Article Text

Abstract
Objectives To define the target domains of culture-improvement interventions, to assess the impact of these interventions on surgical culture and to determine whether culture improvements lead to better patient outcomes and improved healthcare efficiency.
Background Healthcare systems are investing considerable resources in improving workplace culture. It remains unclear whether these interventions, when aimed at surgical care, are successful and whether they are associated with changes in patient outcomes.
Methods PubMed, Cochrane, Web of Science and Scopus databases were searched from January 1980 to January 2015. We included studies on interventions that aimed to improve surgical culture, defined as the interpersonal, social and organisational factors that affect the healthcare environment and patient care. The quality of studies was assessed using an adapted tool to focus the review on higher-quality studies. Due to study heterogeneity, findings were narratively reviewed.
Findings The 47 studies meeting inclusion criteria (4 randomised trials and 10 moderate-quality observational studies) reported on interventions that targeted three domains of culture: teamwork (n=28), communication (n=26) and safety climate (n=19); several targeted more than one domain. All moderate-quality studies showed improvements in at least one of these domains. Two studies also demonstrated improvements in patient outcomes, such as reduced postoperative complications and even reduced postoperative mortality (absolute risk reduction 1.7%). Two studies reported improvements in healthcare efficiency, including fewer operating room delays. These findings were supported by similar results from low-quality studies.
Conclusions The literature provides promising evidence for various strategies to improve surgical culture, although these approaches differ in terms of the interventions employed as well as the techniques used to measure culture. Nevertheless, culture improvement appears to be associated with other positive effects, including better patient outcomes and enhanced healthcare efficiency.
Trial registration number CRD42013005987.
- Healthcare quality improvement
- Communication
- Human factors
- Management
- Safety culture
Statistics from Altmetric.com
Introduction
Healthcare organisations are employing interventions that aim to improve local culture as a way to create a more positive and patient-friendly clinical environment. Many successful quality improvement projects, such as the statewide reduction in catheter-related bloodstream infections in Michigan1 and the reduced morbidity and mortality associated with the WHO Surgical Safety Checklist,2 included efforts to improve the culture surrounding healthcare delivery. In fact, leaders of these projects often attribute improvements in care as much to the changes in local organisational culture as to components of the intervention itself.3 It appears, therefore, that combining quality improvement with efforts to promote workplace culture has the potential to improve both the quality and efficiency of healthcare delivery.
In To Err Is Human, the Institute of Medicine (IOM) highlights the importance of building a culture of safety as a prerequisite to improving healthcare quality and reducing patient harm.4 In this context, culture refers to the beliefs, values and behavioural norms shared between individuals in a team or unit. These issues are particularly salient in fields like surgery, where procedures are dynamic, complex, high-stakes and rely on contributions from team members across multiple disciplines.5
Since the IOM report, many organisations have attempted to measure, understand and even improve their local culture. Within surgery, culture often varies by provider type and physician specialty, even within the same institution.6 ,7 While the threshold for positive culture depends heavily on the method of assessment, better culture, as it pertains to patient safety, appears to correlate with fewer adverse intraoperative and postoperative events.8–10 What remains unclear, however, is whether culture change is truly feasible and whether improving culture leads to better patient outcomes. Further, the optimal strategies for improving surgical culture remain uncertain. To better characterise these issues, we performed a systematic review with the following aims: (1) to identify the most common domains of culture improvement interventions, (2) to assess the effectiveness of these interventions at improving surgical culture and (3) to determine whether culture improvement is associated with better patient outcomes and more efficient healthcare delivery.
Methods
Review registration
This systematic review was registered with PROSPERO (University of York, Centers for Reviews and Dissemination), an international database of prospectively registered systematic reviews (registration number CRD42013005987). The methodology and reporting were performed in line with the Preferred Reporting Items for Systematic review and Meta-Analyses.11
Search strategy
Our search strategy, developed with the assistance of a research librarian, began with a comprehensive definition of surgical culture: the interpersonal, social and organisational factors that affect the healthcare environment and influence patient care in the perioperative period. We searched PubMed, Cochrane, Web of Science and Scopus databases from January 1980 to January 2015 for interventions directed at improving any aspect of surgical culture. Our final search protocol included the Medical Subject Headings (MeSH) terms Organizational Culture, Social Environment, Interprofessional Relations, Attitude of Health Personnel, Surgery Department, Hospital, Operating Rooms, Surgical Procedures and Operative/standards as well as important keywords, such as teamwork, communication and safety climate (see online supplementary appendix 1). References of included studies were also screened for additional studies relevant to our topic.
Review and study inclusion and exclusion
We screened for studies relevant to surgery, including labour and delivery and other surgical subspecialties. Based on our initial title and abstract screening, we determined that studies employed culture-improvement strategies that fit within discrete domains. In order to better describe the improvement strategies, the authors identified these domains empirically and revised them in an iterative process as our search progressed. Full-length studies were then screened and included in our review if they met the following inclusion criteria: the study reported on an intervention that aimed to improve surgical culture and culture change was measured directly. We excluded editorials, reviews and titles with no available abstracts. Studies were screened sequentially based on title, abstract and full studies as generated by our search; two investigators independently performed each stage of screening.
Data collection
Data were abstracted using a structured abstraction tool. We collected data on the year of publication, domain and type of culture-improvement intervention used, study design, characteristics of study participants, healthcare setting, surgical specialty, country, medical centre type, culture assessment tool used, study time frame and any potential obstacles to culture change that were highlighted. When applicable, we also abstracted data on related outcomes, which we divided into two categories: patient outcomes (eg, morbidity or mortality) and healthcare efficiency (eg, operating room (OR) turnover time, equipment availability issues, handoff problems).
Quality assessment
The primary goal of our quality assessment was to assess the reliability of the study design and the generalisability of the findings. We therefore adapted a quality assessment tool used in prior reviews that evaluated interventions in which the results are sensitive to the context and implementation of the programme.12 ,13 Strong study designs included the use of a control group and/or repeated outcome measurements to assess the sustainability of culture change. Studies were determined to be generalisable if they reported on an intervention that was either implemented or measured in actual clinical settings as opposed to simulation-based exercises. In addition to design and generalisability, better quality studies met the following three criteria: intervention performed at multiple sites (separate hospitals, clinics or health centres), use of an established theory as a basis for the intervention and mandatory participation for all staff members (which we assumed to be more representative of real-world interventions than those requiring voluntary participation). In order to focus our review on studies of higher quality, studies were categorised as high quality if they met all criteria, moderate quality if they met four criteria and low quality if they met fewer than four criteria. Two investigators independently performed quality assessment. To supplement this quality assessment tool, we also assessed randomised trials using the Cochrane Collaboration's Tool for Assessing Risk of Bias.14
Results
Description of the studies
Our search yielded 47 studies that met our inclusion criteria (figure 1). Twenty-five studies were performed in the USA, while the remaining studies were performed in the UK (n=13), Canada (n=4) or other international settings (n=5). Most studies were performed in academic medical centres; four took place at a Veterans Affairs Hospital.15–18 Overall, the vast majority of studies involved interventions targeting the intraoperative or perioperative period (n=38). Fewer studies targeted postoperative (n=7)18–24 or preoperative care (n=6); however, several studies targeted more than one setting.22 ,25–29
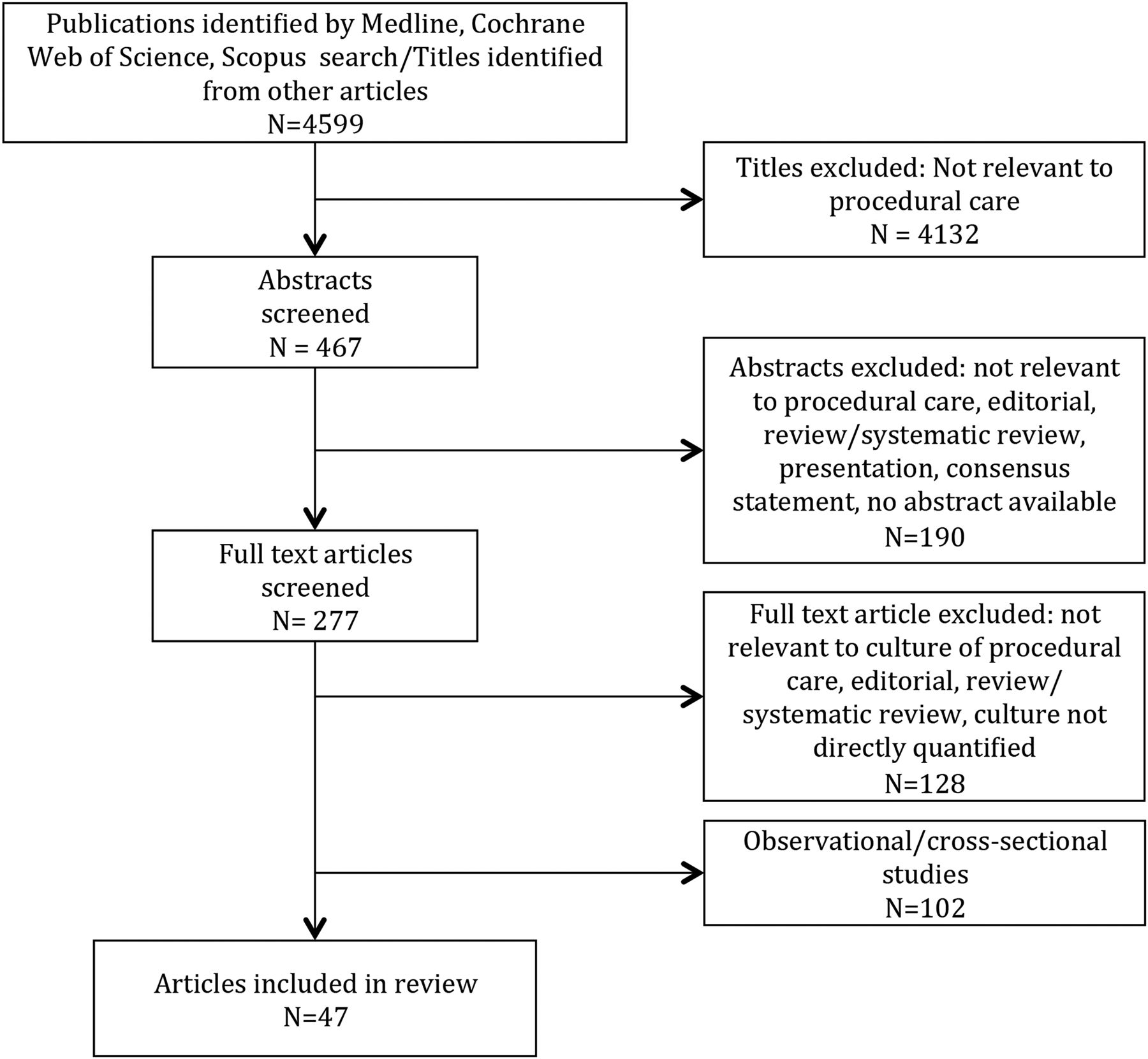
{kind=link}
Identification of eligible studies.
Studies mostly included interventions that targeted surgeons and nurses (n=43). Twenty studies focused specifically on surgery or anaesthesia residents and three studies studied culture improvement among medical students.17 ,20–24 ,27 ,28 ,30–42
Quality assessment
Of the 47 studies included in our review, 4 were randomised control trials (RCTs), of which 3 had low risk of bias and 1 had unclear risk of bias (see online supplementary appendix 2). However, all four of these studies evaluated an intervention that took place in a simulated environment, greatly limiting their relevance and generalisability to real-world clinical settings. These studies were therefore categorised as low quality by our quality assessment tool.23 ,24 ,31 ,43 Of the 43 observational studies, 10 (23.3%) were determined to be moderate-quality and 33 (76.7%) to be low quality (see online supplementary appendix 3); none met criteria for high quality. Five studies used a controlled pre-post study design without randomisation,21 ,27 ,29 ,44 ,45 two of which were deemed moderate quality. The remaining studies used pre-post study design without a control group. The moderate-quality and low-quality studies are summarised in Table 1 and online supplementary appendix 4, respectively.
Summary of moderate-quality studies evaluating effects of cultural interventions
Cultural definition and measurement
The most common tool for culture measurement, used by over half of the moderate-quality studies (n=6),15–17 ,22 ,38 ,46 was the Safety Attitudes Questionnaire (SAQ). The SAQ is a validated and widely adopted tool used to measure work environment and patient safety culture.47 The second most frequently used tool across all studies was the Oxford Non-technical Skills scale.23 ,24 ,29 ,32 ,44 ,48
Interventions employed
Culture-improvement strategies varied between studies but fit discretely into three separate domains: teamwork (n=28), communication (n=26) and safety climate (n=19); several studies fit into more than one domain. Studies were included in a given domain if the authors directly expressed the goals of improving that domain of culture. Moderate-quality studies were represented equally in all three domains (safety climate,15 ,19 ,21 ,22 ,38 teamwork16 ,19 ,21 ,22 ,45 ,46 and communication17 ,19–21).
Interventions were grouped into several categories, including briefings/debriefings (n=23), team-building exercises (n=22), educational campaigns (n=21) and checklists (n=15). Often, more than one type of intervention was employed. On occasion a single intervention was directed at multiple domains of culture. For example, checklists were used to improve communication but were also used to improve teamwork and safety climate.34 ,49
Briefings and debriefings typically refer to a brief, 5 min assembly of the surgical team before and after the operation to discuss specific details of the case. Educational campaigns varied from voluntary review of guidelines followed by a knowledge test38 to a human factors seminar lasting two full days.50 Checklist interventions aimed to improve culture by standardising processes, streamlining care pathways and empowering team members to speak up when care deviated from expected. Checklists were either implemented as an isolated intervention or as a component of a more comprehensive intervention bundle (eg, medical team training (MTT), central line insertion bundles). In some cases, checklists used the WHO Surgical Safety Checklist without any content modification.21 ,34 ,41 ,49 ,51
Educational campaigns and team-building exercises were either developed by investigators or they were adapted from previously validated programmes, most notably Team Strategies to Enhance Performance and Patient Safety (TeamSTEPPS)19 ,25 ,28 ,40 ,45 and MTT.15–18 ,30
Improvements in culture
All moderate-quality studies (n=10) reported an improvement in at least one domain of culture (all low-quality studies, with the exception of Morgan et al,44 also reported culture improvements). For example, Weaver et al demonstrated a significant improvement in communication in the OR as measured by an increased number of check-backs, call-outs and handoffs after implementation of the TeamSTEPPS programme in comparison to a control arm (p<0.05). This study also demonstrated a significant improvement in communication as measured by the Hospital Survey on Patient Safety Culture and Operating Room Management Attitudes Questionnaire (p<0.05).45 A study by Wolf et al measured job satisfaction using SAQ after implementation of MTT and found a significant improvement in perceptions of management (p=0.003) and working conditions (p=0.004). There was also a significant drop in nurse turnover during the study period, a marker for nurse job satisfaction.17
While improvement in one domain of culture was nearly ubiquitous, 30 of the 47 studies also reported no improvement in one or more of the other measured domains. For example, Bleakley et al46 noted a significant improvement in teamwork after an educational intervention (p=0.034) but failed to observe significant changes in other domains, including job satisfaction, perception of management, working conditions and safety climate. In some cases, an intervention led to improvements among one group of providers but not others. For example, in a study by Carney et al that implemented MTT, surgeons reported a significant improvement (p<0.05) in all six teamwork items of the SAQ. However, there was no change in nurses' response to ‘nurse input is well received’ after the intervention.16 Similar, partial improvement in culture was reported in 13 other studies.15–17 ,22 ,27 ,30 ,32 ,34 ,37 ,41 ,46 ,49 ,50 Of note, two of the four RCTs also reported no improvement in at least one domain of culture.31 ,43
Evidence of sustained improvements in culture
Several studies continued to track the effects of the intervention long after the intervention was implemented. In a few cases, the positive findings were sustained for >1 year (n=4).22 ,38 ,46 ,52 The median follow-up time for all studies was 9 months.
Patient outcome measures
Two moderate-quality studies made an attempt to connect improved culture to better patient outcomes.19 ,38 Both reported a decrease in postoperative complications. Pettker et al38 reported a significant reduction in the Adverse Outcomes Index (a score reporting on the number of neonatal deliveries with at least 1 of 10 adverse outcomes per total deliveries) over 3 years after implementing a multifactorial patient safety intervention (R2=0.50; p=0.01). Armour Forse et al19 demonstrated a reduction in mortality from 2.7% to 1% (p<0.05) after implementing the TeamSTEPPS programme, and also reported a reduction in overall surgical morbidity (20.2% to 11.0%, p<0.05) as well as an increase in appropriate antibiotic administration, deep vein thrombosis prophylaxis and beta-blocker administration. This study, however, did not perform risk adjustment or include a control group. Additionally, many of the findings in this study, including reduced morbidity and mortality, were not sustained at 1-year follow-up. Evidence regarding better patient outcomes following interventions to improve surgical culture was also provided by several low-quality studies.24–26 ,30 ,34 ,42 ,48 ,49 ,53 ,54
Efficiency measures
Two moderate-quality studies also measured improvements in efficiency after an intervention to improve surgical culture.17 ,19 Armour Forse et al19 reported improved OR punctuality following implementation of TeamSTEPPS (81% cases starting on time postintervention vs 69% preintervention) while Wolf et al17 noted a reduction in OR delays (23% to 10%, p<0.0001), a decrease in equipment availability problems (24% to 7%, p<0.0001) and fewer patient handoff issues (5.4% to 0.3%, p<0.0001) after MTT. These findings were supported by three low-quality studies.28 ,55 ,56
Obstacles to culture improvements
The two major obstacles to culture improvements identified were participant reluctance to engage in activities and the regression of improvements over time.19 ,35 ,56 ,57 One study by Bethune et al56 noted “it was rarely possible to get all members of the staff together for a formal debrief”. Additionally, Khoshbin et al35 reported that surgeons were concerned that mandating intervention compliance may result in completion of the required task without consideration of the underlying importance of the intervention, thereby reducing the intervention's observed effects.
Two studies reported regression towards baseline in some of the improvement initially noted in early follow-up measurements. Armour Forse et al19 noticed an increase in surgical mortality and morbidity towards, but not reaching preintervention measures, 1 year after implementation of TeamSTEPPS, and Böhmer et al57 reported that improvement in communication was not maintained at 18 or 24 months after implementation of the WHO Surgical Safety Checklist.
Discussion
Our systematic review identified 10 moderate-quality studies, all of which demonstrated an improvement in at least one domain of culture. Several of these studies also showed marked improvements in patient outcomes and healthcare efficiency, findings that were further supported by a number of low-quality studies. Our findings offer promising evidence that not only is it possible to improve surgical culture but that interventions aimed at improving culture may be viable targets for the future of quality improvement.
Unlike clinical trials, which tend to use standardised protocols and targeted outcomes, we identified a wide range of successful culture interventions. While briefings/debriefings and team-building exercises were common components of successful interventions, individual programmes varied widely across studies and many combined multiple components into a single intervention plan. Because of this, we were unable to determine which specific types of interventions were most successful at improving culture. However, our finding that measureable changes in culture can result from multiple, seemingly unrelated interventions suggests that the formula for success is likely to be more site-specific than intervention-specific. Multiple examples that similar interventions do not necessarily lead to similar outcomes exist in the quality improvement literature, including a recent study evaluating the mandated implementation of the WHO Safe Surgery Checklist in Ontario, Canada. Despite previous work suggesting that checklists lead to better patient outcomes,58 Urbach and colleagues failed to demonstrate any improvement in the first three months after the policy was implemented.59 As any given intervention—even an effective and validated one—is unlikely to be successful in every clinical setting, healthcare institutions intent on improving their surgical culture may benefit more from developing individualised programmes based on proven domains (teamwork, communication and safety culture) than from implementing a standardised, ‘off-the-shelf’ intervention in their local environment.
Similar evidence from other specialties, particularly critical care medicine, appears to support the idea that improving institutional culture can result in better patient outcomes.1 ,60 The most successful of these strategies has been the Comprehensive Unit-based Safety Program (CUSP), which harnesses the energy and expertise of frontline providers and aligns them with the resources of hospital leadership. According to the CUSP model, efforts to engage and motivate frontline providers are made front and centre in order to promote workplace culture that prioritises patient safety and celebrates high-quality care delivery. As a result, a synergistic relationship emerges: delivering high-quality care reinforces positive culture, which in turn reinforces high-quality care. While the implementation of CUSP in the field of surgery has been limited,61 many successful strategies highlighted in this review, including TeamSTEPPS and MTT, include basic CUSP principles.62 ,63 Rather than ‘top-down,’ institution-wide quality programmes, future interventions in surgery may benefit from embracing a more ‘bottom-up’ approach.
While interventions to improve culture in non-surgical settings may inform similar efforts in surgical settings, the OR itself presents unique challenges to measuring and improving institutional culture. Multiple groups of providers (surgeons, anaesthesiologists, nurses)—each with its own training and group philosophy—may limit effective team building. Hierarchy (attending surgeons and trainees, surgeons and non-surgeons) may restrain communication, and tradition may preclude efforts to promote a safety-oriented climate. Given these challenges, efforts to improve surgical culture must adopt a multimodal approach—one that takes into account all relevant team members and stakeholders, and capitalises on the authority of institutional leadership. One promising development in this direction is the American College of Surgeons National Surgical Quality Improvement Program Quality In-Training Initiative, a programme designed to facilitate accountability for patient outcomes and foster an interest in quality improvement among surgical residents.64 As many of these trainees will go on to establish the standards for their future practice settings, training residents to recognise the importance of culture is essential to producing lasting changes in surgical practice.
Despite a general belief that culture change is exceedingly difficult,65 almost all included studies found improvements in at least one measured domain of culture. Alternative explanations for these observed improvements may highlight potential limitations to our review. One possibility is the Hawthorne effect: a phenomenon in which improvements occur as a result of observation and measurement rather than actual changes in practice.66 Culture may be particularly susceptible to these effects due to its loose definition and imprecise measurement tools. Similarly, improvements in culture, outcomes and efficiency may simply be an artefact of other structural changes to patient care rather than a result of studied interventions. Another possible explanation is publication bias, namely that unsuccessful attempts to improve culture are either not written up or not accepted for publication in peer-reviewed journals.67 Our findings are also limited by the precision of our search strategy. Due to its complex definition, culture may have been imperfectly captured by our search terms, resulting in the inadvertent exclusion of relevant studies.
Finally, although all studies demonstrated improvement in at least one culture domain, many also found areas where culture or outcomes did not improve. Those domains that were targeted specifically appeared to improve universally (ie, interventions to improve communication do in fact improve communication); however, there was inconsistent improvement for non-targeted domains and non-targeted clinical sites. In fact, one study actually found lower communication and teamwork ratings for the postacute care unit after performing an intervention on OR personnel.19 These findings reiterate the importance of establishing multiple measurable targets, electing hospital-based and unit-based programme leaders, and applying sustained pressure through simultaneous and complementary interventions.68 Considering the lack of longitudinal data, further research is also needed to determine the fidelity of interventions across healthcare settings and the impact that intermittent, repeated interventions may have on the sustainability of culture change.
Conclusion
Surgical culture appears amenable to a wide range of interventions to improve teamwork, communication and safety climate. Improvements in culture also facilitate progress in other domains of healthcare, including patient outcomes and care efficiency. Future work should aim to standardise methods of culture measurement and reporting.
Acknowledgments
We acknowledge Paul Shekelle, MD, MPH, PhD, West Los Angeles Veterans Affairs Medical Center, Los Angeles, California, for providing helpful guidance on study methodology and manuscript writing, and Bethany Myers for assisting with our search strategy.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online appendix 1
- Data supplement 2 - Online appendix 2
- Data supplement 3 - Online appendix 3
- Data supplement 4 - Online appendix 4
Footnotes
Twitter Follow Greg Sacks at @gregDsacks
Contributors All authors have contributed sufficiently to the study to warrant authorship.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement We are willing to share any additional details of our search strategy and results not already included in the manuscript.