Article Text

Abstract
Background Numerous initiatives have focused on reducing device-associated infections, contributing to an overall decrease in infections nationwide. To better understand factors associated with this decline, we assessed the use of key practices to prevent device-associated infections by US acute care hospitals from 2005 to 2013.
Methods We mailed surveys to infection preventionists at a national random sample of ∼600 US acute care hospitals in 2005, 2009 and 2013. Our survey asked about the use of practices to prevent the 3 most common device-associated infections: central line-associated bloodstream infection (CLABSI), ventilator-associated pneumonia (VAP) and catheter-associated urinary tract infection (CAUTI). Using sample weights, we estimated the per cent of hospitals reporting regular use (a score of 4 or 5 on a scale from 1 (never use) to 5 (always use)) of prevention practices from 2005 to 2013.
Results The response rate was about 70% in all 3 periods. Use of most recommended prevention practices increased significantly over time. Among those showing the greatest increase were use of an antimicrobial dressing for preventing CLABSI (25–78%, p<0.001), use of an antimicrobial mouth rinse for preventing VAP (41–79%, p<0.001) and use of catheter removal prompts for preventing CAUTI (9–53%, p<0.001). Likewise, a significant increase in facility-wide surveillance was found for all three infections. Practices for which little change was observed included use of antimicrobial catheters to prevent either CLABSI or CAUTI.
Conclusions US hospitals have responded to the call to reduce infection by increasing use of key recommended practices. Vigilance is needed to ensure sustained improvement and additional strategies may still be required, given an apparent continuing lag in CAUTI prevention efforts.
- Infection control
- Hospital medicine
- Nosocomial infections
- Patient safety
Statistics from Altmetric.com
Introduction
Combating healthcare-associated infection (HAI) is a priority worldwide.1–3 Indeed, a variety of efforts to reduce HAI are underway globally. Large-scale efforts include the WHO Patient Safety Clean Care is Safer Care programme,3 surveillance and prevention efforts by the International Nosocomial Infection Control Consortium in America, Africa and Europe,4 ,5 and the European Union-funded ‘Prevention of Hospital Infections by Intervention and Training’ (PROHIBIT) consortium.6 Likewise, HAI prevention initiatives have been undertaken within a number of individual countries, such as the Matching Michigan programme in England,7 the HAI prevention programme established by the Australian Commission on Safety and Quality in Health Care,8 and required participation in regional infection prevention collaboratives for certain hospitals in Japan.9
In the USA, reducing HAI is an agency priority goal for the Department of Health and Human Services (HHS).1 ,10 In 2008, HHS established a federal steering committee that subsequently developed a National Action Plan to Prevent HAIs, with an explicit goal of reducing central line-associated bloodstream infection (CLABSI) rates by 50% and catheter-associated urinary tract infection (CAUTI) rates by 25%.1 In 2010, all 50 states as well as the District of Columbia and Puerto Rico submitted HAI prevention plans, and preventing HAI was identified as a Healthy People 2020 objective.2 ,11 In 2011, Partnership for Patients, a public-private partnership, was established to make hospital care safer and included a concentrated focus on HAI.12
This increasing emphasis on preventing HAI has been a call to action13 and has been accompanied by a number of specific efforts to achieve this important goal. Hospital payment policies from the Centers for Medicare and Medicaid Services, which removed payment for certain HAIs, began in October 2008.14 Required by section 3008 of the Affordable Care Act, strategies that link HAI outcomes to payment reductions have continued to expand with payment changes starting in October 2014 that compare hospitals nationwide using two composite scores—one generated from claims data and one generated from CAUTI and CLABSI rates as reported to the National Healthcare Safety Network (NHSN).15 A second programme, the Hospital Value-Based Purchasing Program, will also include an increasing number of HAI measures in upcoming years.16 Finally, public reporting of infection rates has been mandated by some states and as part of the Hospital Inpatient Quality Reporting Program.17 ,18
Largely in response to these payment and reporting policies, a number of large-scale infection prevention efforts have been launched, including collaboratives established as part of Hospital Engagement Networks and the Agency for Healthcare Research and Quality's ‘On the CUSP’ initiatives.11 ,19 These collaborative efforts bring together groups of hospitals that receive information and guidance from experts on implementing evidence-based practices or bundles of practices to prevent HAIs. Several of these initiatives have focused specifically on preventing device-associated infections. Accordingly, data from the Centers for Disease Control and Prevention (CDC) suggest that certain device-associated infection rates in the USA appear to be declining and that device-associated infections are contributing less to the overall HAI burden of disease compared with prior estimates.20 The specific actions taken by hospitals that may contribute to these changes, however, have not been described. Therefore, we sought to evaluate the use of key practices to prevent device-associated infections by US acute care hospitals from 2005 to 2013 to ascertain how hospitals have responded to these various policy changes and to identify potential opportunities for even greater improvement in reducing device-associated infections.
Methods
Study design and data collection
Data for this study were collected as part of an ongoing project focusing on infection prevention practices in US hospitals.21 ,22 In spring of 2005, 2009 and 2013, we conducted a survey of infection preventionists at a national random sample of non-federal US hospitals that asked about use of practices to prevent device-associated infections, including CLABSI, ventilator-associated pneumonia (VAP) and CAUTI. The survey that was mailed to each hospital was addressed to the infection control coordinator. Instructions provided on the first page of the survey indicated that if there was more than one infection preventionist the instrument should be completed by the infection preventionist who supervises and/or coordinates the other infection preventionists. The original hospital sample was selected by identifying all non-federal, general medical and surgical hospitals with 50 or more hospital beds and with medical/surgical or cardiac intensive care beds using the 2005 American Hospital Association Database. Hospitals were stratified by bed size (50–250 vs >250 beds), and a random sample of 300 hospitals from each group was selected, resulting in an initial sample of 600 hospitals. The same hospital sample was used in 2009 and 2013 with a slight reduction in the number due to the closure or merger of some hospitals since the original sample was identified. In 2009 the survey was sent to 578 hospitals, while the 2013 survey included 571 hospitals.
The survey process for all years followed a modified Dillman approach.23 In 2005 an initial mailing was sent with a $10 incentive, followed by a 2-week reminder letter, and a second mailing of the survey after 4 weeks to those who had not yet responded. In 2009 a third survey mailing was added due to a lower response to the first two mailings, which occurred at the height of H1N1 preparations. In 2013 a fourth reminder survey was sent to non-respondents at 4 months after the initial mailing to achieve a similar response rate as in the prior surveys.
Study measures
The main outcome for our analysis is a binary variable (0/1) indicating regular use of evidence-based recommendations to prevent CLABSI, VAP and CAUTI. The survey included questions about a number of different practices related to each type of device-associated infection based on guidelines published by the CDC and expert guidance from professional organisations such as the Society for Healthcare Epidemiology of America and the Infectious Diseases Society of America.24–29 The specific practices included in this analysis are practices that were included in all three rounds of the survey, which includes practices that are recommended for use by all hospitals, some that are considered special approaches when infection rates are not controlled and some that are not recommended for routine use (see online supplementary appendix). Respondents were asked to rate the frequency of use for each practice on a scale from 1 to 5 (1 being ‘never use’ and 5 being ‘always use’). Regular use of a practice was defined as receiving a rating of 4 or 5 whereas values of 1–3 were considered reflective of lack of use of a practice on a regular basis. Information about general hospital characteristics, including intensive care unit (ICU) beds, affiliation with a medical school, presence of hospitalists and some characteristics of the infection control and prevention programme, such as the number of full-time equivalent infection preventionists and whether the lead infection preventionist was certified in infection control, were also collected. Respondents were also asked whether their facility was involved in a collaborative effort to reduce HAIs (such as a Keystone project, the Pittsburgh Regional Health Initiative, or Institute for Healthcare Improvement). The number of acute care hospital beds was obtained from the American Hospital Association survey data.
Statistical analysis
Taking into account our stratified sampling approach, the survey data were analysed using sample weights based on the original probability of selection within each stratum resulting in estimates that represent the full population of non-federal acute care hospitals with 50 or more hospital beds and an ICU. Results are reported as weighted means or proportions with 95% CIs. Also, given the differential probability of selection, and the clustering by hospital across the three waves of the survey, results were estimated as a weighted longitudinal panel design. The reported p values, which compare percentages across years, were generated using generalised estimating equations with a logit link and robust SEs with probability weights, accounting for the inherent clustering by hospital and non-independence of the residuals and the heterogeneous weights. All reported p values are two-tailed and all analyses were conducted using Stata V.13.0 (StataCorp, College Station, Texas, USA). Statistical significance is defined as a p value of ≤0.05.
Results
The overall survey response rate was approximately 70% for all three study years. Selected hospital characteristics across years are shown in table 1. Significant increases were observed in the per cent of hospitals that reported using hospitalists (57% in 2005 vs 75% in 2009 vs 85% in 2013, p<0.001) as well as the per cent reporting participation in a collaborative effort to reduce HAI (42% in 2005 vs 68% in 2009 vs 82% in 2013, p<0.001). There was also a significant increase in the number of full-time equivalent infection preventionists per 100 hospital beds, from 0.67 in 2005 to 0.91 in 2013.
Hospital descriptive information (weighted, mean or proportion with 95% CI)
Practices to prevent CLABSI
There was a general increase in the use of most CLABSI prevention practices from 2005 to 2013 (figure 1). The use of two key recommended practices—maximum sterile barrier precautions during central line insertion and chlorhexidine gluconate for insertion site antisepsis—showed a substantial increase between 2005 and 2009 (71–90% and 69–95%, respectively) with both practices reportedly being used by nearly 100% of responding hospitals in 2013. The per cent of hospitals using an antimicrobial dressing with chlorhexidine also increased significantly over time (25% in 2005, 54% in 2009 and 78% in 2013, p<0.001), while use of antimicrobial-coated catheters remained relatively flat with about a third of hospitals reporting their use at each study time point. Also, the per cent of hospitals with an established surveillance system for monitoring CLABSI rates facility-wide significantly increased, from 52% of hospitals in 2005 to 66% in 2009 to 90% in 2013 (p<0.001).
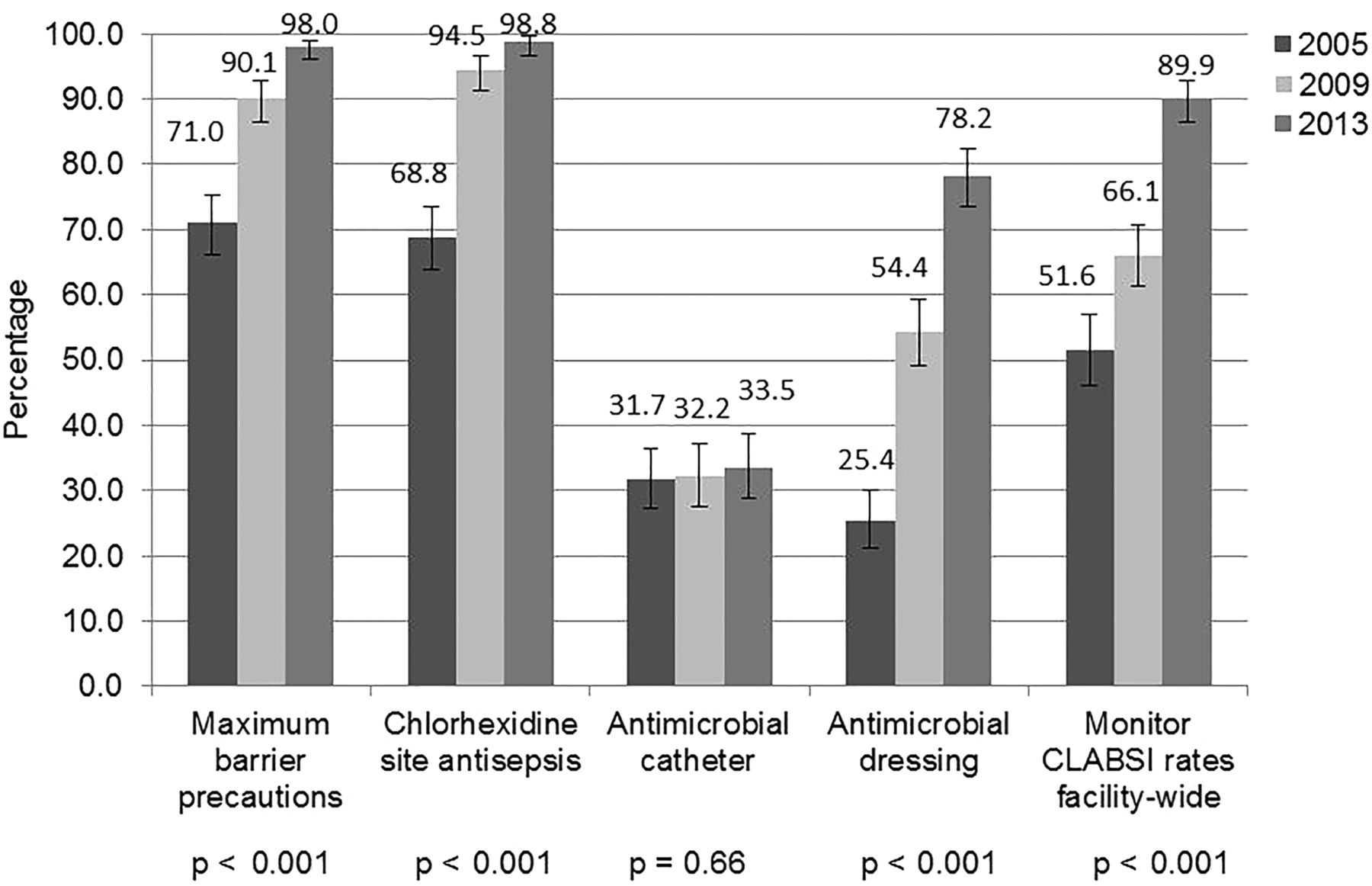
Per cent of hospitals that regularly use practice to prevent Central Line-Associated Bloodstream Infection (CLABSI).
Practices to prevent VAP
The percentage of hospitals reporting the use of most VAP prevention practices also generally increased over time (figure 2). The most commonly used practice at all three time points was semirecumbent positioning: 82% reported use of this practice in 2005, 95% in 2009 and nearly 100% of hospitals in 2013 (p<0.001). Significant increases were also noted in the use of an antimicrobial mouth rinse with a nearly doubling in the per cent of hospitals using this practice (41% in 2005 to 79% in 2013), as well as in the use of subglottic secretion drainage (21% in 2005, 42% in 2009 and 55% in 2013, p<0.001). The use of topical and/or systemic antibiotics for selective digestive tract decontamination also increased over time but remained the least commonly used of the practices assessed for preventing VAP with 13% of hospitals reporting its use in 2005 and 25% in 2013. Finally, there was some increase in the per cent of hospitals with an established surveillance system for monitoring VAP rates facility-wide: 34% in 2005, 39% in 2009 and 43% in 2013 (p=0.02). However, more than 50% of facilities reported having an unit-specific surveillance system for monitoring VAP in all 3 years for a combined rate of greater than 90% of facilities having some type of monitoring (facility-wide and/or unit-specific) in 2005, 2009 and 2013 (data not shown).
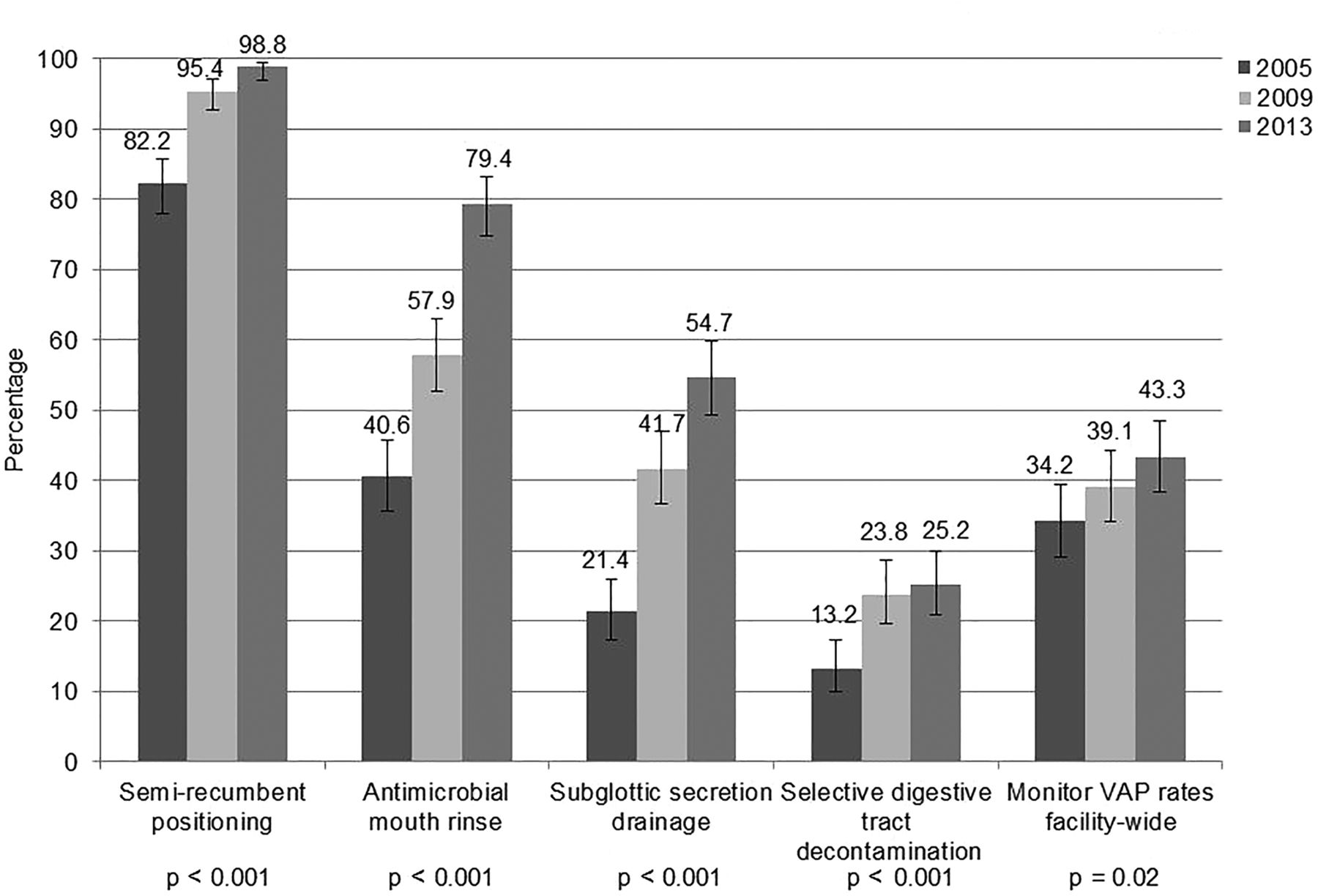
Per cent of hospitals that regularly use practice to prevent Ventilator-Associated Pneumonia (VAP).
Practices to prevent CAUTI
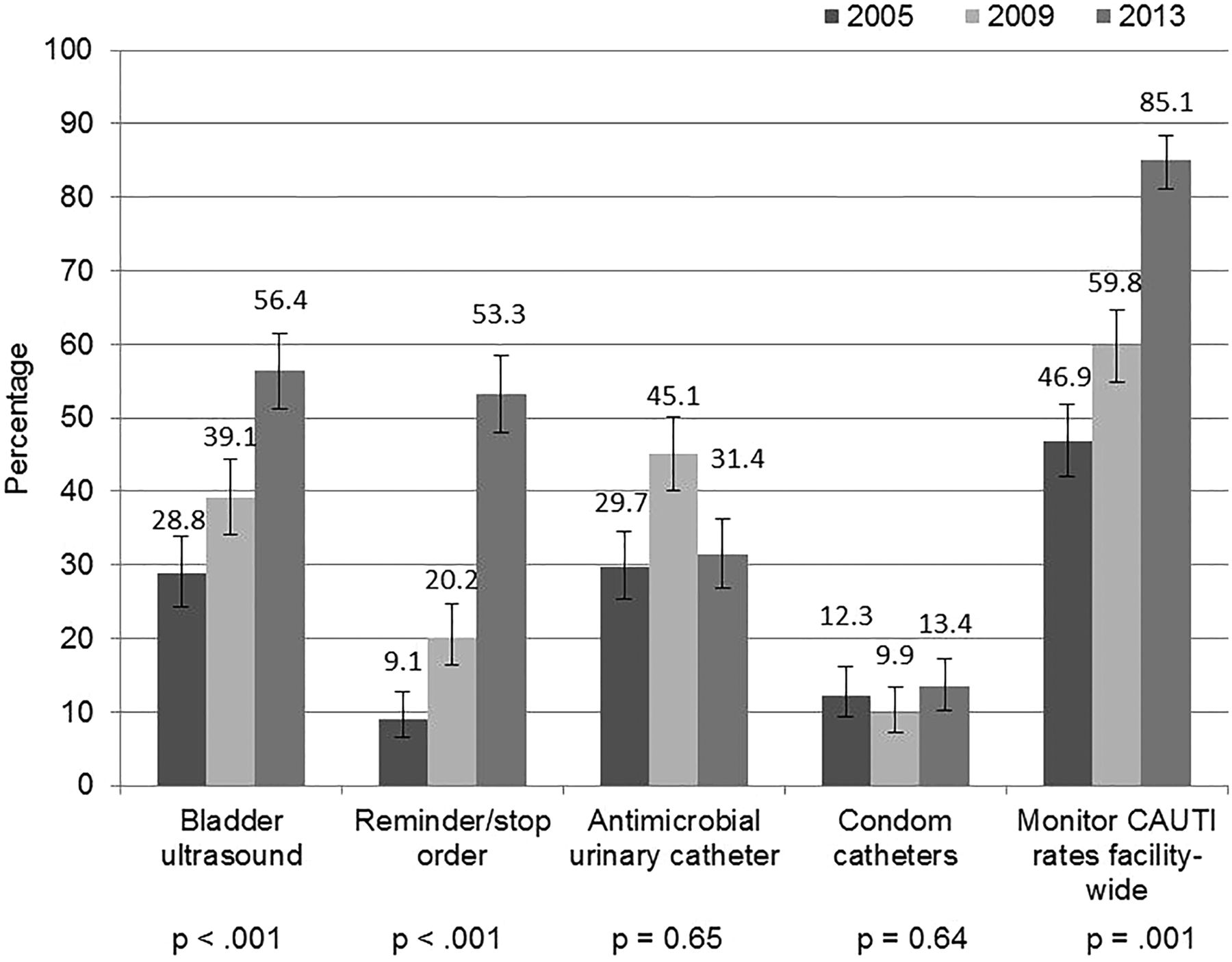
An increase in the use by hospitals of some CAUTI prevention practices also occurred during the study period (figure 3). Most notable is the increase in the per cent of hospitals reporting the use of urinary catheter reminders or stop-orders, which were used by 9% of hospitals in 2005, 20% in 2009 and 53% in 2013 (p<0.001). A significant increase was also observed in use of portable bladder ultrasound: 29% in 2005, 39% in 2009 and 56% in 2013 (p<0.001). Use of other practices remained relatively unchanged. While there was an increase in antimicrobial-coated urinary catheter use from 2005 to 2009 (30% to 45%), the per cent of hospitals using an antimicrobial device decreased to 31% in 2013. Another noteworthy change was the percentage of hospitals that reported having an established surveillance system for monitoring CAUTI rates facility-wide: 47% in 2005, 60% in 2009 and 85% in 2013 (p<0.001).
{kind=link}
{kind=link}
{kind=link}
Per cent of hospitals that regularly use practice to prevent Catheter-Associated Urinary Tract Infection (CAUTI).
Discussion
Providing safer care for patients by reducing HAIs—particularly those infections acquired during a hospital stay—has been a major focus of US policy-makers for at least a decade. This focus on safer care, led in part by the US government and reinforced by payment policies, mandated reporting of infection rates and targeted prevention efforts,11 ,14 ,17 ,30 ,31 appears to correspond with some observed reductions in rates of certain types of infections in many US hospitals.20 ,32 ,33 Our findings suggest one potential mechanism of action for the improved rates, showing that US hospitals have responded to the call to reduce infection by increasing their use of key recommended practices with nearly universal adoption of certain practices, such as maximum barrier precautions and chlorhexidine site disinfectant to prevent CLABSI, and semirecumbent positioning to prevent VAP. While our results also show some notable increases in the use of certain CAUTI prevention practices, CAUTI prevention in general continues to lag behind the prevention efforts targeting other device-associated infections.
Lower relative uptake of CAUTI prevention policies (compared with those for CLABSI and VAP) was also found in a survey of US hospitals by Stone et al.34 Moreover, our work has repeatedly shown generally low rates of use of CAUTI prevention practices by US hospitals,21 ,35 and that many clinicians do not view CAUTI as a priority, given it is usually less deadly than CLABSI or VAP and considered easily treatable with antibiotics.36 ,37 Despite these perceptions, over the past couple of years the importance of CAUTI prevention has become increasingly prominent as one of the targeted infections for non-payment, as part of the US government's national action plan and as one of The Joint Commission national patient safety goals for hospitals.38 Our findings suggest that these efforts—when looking at process measures—appear to be moderately successful, with an increase in the per cent of hospitals that are using important CAUTI prevention practices, such as reminders or stop orders and bladder ultrasound scanners, along with a significant increase in CAUTI surveillance efforts. Nonetheless even greater effort may be warranted. In particular, evidence shows that targeted initiatives that promote the use of key CAUTI prevention practices, whether at a facility level, a state level or even a national level, can lead to lower CAUTI rates.39–41 Preliminary results from the national ‘On the CUSP: STOP CAUTI’ initiative, for example, suggest up to a 16% relative reduction in CAUTI rates among participating hospital units.42 This compares with what appears to be little reduction or potentially even a slight increase in CAUTI rates in the USA based on data from the CDC.32 ,43 As such, in the US government's national action plan, which was updated and expanded in 2013, reducing the national rate of HAIs by 30 September 2015 by demonstrating a 10% reduction in hospital-acquired CAUTIs remains an agency priority.44
Preventing CLABSI has been perhaps one of the greatest success stories in the journey to reduce HAIs. Data from the CDC show a 44% decrease in CLABSI from 2008 to 201232 and, as noted in the HHS 2015 performance report, there was confidence that the target goal of a 50% reduction in CLABSI rates would be met.44 Our study shows almost universal adoption by US hospitals of maximum sterile barrier precautions and chlorhexidine as a site antiseptic during insertion of central lines, which likely contributes to this substantial reduction in CLABSI rates. Both of these practices are considered ‘basic practices that should be adopted by all acute care hospitals’ in recent guidelines, with a grade of 1 (high quality evidence) for chlorhexidine disinfectant and a grade of 2 (moderate quality evidence) for maximum sterile barrier precautions.25 Moreover, these practices were a standard part of the technical component (or CLABSI prevention bundle) that was used as part of the highly successful Veterans Affairs initiative45 and the Keystone ICU collaborative.46 ,47 Antimicrobial catheters, which according to current guidelines are classified under ‘special approaches for preventing CLABSI’ for use in locations or populations with unacceptably high CLABSI rates,25 remain consistently used by about a third of hospitals. In contrast, use of an antimicrobial dressing, also considered a special approach, has continued to increase with nearly 80% of hospitals reporting use of this practice in 2013. Continued monitoring of these trends are necessary to ensure the sustained use of critical practices for preventing CLABSI.
Data from the NHSN reveal rates of VAP that range from 0 to 4.4 across different types of hospital units.33 Lack of a valid or reliable definition of VAP, however, makes it difficult to assess progress with respect to preventing this highly morbid condition and has prompted the CDC to move to monitoring ventilator-associated events as part of the NHSN surveillance programme.26 Possible and probable VAP remains a component of the three-part ventilator-associated event definition and strategies for preventing VAP are still of critical importance. Our study suggests that the most commonly used strategy across US hospitals for VAP prevention is semirecumbent positioning, which entails elevating the head of the patient's bed 30° or more. However, use of an antimicrobial mouth rinse as part of oral care has also become increasingly popular, which may be due to several studies that show this to be an effective strategy for preventing postoperative respiratory infections especially in patients with cardiac surgery.26 ,48 Subglottic secretion drainage is also gaining traction with over 50% of US hospitals reporting use of this special type of endotracheal tube in 2013.
Results from comparable surveys conducted in Thailand and Japan include some findings that appear similar to those from our sample of US hospitals.9 ,49 In particular, reported use of catheter reminders or stop orders and bladder ultrasound scans to prevent CAUTI is relatively low, as compared with the use of maximum sterile barrier precautions to prevent CLABSI and semirecumbent positioning to prevent VAP, which are both used by at least 60% of hospitals in Thailand and Japan. On the other hand, reported use of chlorhexidine for insertion site antisepsis and antimicrobial dressings to prevent CLABSI as well as the use of antimicrobial mouth rinse and subglottic secretion drainage to prevent VAP appear to be substantially lower among hospitals in Thailand and Japan compared with our US sample. However, given the survey in Thailand was conducted in 2010 and the survey in Japan in 2012, and reflect only a single point in time, whether some of the difference is temporal in nature and the extent to which the use of such practices might be changing over time in these other countries is unknown. Ongoing work as part of the PROHIBIT study6 also includes data from a survey of hospitals throughout Europe but the results have not yet been published.
Our findings should be interpreted in the context of some possible limitations. First, non-response bias is a potential issue but given a nearly 70% response in all study years we believe these results accurately represent the use of infection prevention practices by US non-federal hospitals with 50 or more beds and an ICU in 2005, 2009 and 2013. However, we also recognise that the original sample as selected for the 2005 survey may no longer be as representative of the current distribution of US non-federal hospitals and that the sample selection and the sample weights may also require updating should this type of survey be repeated. Second, reported practice use is based on the response of one individual respondent from each hospital, generally the lead infection preventionist. This too could be a source of response bias. However, while the infection preventionist may not be intimately familiar with some of the more detailed aspects of practice implementation in a given unit, it is our experience through extensive qualitative studies36 ,37 that they are sufficiently aware of what types of approaches to prevent infection are being used in their hospital. Lastly, we do not have data on actual infection rates. Nonetheless, the practices included in the survey are practices that have been shown through research to reduce infections and are generally included in published guidelines or recommendations from the CDC and other professional associations. Moreover, we have previously shown how our findings correspond with national data on infection rates.41
US hospitals appear to be responding to the call to reduce infection by increasing their use of key recommended practices with nearly universal adoption of maximum barrier precautions, chlorhexidine site disinfectant and semirecumbent positioning. This increased use of prevention practices is likely a key reason for declining rates for some device-associated infections, such as CLABSI. While work to more fully understand hospital and external factors that facilitate effective implementation of key infection prevention practices is necessary to inform ongoing improvement efforts, persistent vigilance is also needed to ensure sustained improvement and additional strategies may be required, given an apparent lag in CAUTI prevention efforts.
Acknowledgments
The authors thank Andrew Hickner for his assistance with conducting the survey mailing, and Jason Mann for his help with manuscript preparation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors SLK had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: SLK and SS. Acquisition of Data: SLK, SS and KEF. Analysis and interpretation of data: SLK, SS, DR and JM. Critical revision of the manuscript for important intellectual content: SLK, SS, KEF and JM. Statistical analysis: DR. Administrative, technical or material support: KEF. Study supervision: SLK and SS.
-
Funding This project was supported by the Blue Cross Blue Shield of Michigan Foundation grant 1907.II and the US Department of Veterans Affairs (VA), including a VA National Center for Patient Safety funded Patient Safety Center of Inquiry. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs.
-
Competing interests None declared.
-
Ethics approval University of Michigan IRB and VA Ann Arbor Healthcare System Human Studies subcommittee.
-
Provenance and peer review Not commissioned; externally peer reviewed.