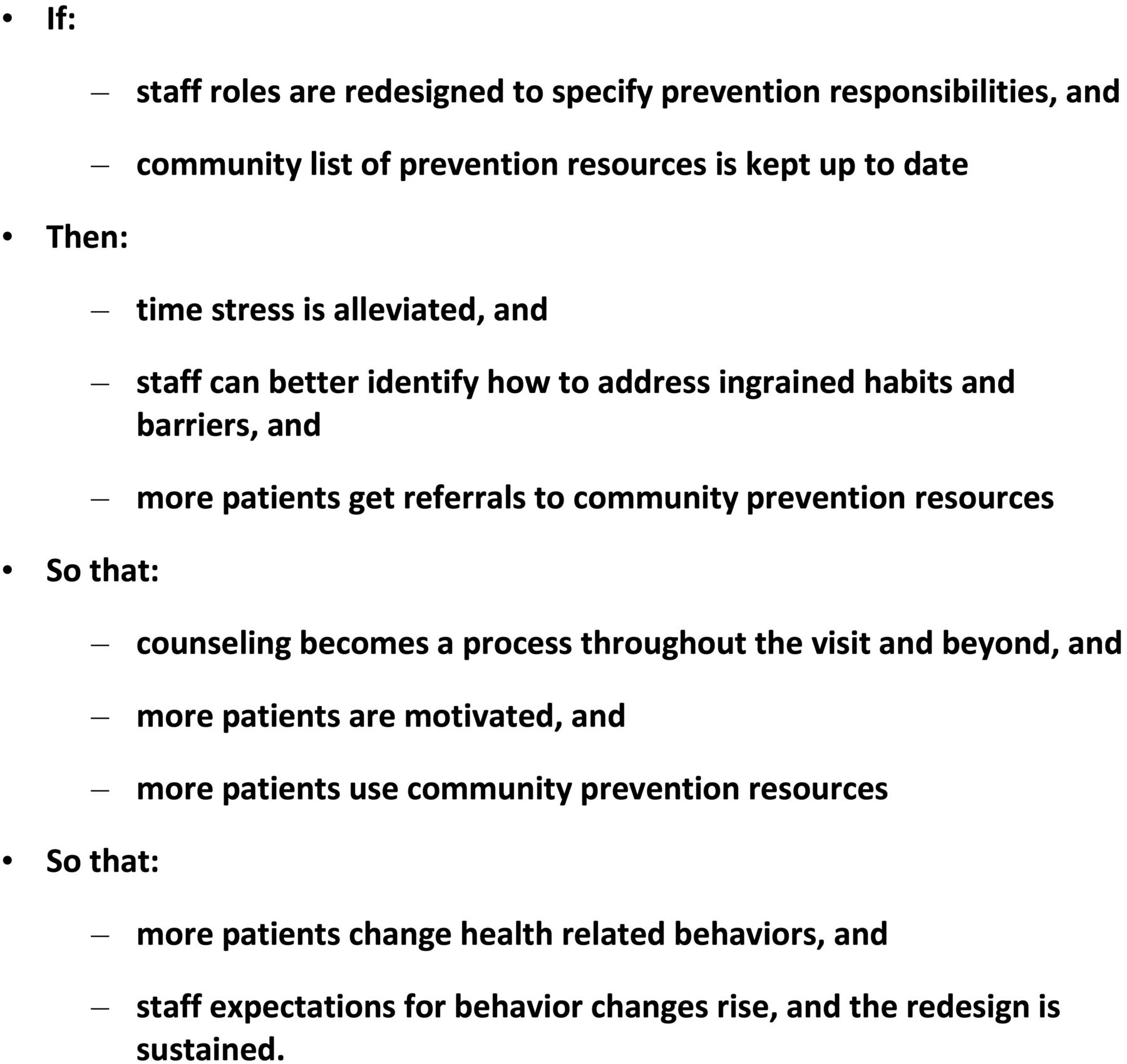
Meaningful programme theory uses the most appropriate possible combination of informal and formal theory to recognise dysfunction in care systems and identify its root cause(s); say what the corrective intervention is made up of (ie, its component parts); specify the range of likely outcomes (desired or not); indicate why it is likely to deliver the desired results (mechanisms); and describe how its impact will be assessed.24 As an example, The Ishikawa (‘fishbone’) diagram in figure 2 is an explanatory theory that pulls together the many barriers to the effective promotion of health-related behaviours in primary care practices and integrates them into a coherent map or model of the nature and sources of the problem being addressed.18 Figure 3 describes the presumed causal mechanisms that make up a theory of change in an initiative designed to overcome some of these barriers.30 This initiative modified the roles of clinic staff, making it possible for them to initiate counselling on tobacco and alcohol use, diet and physical activity as soon as patients registered for care. It also enabled the most effective use of each staff member's skills in implementing these preventive measures (eg, physicians advise patients on how to quit smoking, while ancillary staff refer patients to community resources for tobacco cessation and follow-up on participation). The causal theory underlying this example can be thought of as a series of if–then statements: “If staff take on more appropriate roles, then clinic time pressure and stress are alleviated; if time pressure and stress are alleviated, then staff, within their appropriate roles, are in a stronger position to address patients’ ingrained habits and motivate change.”

Ishikawa ‘fishbone’ diagram: explanatory theory of barriers in primary care to the support of health-related patient behaviours.

{kind=link}
{kind=link}
{kind=link}
Programme theory (theory of change) for overcoming barriers to the implementation of behaviour change interventions in primary care.
A key point is that articulating a programme theory is both feasible and practical, even for practitioners accustomed to ‘flying by the seat of their pants’. What the development of a programme theory can achieve is to shift improvement practitioners’ thinking from the implicit to the explicit, thus giving voice to the (often unrecognised) assumptions that guide their interventions, enabling the detection of any lack of consensus among team members, and surfacing weakness or incoherence in the proposed intervention's causal logic.
Importantly, a programme theory also plays an invaluable role in providing a framework for evaluation.11 ,24 ,28 This role is invaluable because all improvement work, whether or not it is intended to generate publishable new knowledge, needs to be designed in a way that makes it possible to know whether the intervention has actually resulted in improvements.31 Improvers need to pay careful attention to at least the following elements of evaluation: their choice of particular outcomes of interest (eg, changes in processes of care delivery; changes in patients’ clinical status; costs); the type of evaluation (quantitative; qualitative; mixed); the approach to interpretation of the data (eg, p-value driven; Bayesian; grounded theory); appropriateness of the evaluation methods for the intervention's phase of development11; and the procedures for data collection and standards for data quality.32–34
The consequences of failing to use theory or misusing it
Despite the potential value of theory, a striking feature of many improvement efforts is the tendency of its practitioners to move straight to implementation,33 skipping the critical working out of the programme theory; for example, sometimes only the source of the problem is identified but not an accompanying theory of change. Improvement interventions are also commonly launched without either a good outcome measurement plan or the baseline data required for meaningful time-series analyses.34–36 This rush to implementation often results in improvement interventions that, while attractive in concept, are not clear about the specifics of the desired behaviours, the social and technical processes they seek to alter, the means by which the proposed interventions might achieve their hoped-for effects in practice, and the methods by which their impact will be assessed.37 Moreover, published descriptions of what the intervention consists of are often, and unfortunately, remarkably poor.38 ,39
Failure to use the various elements of formal theory adequately has frustrated the efficacy and understanding of improvement interventions, and has inhibited the learning that can inform planning of future interventions. For instance, despite the ubiquity of audit and feedback interventions as an improvement technique, an initial Cochrane review40 was able to offer few useful recommendations on making this technique effective because of weaknesses in the theoretical underpinning of this review's analysis. An updated review41 using a method42 that drew on formal theory43 demonstrated that audit and feedback interventions were demonstrably effective when improvers using those methods included explicit targets and action plans in their interventions—exactly the kind of finding that is most helpful to those seeking to secure positive change.
Similarly helpful to practitioners is the way an explicit account of an intervention can help to avert ‘cargo cult science’. This phenomenon, first described by Richard Feynman,44 occurs when poor understanding of what an intervention really consists of, what it does, and how it works thwarts the meaningful replication of interventions that were successful in their original context.1 ,45 Without a good theoretical grasp of the underlying theory and its critical components (‘active ingredients’), improvers may adopt the label or outward appearance attached to a successful intervention, which does not permit them to reproduce its impact.46 This problem may help to explain apparently contradictory findings about the value of surgical checklists, for example.47–49
A well-founded theoretical account can also help to explain findings that otherwise appear baffling. For example, the inconsistent and relatively limited effectiveness of rapid response team systems in reducing mortality50 may be attributable at least in part to failure to create programme theories appropriate to the various phases of this initiative's development.11 As a consequence, these systems developed without clear and consistent rationales for the composition of the teams themselves, identification of appropriate target population(s) for their efforts, selection of the bedside interventions to be used in these diverse, complex clinical situations or standardisation of the methods for applying those interventions.51 ,52
Developing and applying programme theory
Developing a programme theory might, at first sight, appear daunting. But many of the tasks involved are relatively straightforward, and many stakeholders benefit from involving a multidisciplinary team in its creation. Various resources can be helpful in structuring thinking about programme planning and evaluation—including publication guidelines for improvement work, even when publication is not initially intended.53 Three points are important in this connection. First, few if any theories (whether grand, big or small) set out to be fully predictive of an intervention's feasibility or effectiveness, particularly when that intervention is a complex, multicomponent social treatment; rather, theories aim to provide frameworks for conceptual thinking and programme design, and help to generate additional theories (hypotheses) for testing. They must be kept under constant review, and updated in light of learning from the intervention's successes and failures in the real world. Second, and relatedly, people rarely proceed to action on the basis of formal theory alone,10 and rarely is it advisable to do so, since the deep knowledge of both mechanisms and contexts often evades formal capture in advance of implementation. Effective application of programme theories always relies on practical experience, contextual sensitivity, and well-informed judgment.54 Third, improvement programmes will often find it useful, when possible, to involve a social and/or behavioural scientist in the work: doing this can provide know-how in the development of programme theory and background knowledge in relevant mid-range theories. Such partnerships can be particularly valuable in refining or formalising theories before, during or even after the work is done.45
An improvement team is well-advised therefore to start by sketching out an intervention, then identifying its components and the relationships that link their application with the desired outcomes. To give their initial programme theory this added depth and specificity the team will need to articulate the assumptions that underlie the selection of the intervention's components and theory of change, then seek to assess those assumptions against relevant theories at higher levels of abstraction. Grand and mid-range theories can be especially helpful in generalising learning from situations that initially appear new and unique, in part by distinguishing proximal causes (the most immediate action that makes something happen) from distal causes (deeper structures that may lie behind patterns of effects).
Also important is the need to recognise and value the role of informal theories derived from personal experience, which are always at work in improvement efforts.19 Combined formal and informal theory can serve more effectively as the basis for decision-making and action than either kind of theory by itself.10 ,19 ,55 This is true both at the design stage, and when the intervention is being implemented, since the theories that underlie programmes often—usually—need to be updated in response to what is happening in practice. Review of the initial programme theory in light of combined informal-plus-formal theory can help detect the almost inevitable inaccuracies that occur early on in a programme, and help relevant features of context to come more plainly into view.56–58 Cultural, emotional and political challenges, including leadership and participant buy-in, as well as structural, educational and physical/technological influences, are all likely to become much more vivid as the work proceeds.58 ,59 The full meaning of kaizen—the widely used mantra in improvement, that ‘every defect is a treasure’—becomes particularly apparent when an improvement intervention stalls, or creates as many problems as it solves, because these frustrations call for the creative use of formal and informal concepts to modify the prior programme theory (box 2). Experiential learning theory,60 with its iterative ‘build-test’ cycles of four linked actions—hands-on experience with an action; observation-and reflection on that experience; using abstract concepts and generalisations to rethink or redesign the action; and testing the new version of the action—provides a useful framework for understanding how the updating of theory might optimally be undertaken. The ability to blend formal and informal theories effectively at all stages of interventions is an important applied skill that develops as a practitioner moves from novice to expert.19 ,61
Successful modification of an initial programme theory that proved to be ineffective: an example
Although the use of antenatal corticosteroid therapy to prevent respiratory distress and mortality in premature infants offers some of the strongest and most compelling evidence of benefit to be found in the meta-analytic literature,62 practicing obstetricians were slow to adopt the therapy throughout the 1990s. The then-predominant theory regarding widespread acceptance of medical advances was that publishing research reports about evidence-based practices and disseminating conference proceedings and guidelines through educational programmes, would be sufficient. The reality, however, was that the adoption of corticosteroid use in response to these measures was extremely disappointing.63 Leviton and colleagues64 responded to this frustration by moving away from the prior approach and searching for one that might encourage steroid use more directly. To accomplish this, these investigators conducted focus groups of obstetricians, and interviews with key informant perinatologists and neonatologists. These investigations revealed that obstetricians had largely been following a ‘watch and wait’ approach to manage premature labour, with the result that premature babies were frequently born before the therapy could be given. Also, obstetricians focused on the risk of maternal infection, since they were concerned that glucocorticoids would disguise it (they do not). Neonatologists, by contrast, recognised the benefits of the therapy because they managed the babies once they were born. These insights were highly compatible with the ‘big’ psychological theory of how the framing of risks and benefits affects perceptions of those risks and benefits.10 In response to these findings, the investigators then developed a simple practice guideline that was formally endorsed by the American College of Obstetricians and Gynecologists and became the new standard of care. This endorsement provided practicing obstetricians with further, much-needed expert reassurance about the efficacy and safety of the therapy, as well as high-level professional backing for its use—an ‘impact theory’ based on the efficacy of professional group solidarity rather than the previous educational approach. The use of corticosteroids subsequently rose 68% in hospitals receiving usual word of mouth dissemination, and 113% in hospitals receiving an active dissemination intervention, both of these effects being substantially greater than in most previous studies of guideline adoption.64
In important ways, this blending of informal and formal theories resembles the process of formulating accurate diagnoses in medical practice.65 As expert practitioners solve problems, they move back and forth among the observed realities of the problem being addressed, their own stored knowledge of formal theory, and their (often extremely large) repertoires of concrete examples, images, understandings and actions gleaned from experience. During this process they iteratively reframe their perception of the problem situation, and explore the impact of proposed interventions by conducting small tests of change (experiments), either virtually or in the real world.19 The value of combining informal and formal theory highlights the point that improvement interventions do not always need to flow deductively from established formal theories. Requiring them to do so could significantly stifle innovation, since in discovering and refining innovations “Personal experience, intuition and luck still play a role alongside rigorous science and rational thinking, and they probably always will.”66 Established pre-existing theory (eg, mid-range theory) is therefore best considered a resource, not a shackle. The important point here is that in order to increase the impact of interventions and the likelihood that others can replicate them successfully, improvers need to be explicit about what they are doing and why. Stated differently, they need to demonstrate that there is a reasonable expectation, based on what is already known, that a new intervention will work, and with a minimum of collateral damage. Box 3 provides a particularly useful example of the various roles theory can play in planning, executing and evaluating an improvement initiative. Of special note in this example is the interweaving of informal theories (some based on the improvement team's prior personal experience, others that emerged during the programme's implementation) and formal published theory identified early in the planning of the intervention. This intervention led to an increase in the facility's deep vein thrombosis prophylaxis performance to a level that met the Veterans Administration External Peer Review Programme national target.
Use of theories in an improvement project: an example67
Clinical problem:
-
Development of deep vein thrombosis (DVT) following surgery
Care delivery problem:
-
Inconsistent and inappropriate use of postoperative DVT prophylaxis
Goal of the intervention:
-
To increase proportion of eligible patients receiving postoperative DVT prophylaxis to at least 92% (national target set by Veterans Administration) in one US Veterans Administration hospital
Intervention:
-
Computerised decision support for writing postoperative orders, implemented within the hospital's existing electronic health record system
Middle-level theories:
Formal published theories that provided the initial rationale for design and implementation of the intervention
-
Diffusion of innovations21
-
Fit between Individuals, Task and Technology (FITT).68 Drawing particularly on the attributes of usability, compatibility, and relative advantage from Rogers’ theory of the diffusion of innovations,21 FITT postulates that the introduction of new technology leads to positive changes in care system only if the attributes of the user group, the characteristics of the implemented technology, and the affected tasks match each other
Programme theory:
Developed and refined by researchers in the course of designing and implementing the intervention; consisted of the following elements
▸ Explanatory theory:
– A coherent picture of the nature and source of the care delivery problem, obtained by integrating qualitative observations obtained during the study into a map or model of the care delivery problem
-
Lack of pressure for change from peers, leaders
-
Lack of information among physician staff regarding prophylaxis options, DVT risk categories
-
Non-linear, highly adaptive workflow of postsurgical management
-
Availability of multiple paths for writing postoperative orders
-
Prior prophylaxis guideline recommendations that were not aligned with local established surgical practice, culture
-
Lack of an effective and acceptable management tool that would reduce the burden, increase in accuracy and consistency in ordering DVT prophylaxis
▸ Logic model: Two Plan-Do-Study-Act cycles:
– First cycle: develop decision support
-
Form interdisciplinary quality improvement team; recruit advisory subject matter experts
-
Review published literature on clinical guidelines; collect DVT prophylaxis protocols from academic affiliates
-
Perform baseline study of cognitive tasks, ordering patterns and users’ workflow processes using non-participant observation and think-aloud protocols
-
Draft and implement initial computer-based order-entry menu
-
Test series of order-entry menu mock-ups and prophylaxis options, organised according to categories of patient risk; use surgeon feedback to build specialty-specific order menus
-
Mount educational campaign on purpose and design of new menus
-
Collect first-phase performance data
-
Second cycle: analyse human factors
-
Identify sociotechnical issues or barriers to implementation through observation, surgeon focus groups, chart reviews; categorise identified issues according to FITT model criteria
-
Engage clinical champions
-
Revise order menus
-
Create tracking systems (computer-based; manual chart review) for quantitative measurement of: (1) menu exposure; (2) use of new menu for writing prophylaxis orders; (3) total prophylaxis orders from any source
-
Develop system for validating completeness, accuracy of data on prophylaxis, contraindications to prophylaxis
-
Collect second-phase performance data
-
▸ Theories of social change:
– Identified by the improvement team; some of these, including the following, correspond to published general theories (described here in wording from Grol et al7)
-
Process re-engineering theory: Changing multidisciplinary care processes and collaboration instead of changing individual decision making
-
Cognitive theory: Taking into account professionals’ decision processes and their need for good information and methods in support of their decisions in practice
-
Theory on communication: Providing information from credible sources; framing and rehearsing messages; taking characteristics of messages’ recipients into account
-
Social network and influence theory: Local adaptation of innovations, use of local networks and opinion leaders in dissemination
Other theories were identified by the team as being relevant to the particular intervention and local context
-
Forcing functions: Helped to prevent use of ‘work-arounds’ (ie, alternative ordering mechanisms)
-
Buy-in: Created a sense of ownership by the incorporation of user suggestions into the new order system
-
Specificity of support tools: Application of order menu to individual patients at the point of care was facilitated by development of sufficiently prescriptive DVT risk criteria
-
Peer-to-peer influences and sociopolitical forces: Educational campaigns were developed to support these social forces (these proved to be relatively ineffective)
Theory, good and bad
Different disciplines sometimes have diverging views of ‘goodness’ (or quality) as it applies to theory, or indeed what constitutes theory at all. Some criteria for ‘good’ theory in improvement have begun to emerge, but their development is still very much a work in progress. Some criteria apply to virtually all theories in a given area of interest, while others are specific to the purposes for which particular theories will be used, or to their disciplinary origins. Emerging cross-disciplinary criteria might help users evaluate which theories are likely to be most useful for their purpose. For example, a recent consensus exercise of psychologists, sociologists, anthropologists and economists identified nine criteria for theories relevant to the area of behaviour change (box 4).69 ,70 Similarly, Grol et al7 have identified four important domains of theory related to the multiple layers of social and economic context required for success in changing the behaviour of providers and patients (actions of individual stakeholders; interpersonal interaction and social context; organisational context; and fiscal incentives, supports and constraints). Although uninhibited proliferation of theories of social change can be seen as problematical, the emergence of other such examples of ‘good’ theory is likely to be helpful as the field of improvement studies evolves.
Suggested criteria for ‘good’ theory in the area of behaviour change70
-
Clarity of theoretical concepts: ‘Has the case been made for the independence of constructs from each other?’
-
Clarity of relationships between constructs: ‘Are the relationships between constructs clearly specified?’
-
Measurability: ‘Is an explicit methodology for measuring the constructs given?’
-
Testability: ‘Has the theory been specified in such a way that it can be tested?’
-
Being explanatory: ‘Has the theory been used to explain/account for a set of observations?’ Statistically or logically?;
-
Describing causality: ‘Has the theory been used to describe mechanisms of change?’
-
Achieving parsimony: ‘Has the case for parsimony been made?’
-
Generalisability: ‘Have generalisations been investigated across behaviours, populations and contexts?’
-
Having an evidence base: ‘Is there empirical support for the propositions?’
Perhaps as important as the criteria for ‘good’ theory are the criteria for ‘bad’ theory; practitioners need to be alert to the possibility of being led astray by apparently attractive theories that may be partial, inappropriate for the context or flawed. A compelling recent example is the Stages of Change Theory, also known as the Trans-Theoretical Model. Although it has been widely used, evidence of its effectiveness is not supported by the results of careful systematic reviews. Indeed, in summarising these reviews, West notes that “…the problems with the model are so serious that it has held back advances in the field of health promotion and, despite its intuitive appeal to many practitioners, it should be discarded.”71
Conclusions
Theory need not mystify—or alienate—practitioners of improvement; it is not simply an arcane, abstract concept of interest mainly to scholars. Indeed, as Tolstoy put it, “The need to seek causes has been put into the soul of man”.72 Theory takes many forms, some informal, some highly structured: explanatory maps and models that make sense of complex situations; statements that call out testable causal relationships; sweeping generalisations that cover broad areas of interest; concrete descriptions of intervention methods and their mechanisms of action. Formal theory complements informal, experience-based theory, helping to define areas of dysfunction in healthcare systems, pinpoint their loci, and identify their possible mechanisms.18 It can provide frameworks that allow the accumulation of knowledge based on informal or small theories and empirical observations. For improvers and researchers, a well-formulated programme theory is likely to enhance the work of improvement, evaluation and research. Among other things, programme theories enable clarity about the components of a programme, the mechanisms through which the programme activities are thought to lead to the intended outcomes, the key outcomes to be assessed, plus the measurement tools, analytical approaches and data collection methods and standards that will be used.
In the near term, greater and more effective use of theory in improvement work could be usefully supported in a number of ways, for example: by identifying theory in publication guidelines as an essential element in doing, studying and reporting improvement work; by creating a publication guideline specifically devoted to the complete, precise reporting of the use of theory in improvement projects; and by developing a compendium of well-constructed reports that demonstrate the effective use of theory in actual improvement projects. Over the long term, a broad research agenda will also need to address the deeper aspects of theory as it is used in improvement. But the germane issue for improvement practitioners at this point remains not so much whether they use theory—they always do, even when they are not aware of it—but whether they make explicit and well-founded the theory or theories they actually use.
Acknowledgments
The authors are grateful for comments on earlier drafts of this paper by the members of the Health Foundation's Improvement Science Development Group.
References
Footnotes
-
Contributors The authors are listed in alphabetical order. FD led the drafting; all authors made major contributions to intellectual content, participated in writing and revision and signed off on the final draft.
-
Funding This paper was written with the sponsorship and general support of the UK Health Foundation, through the support of its Improvement Science Development Group.
-
Competing interests MD-W contribution to this article was funded by a Wellcome Trust Senior Investigator Award (WT097899) and was supported by University of Leicester study leave at Dartmouth College.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement This paper involves no original research data.