Article Text

Abstract
Background Healthcare has become increasingly complex and care delivery models have changed dramatically (eg, team-based care, duty-hour restrictions). However, approaches to critical communications among providers have not evolved to meet these new challenges. Evidence from safety culture surveys, academic studies and malpractice claims suggests that healthcare handover quality is problematic, leading to preventable errors and adverse outcomes. To address this concern, from 2013 to 2016 Massachusetts General Hospital completed phase I of a multifaceted programme to implement standardised, structured handovers across all departments, units and direct care providers.
Methods A multidisciplinary Handovers Committee selected the I-PASS handover system. Phase I implementation focused on large-scale training and shift-to-shift handovers. Important features included administrative and clinical leadership support; EHR templates for I-PASS; hospital handover policy revision; varied educational modalities, venues and durations; concomitant TeamSTEPPS training; unit-level I-PASS champions; handover observations; and solicitation of caregiver feedback and suggestions.
Results More than 6000 doctors, nurses and therapists have been trained. Trended observation scores demonstrate progressive but non-uniform adoption of I-PASS, with significant improvements in the correct sequencing and percentage of I-PASS elements included in handovers. Adoption of Synthesis (readback) has been challenging, with lower scores.
Conclusions Comprehensive I-PASS implementation in a large academic medical centre necessitated major cultural change. I-PASS education is straightforward, whereas assuring consistent and sustained adoption across all services is more challenging, requiring adaptation of the basic I-PASS structure to local needs and workflows. EHR I-PASS templates facilitated caregiver acceptance. Initial phase I results are encouraging and the lessons learned should be helpful to other programmes planning handover initiatives. Phase II is ongoing, focusing on more uniform and consistent adoption, spread and sustainability.
- Communication
- Hand-off
- Human factors
- Patient safety
- Transitions in care
Statistics from Altmetric.com
Introduction
Problem description
In 2012, Massachusetts General Hospital (MGH) safety culture survey scores for handovers and transitions of care, though similar to the national median, were the lowest among all domains. Furthermore, based on safety reports and resident surveys, deficient handovers were not infrequently associated with preventable errors and adverse events. Although virtually all departments and divisions had some handover policy, there was no systematic, standardised, institution-wide approach.
These findings were also concerning given the educational mission of MGH, as there are Accreditation Council for Graduate Medical Education (ACGME) Common Program Requirements (VI.B.2 and VI.B.3) for resident competency in ‘effective, structured handover processes’.1 A previous study of MGH residents demonstrated that handovers often lacked important elements, and 59.4% of respondents reported that problematic handovers had contributed to major or minor patient harm.2
These considerations were the proximate stimulus for the MGH Center for Quality and Safety (CQS) to implement a comprehensive handover initiative using the I-PASS system.3–5
Available knowledge
The handover problem
Handovers of patient care responsibility are ubiquitous in healthcare, affecting all practitioners in a myriad of different scenarios: nurses, residents, attending physicians and therapists; shift change, weekend coverage, night floats, off-service transitions, cross-service or cross-venue transfers; and inpatient–outpatient transitions.6 ,7 However, despite their central role in assuring safe and high-quality care, evidence from multiple sources demonstrates that healthcare handovers are often flawed or inadequate. Handoffs and transitions of care are typically among the lowest scoring domains in national summaries of Agency for Healthcare Research and Quality (AHRQ) safety culture survey scores (47% positive in 2014),8 and communication failures are a common cause of Joint Commission Sentinel Events9 and malpractice claims.10–12
Handovers have not evolved to meet the needs of contemporary practice
Healthcare handovers have always been suboptimal. However, their inadequacy has become more apparent and consequential in recent years, and the attention focused on them has commensurately increased,13–15 because they have not evolved to meet the new paradigms and challenges of modern healthcare.
Medicine and surgery have become increasingly complex—more diagnoses and treatments, more practitioners involved in a patient's care, team-based care and new care delivery venues. A decade ago, estimates suggested that an average patient hospitalisation was associated with 24 physician and nurse handovers and the number is undoubtedly larger now,13 ,14 providing even more opportunities for error.16
The highly variable, inconsistently effective practice of healthcare handovers stands in stark contrast to the systematic teaching, implementation and monitoring of communication strategies that characterises truly high reliability professions such as aviation, space exploration (National Aeronautics and Space Administration), nuclear power, railroad and ambulance dispatch and Formula One racing.7 ,17–20 Health policy, regulatory and accreditation organisations all now recognise the need to improve and standardise healthcare handovers to achieve comparable levels of reliability.1 ,21 ,22
Handovers at teaching hospitals
Teaching hospitals are particularly vulnerable to handover-related adverse events and patient harm because of their complex case mix, size, frequent resident handovers and constantly changing trainee rotations.2 ,23–28 Resident duty-hour restrictions have further exacerbated the handover problem, as cross coverage and night floats are increasingly used. Residents are often less knowledgeable about their patients; there are more delays, in-hospital complications and preventable adverse events; continuity of care has decreased; and the overall quality of medical and surgical care is potentially compromised.29–37
Lack of systematic handover education
Despite the availability of various handover educational strategies,38 ,39 most medical students and residents still receive little or no formal education in structured, standardised handover and communication techniques, nor are there widely accepted standards or expectations.19 ,26 ,38–45 Handover techniques are typically learned by apprenticeship and imitation of local practice and vary substantially by unit and service.
Assuring care continuity in the new paradigm
Clearly, the optimal balance of trainee fatigue mitigation, continuity of care and patient safety has not yet been achieved, and better handovers are critically needed. In the new paradigm, optimal team communications and continuity of care will assume greater importance as individual practitioner continuity diminishes.27 ,46
Rationale for the I-PASS system
I-PASS contains all optimal handover features
Considerable research, including studies from consistently high-reliability industries and professions, has identified features that characterise optimal handover practice (table 1, left column).6 ,7 ,12 ,14–16 ,19 ,21 ,26–28 ,47–50
Optimal handover features and corresponding MGH implementation tactics
I-PASS handovers incorporate all the optimal handover features in table 1, and this system has been rigorously studied, validated and published in the peer-reviewed literature.3–5 ,52 We found I-PASS to be simple and intuitive; it was specifically designed for healthcare and can accommodate numerous complex patients and problems; and robust educational resources are available, including relevant aspects of TeamSTEPPS.
The first three I-PASS elements are familiar to most clinicians—illness severity (how sick is the patient), patient summary (events leading up to the hospitalisation; diagnostic work up; hospital course; treatments; overall plan) and action list (what needs to be accomplished by the handover receiver; time frame; consultations and test results; indication of completion).
I-PASS also incorporates two elements which are not as familiar to clinicians and much less consistently used in current handover practice —situational awareness/contingency planning and synthesis by receiver. The former emphasises situations that might arise given a patient's hospital course or disease process, and the suggested actions or treatments. This is anticipatory problem solving, similar to an emergency checklist for airline pilots, which makes the incoming provider better prepared for all eventualities.
Synthesis by receiver, a communication standard in most other high-reliability professions, is the concise checkback or readback of the information which has been conveyed, followed by an opportunity for bidirectional, interactive discussion and questions between handover giver and receiver (rather than one-way, telegraphic communication). This assures accurate and complete information transfer and enhances understanding of the patient.53–55
Systematic curricular development
Among handover systems we evaluated, a uniquely desirable feature of I-PASS was its systematic, formal curricular development,4 including detailed conceptual and logic models.
Evidence-based practice
Results of a pilot study using an I-PASS precursor, and a subsequent multicentre I-PASS study, have shown dramatic reductions in errors and adverse events,5 ,52 which greatly facilitates provider acceptance.
Compatibility with MGH culture and organisational needs
Core attributes of the I-PASS system are fully consistent with MGH organisational culture and context,56 including evidence-based practice and a commitment to quality and safety, and only a manageable number of new skills and organisational changes were required.
Understanding and mitigating potential implementation barriers
Even evidence-based programmes that have been successful in pilot studies may not achieve similar results when more broadly applied in real-life healthcare settings.57 This may reflect failure to understand and address theoretical and contextual barriers to implementation.56 ,58 ,59
The MGH I-PASS initiative illustrated potential challenges that were similar to those described by Grol and Grimshaw56 in the context of a hand hygiene programme. These included lack of practitioner understanding of the impact of non-compliance on patient outcomes, and resulting unwarranted comfort with current approaches (cognitive theory); lack of external stimuli for change, such as feedback on current performance, incentives and modelling of new practices (behavioural theory); lack of social or group norms, opinion leaders or local consensus (eg, senior residents and attendings were generally satisfied with existing practices and reluctant to change (social influence theories)); lack of existing institutional policy promoting the expected behaviour (organisational theory); and the need for clear, appealing messages about the importance of the initiative (marketing theory).
Finally, a number of practical organisational factors also posed potential barriers to successful I-PASS implementation. These include patient coverage and workload concerns (eg, perceived insufficient time to do an I-PASS handover on each patient); and challenging current workflows on some services, such as asynchronous handovers using secure email, which is contrary to the I-PASS emphasis on in-person, synchronous, interactive dialogue. Understanding these theoretical, practical and contextual barriers to compliance assisted us in designing customised intervention approaches.
Specific aim
The project aim was to implement I-PASS across all MGH disciplines, venues and caregivers, thereby improving handover communications and ultimately reducing medical errors and adverse events.
Methods
Context
Hospital statistics
MGH is a 999 bed tertiary/quaternary academic medical centre located in Boston, Massachusetts. It serves local patients from metropolitan Boston and adjacent suburbs and is a national and international referral centre for complex or critically ill patients. MGH has approximately 51 000 annual admissions, 106 000 emergency department visits, 21 000 inpatient surgical operations and 16 000 outpatient surgical procedures. The Massachusetts General Physicians Organization (MGPO) is a multispecialty group practice employing roughly 2500 physicians. MGH has approximately 880 residents and interns, 4800 registered nurses and nearly 25 000 full or part-time personnel.
Complex case mix and teaching mission
MGH's often complex patient population requires the involvement of many different providers and services, and accurate information exchange among them is critical. As a major teaching institution, residents are involved in the care of most patients, and they constantly convey important end of shift and end of rotation information.
Senior leadership support and the Lawrence CQS
MGH and MGPO Board of Trustees and senior leadership are committed to quality and patient safety; in 2007, they established the Lawrence CQS to accelerate progress in these areas. CQS coordinates all quality and safety activities within the institution, aided by a network of departmental and Patient Care Services (Nursing) quality chairs, and it was well positioned to direct I-PASS implementation. This initiative was led by three CQS staff as part of their institutional responsibilities. Except for initial startup costs, ongoing costs of education and programme management consisted mainly of staff time and were considered part of the Center's annual goals.
Interventions
The right column of table 1 summarises MGH implementation approaches, which reflect the optimal handover principles in the left column6 ,7 ,12 ,14–16 ,19–21 ,26–28 ,38 ,40 ,47–50 ,60–64 and the contextual features described previously. Important components include the following.
MGH Handovers Committee
In 2013, MGH formed a multidisciplinary Handovers Committee consisting of representatives from CQS, physician and nurse leaders from across the institution, therapists, educators and trainees. This committee evaluated various handover systems and selected I-PASS. It subsequently provided high-level strategic direction and served as the link to other stakeholder groups.
Senior leadership advocacy
The support of senior hospital leadership, board members, department chairs and senior physicians and nurses was critical to effect major behavioural and cultural changes.65 Considerable effort was devoted to educating these groups and assuring their engagement in I-PASS implementation. The Hospital President communicated his support for I-PASS in global emails, and I-PASS leaders presented to the MGH Board of Trustees and department chairs. Physician education was usually conducted by a Hospital Vice President, which sends an important message regarding institutional commitment.
Universal training
In contrast to the more limited approach in some previous I-PASS publications, we trained all direct caregivers (eg, attending physicians and residents, nurses, therapists), with education tailored to specific role groups, venues and specialties. This broader scope of implementation demonstrated that I-PASS was an institutional priority, and it also facilitated use of I-PASS in communications across role groups and settings.
Housestaff Quality and Safety Committee
Most physician handovers occur among residents. As a source of frontline feedback regarding implementation barriers and suggested changes, the Housestaff Quality and Safety Committee provided valuable input and leadership, facilitating iterative improvements in implementation strategies and tactics.
Timeline
Ideally, all caregivers would be educated simultaneously, and implementation would progress in parallel across the institution. However, the realities of clinical care, hospital operations, fiscal constraints and competing priorities made this impossible at MGH, as it likely would be at many other hospitals. For example, it was necessary to train nearly 4000 nurses without taking them offline (which would have required expensive backfilling), and staggered training was necessary. Also, during phase I of I-PASS implementation (2013–2016), MGH had numerous other major competing priorities including Joint Commission preparation, Ebola planning and installation of a new Electronic health record (EHR). Phase II (adoption, spread and sustainability) is expected to take several more years.
Communicating the evidence base
When MGH began its I-PASS initiative, most clinicians were satisfied with their current handovers and unenthusiastic about changing their practices without a compelling motivation. Thus, our I-PASS training programmes emphasised the empirical evidence linking structured, standardised handovers and higher quality patient care. All I-PASS training presentations began with a review of the evidence supporting the urgent need to improve patient handovers; the anticipated improvements in patient safety that would likely result; and the demonstrated effectiveness of I-PASS in peer-reviewed publications.
Varied, flexible training opportunities
Training sessions varied from brief I-PASS introductions (20–30 min) to 1.5–2 hours, full training sessions. Presentations were developed for all potential training opportunities, and they were offered at a variety of times to accommodate different schedules. These included 25 open training sessions with handover simulations (631 individuals trained); presentations to 20 individual departments or units, either at Grand Rounds or departmental meetings (1091 individuals trained); and orientation sessions for new house officers in June. In order to train 4000 nurses without disrupting their patient care responsibilities, a comprehensive, multimodality educational initiative was developed and implemented by the MGH Knight Center for Clinical and Professional Development.
All these training opportunities were also made available on an ongoing basis for new trainees, attending staff, nurses, therapists and other staff involved in direct patient care.
Multimodal educational techniques
A variety of adult learning modalities were either created internally or adapted from the I-PASS developers (http://ipassstudygroup.com/), including didactic lectures, web modules, teaching manuals, slide presentations, videos, workshops, simulations, role playing and an introduction to TeamSTEPPS. I-PASS handovers were imbedded within a number of scenarios in the MGH Simulation Unit. We also implemented periodic hospital-wide public relation campaigns including hospital newsletters and emails, posters featuring hospital leaders, badge cards and buttons.
MGH handover policy revision
The hospital's policy on handovers and transitions of care was due for its periodic revision as I-PASS was being introduced. At the request of the Handover Committee, this policy was amended to explicitly recommend (but not mandate) the use of I-PASS.
Appropriate sequencing
I-PASS implementation began with shift-to-shift handovers, as these are the most frequent and universal. Individual services and units were encouraged to adapt the basic I-PASS structure to their particular workflows, which were mapped, and numerous templates and unit-specific demonstration projects were developed. During phase II, currently underway, cross-departmental and cross-venue handovers will be implemented.
EHR handover templates
I-PASS implementation overlapped with introduction of a new EHR into the hospital. We included members of our EHR and IT leadership in the Handover Committee, and they developed and adapted EHR I-PASS templates with some convenient autopopulation capabilities. A manual was developed which summarised the use of I-PASS templates for specific handover applications.
Integration with the hospital EHR has been a valuable adjunct to foster I-PASS implementation. It provides detailed, I-PASS formatted, computer-accessible or typed summaries of patient information that reinforce and supplement verbal handovers, thereby increasing both their efficiency and accuracy.
Local resource leaders
Similar to the experience with surgical checklists,57 we realised that simply teaching I-PASS without an explicit plan to encourage and monitor local implementation was likely to fail. We also recognised the need to transition responsibility for adopting and sustaining I-PASS from a few CQS project leaders to a larger group of local operational leads.
One important tactic was identification of 15 department and unit-level resource leaders to serve as local champions and educational resources; they assumed progressively greater responsibility for coordinating local I-PASS implementation on their service or unit.
Observers
Resource leaders recruited additional residents, faculty and senior nurses and technicians on their services to serve as handover observers. Ideally, these observers understood the I-PASS system and were also familiar with the individual patients being discussed. They could therefore assess both I-PASS adherence and clinical content. Additional I-PASS education and supplemental training in observation and grading were provided for these individuals.
Observations provide empirical data regarding I-PASS compliance; they reinforce the commitment of the institution to this process; and they provide an opportunity for immediate feedback and education. A form was developed and vetted through our Handover Committee for use in observing and grading handovers, and this was also made available as a smartphone application (see online supplementary file 1).
supplementary file
Workflow mapping, focus groups and demonstration projects
Handover workflows were mapped in a number of departments, and focus groups were held with various constituencies, including the Housestaff Quality and Safety Committee, to expose barriers to I-PASS implementation and discuss mitigation strategies. I-PASS leaders worked with selected services and departments to develop demonstration projects that addressed implementation barriers or expanded I-PASS into new areas (eg, cross-departmental and cross-venue handovers).
Study of the intervention
Evaluation of implementation effectiveness was guided by the four-stage Kirkpatrick model.51
Measures
Measures included Kirpatrick level 1—reaction (do trainees feel it was a valuable experience) and level 2—learning evaluations (did you impart the desired knowledge and achieve the educational objectives), which were ascertained using structured, post-training surveys; and Kirpatrick level 3—behaviour (are the trainees actually applying the new knowledge changing behaviour), determined using monthly departmental or service-level handover observations. Kirpatrick level 4—results (impact on patient quality and safety) data were not obtained, as discussed in the Limitations section.
Analysis
Descriptive survey and observation results were analysed by department and service, and over time. Results were displayed in both tabular and graphic formats.
Ethical considerations
This is an institution-wide, operational implementation rather than a research project, and Institutional Review Board review was not sought.
Results
Physician results
Post-training surveys (see online supplementary file 2) have generally shown 80%–100% positive responses to Kirkpatrick level 1 (eg, content, pace, length, educational tools) and Kirkpatrick level 2 (acquisition of the desired knowledge, skills and attitudes, including I-PASS elements and characteristics of optimal handovers) evaluations. Trainee feedback did result in a reduction of full training programme length from 2–3 to 1–2 hours.
Online supplementary file 1 shows an observation form, available as a printed document or smartphone application, which is used to track I-PASS compliance (Kirkpatrick level 3) across units and longitudinally. Online supplementary file 3 is an example of 1 month's Kirkpatrick level 3 outcomes from a single department, during which nine handovers were observed.
After collection from each department, physician handover observation data are aggregated and updated by CQS for each I-PASS question and observation period (table 2) and the total number of monthly observations by each department is also tabulated (table 3). There is wide variability across departments in the number of monthly and total handover observations, indicating we have not yet achieved the desired level of institutional adoption and consistency.
Monthly summary of physician observation results
Observations by department: 2016
Figure 1 shows hospital-wide Kirkpatrick level 3 physician observation results from table 2, plotted over time. Subsequent to our October 2015 pilot, the formal observation programme began in April 2016 and has been conducted monthly thereafter (except October 2016 due to technical issues). Scores are provided for inclusion of each of the five I-PASS elements, correct sequence, giver preparedness and receiver engagement. Initially low scoring areas (illness severity, situational awareness and contingency planning, synthesis and correct sequence) all improved substantially, while patient summary, action list, and giver and receiver performance were high initially and remained so. Scores for synthesis were consistently among the lowest.
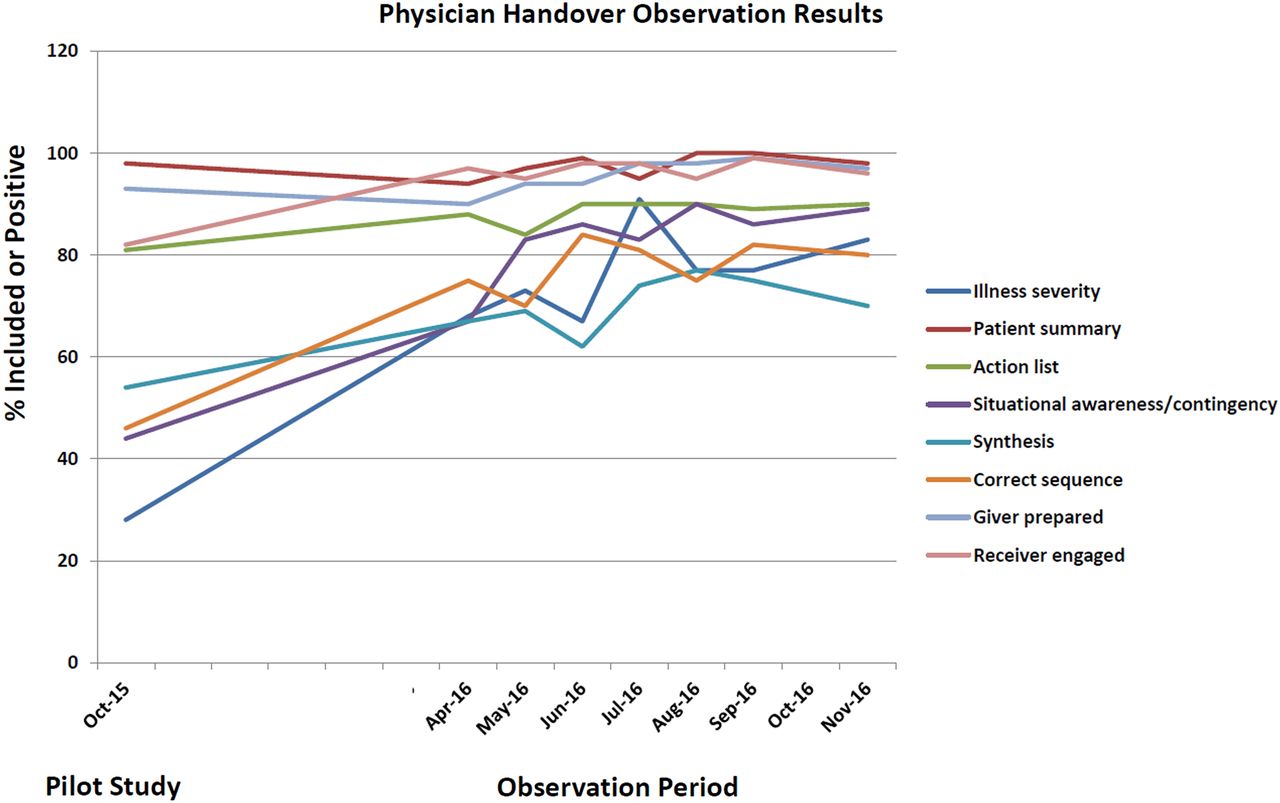
Physician I-PASS Handover Observation Results (October 2015 pilot; April through November 2016 observations). Hospital-wide Kirkpatrick level 3 results of physician handover observations at the department or service level, including data from the October 2015 pilot and subsequent April through November 2016 (except October 2016) observation cycles. Scores are plotted for inclusion of each of the five I-PASS elements, correct sequence, giver preparedness and receiver engagement. Initially low scoring areas (illness severity, situational awareness and contingency planning, synthesis and correct sequence) all improved substantially, while patient summary, action list and giver and receiver performance were high initially and remained so.
Patient Care Services (Nursing) results
Figure 2 shows observation results for selected nursing units as compiled by MGH Patient Care Services. Similar to the departmental results, which focused more on physicians, nursing results show initially high and relatively stable scores for patient summary and action list, as they have historically been included in most handovers. Illness severity, situational awareness/contingency planning and synthesis were incorporated less frequently in the pre-implementation period but rapidly increased postimplementation.

{kind=link}
{kind=link}
Patient Care Services (Nursing) Pre and PostImplementation Observation Results. Observation results for selected nursing units. Similar to the departmental results, which focused more on physicians, nursing data show initially high and relatively stable scores for patient summary and action list, both of which have been included historically in most handovers. Illness severity, situational awareness/contingency planning and synthesis were incorporated less frequently in the pre-implementation period but rapidly increased postimplementation.
Discussion
Summary and interpretation
The MGH I-PASS initiative represents, to our knowledge, the largest single institution implementation of this handover system in a tertiary general hospital with a predominantly adult population. Our initiative is also unique in breadth, encompassing all caregivers, services and units.
We have demonstrated that successful training of large numbers of caregivers can be achieved by a relatively small team of committed project leaders, with modest direct costs and without sacrificing operational effectiveness. Centralised leadership and decentralised local champions have complementary roles and value. Availability of I-PASS functionality within our EHR was particularly valuable when used to its maximum potential. We strongly advise the early involvement of resident leaders in I-PASS initiatives, as they can provide critical insights on implementation barriers such as workflow and systems issues.
Our goal of more expansive I-PASS implementation also exposed challenges that are likely not unique to MGH. Unlike early initiatives that focused primarily on doctors in paediatric units, our population of caregivers, services and locations was much more diverse. Rather than imposing a single model, we emphasised adaptation of the basic I-PASS structure to service-specific needs. For example, essential details within the patient summary may be much different on an obstetrics and gynaecology service than a medical oncology unit. Notably, there is no prescribed amount of information detail or time for an I-PASS handover, and it may be quite short for a stable patient about to be discharged.
Adoption of I-PASS on surgical services has been less consistent than on medical and paediatric units. In focus groups, surgical staff and residents noted that they often covered a large number of patients, many of them postoperative and completely stable, and there was insufficient time to do a formal I-PASS handover on every one. We encouraged surgical services to appropriately adapt the basic I-PASS structure, especially for straightforward patients.
In our experience, synthesis or readback was the most challenging feature of I-PASS for clinicians. Although ubiquitous in other high-reliability professions such as military or commercial aviation, it has until now been rare in healthcare, and many clinicians find it awkward. Also, some services routinely conducted handovers using secure email or other types of asynchronous, one-way communication rather than direct face-to-face or telephonic methods. Adding I-PASS synthesis (readback) would require substantial workflow changes which were not always acceptable to the clinicians.
Complaints about I-PASS sometimes noted ‘insufficient time’ to do structured handovers on every patient being covered. We believe this is not an I-PASS issue per se, but rather reflects the challenges of covering large numbers of patients, especially in the era of duty-hour restrictions. In fact, I-PASS should facilitate efficient and effective handovers because it is structured and standardised.
Ultimately, for I-PASS to be sustained within an institution, cultural change is required. Education is the easiest aspect of an I-PASS initiative. Assuring widespread, consistent adoption and sustaining this over time requires that it be imbedded within the organisational culture.66
Limitations
Because of the scope and scale of our implementation, as well as competing initiatives, it was necessary to roll out I-PASS over a period of several years. This created challenges when attempting to incorporate I-PASS into cross-departmental or cross-venue handovers if one of the areas had not yet fully adopted I-PASS. Another consequence of this asynchronous roll-out was that observational data were not available from every department and unit for every time period.
MGH is a large, metropolitan, academic medical centre where resident handovers predominate. While this could potentially limit generalisability, we believe that the basic principles described could be easily extrapolated to other types of institutions.
Without active surveillance by trained nurses and physicians,5 Kirkpatrick level 4 results (eg, reduction in handover-related adverse events and medical errors) are challenging and costly to acquire in a non-investigational, operational setting. Also, it can be difficult to specifically link improved outcomes to I-PASS, because most institutions conduct multiple process improvement activities at any time. As a less resource-intensive proxy for active surveillance, in phase II we plan to use surveys similar to those of Kitch and associates,2 in which caregivers are explicitly asked about handover-related adverse events in their recent experience.
We are also cataloguing safety reports citing inadequate handovers as a causative factor. However, such results are difficult to interpret as we are simultaneously encouraging more safety reporting in general. Finally, in 1–2 years we will be conducting our periodic safety culture survey update and will specifically assess the impact of I-PASS implementation on the handovers and transitions of care domain.
Conclusions
From 2013 to 2016, we initiated large-scale, multidisciplinary I-PASS training and implementation at a major academic medical centre, with promising early results and actionable lessons for ongoing refinement. Although a major institutional effort, this was conducted with little cost beyond the time of the lead staff. Phase II will include further adoption strategies: customising the tool for specific disciplines and workflows, expanding to other types of handovers and measuring Kirkpatrick level 4 outcomes or their proxies. We believe that, once embedded in hospital culture, this approach has the potential to dramatically improve patient care.
Acknowledgments
The authors acknowledge the support of MGH senior leadership, Patient Care Services leaders and staff, the MGH Norman Knight Center for Clinical and Professional Development, members of the MGH Handover Committee and Housestaff Quality and Safety Committee, and the many Department Chairs, quality leaders, I-PASS Resource leaders and observers who have contributed to the success of this programme. We also are indebted to the I-PASS developers for their innovative contribution, and for the assistance they provided us during implementation.
References
Footnotes
Correction notice This article has been corrected since it first published Online First. The abstract has been added.
Contributors DMS, KMcE, LR, RGC, EM conceived and led the I-PASS initiative, collected and analysed data, and made critical manuscript revisions; DMS and RGC provided graphics; DMS drafted the original manuscript and revision, submitted the original manuscript and revision; and is responsible for the overall content.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.