Article Text

Abstract
Background Although important in clinical care, reports of inappropriate peripherally inserted central catheter (PICC) use are growing.
Objective To test whether implementation of the Michigan Appropriateness Guide for Intravenous Catheters (MAGIC) can improve PICC use and patient outcomes.
Design Quasi-experimental, interrupted time series design at one study site with nine contemporaneous external controls.
Setting Ten hospitals participating in a state-wide quality collaborative from 1 August 2014 to 31 July 2016.
Patients 963 hospitalised patients who received a PICC at the study site vs 6613 patients at nine control sites.
Intervention A multimodal intervention (tool, training, electronic changes, education) derived from MAGIC.
Measurements Appropriateness of PICC use and rates of PICC-associated complications. Segmented Poisson regression was used for analyses.
Results Absolute rates of inappropriate PICC use decreased substantially at the study site versus controls (91.3% to 65.3% (−26.0%) vs 72.2% to 69.6% (−2.6%); P<0.001). After adjusting for underlying trends and patient characteristics, however, a marginally significant 13.8% decrease in inappropriate PICC use occurred at the study site (incidence rate ratio 0.86 (95% CI 0.74 to 0.99; P=0.048)); no change was observed at control sites. While the incidence of all PICC complications decreased to a greater extent at the study site, the absolute difference between controls and intervention was small (33.9% to 26.7% (−7.2%) vs 22.4% to 20.8% (−1.6%); P=0.036).
Limitations Non-randomised design limits inference; the most effective component of the multimodal intervention is unknown; effects following implementation were modest.
Conclusions In a multihospital quality improvement project, implementation of MAGIC improved PICC appropriateness and reduced complications to a modest extent. Given the size and resources required for this study, future work should consider cost-to-benefit ratio of similar approaches.
- healthcare quality improvement
- hospital medicine
- implementation science
Statistics from Altmetric.com
Introduction
Peripherally inserted central catheters (PICCs) have become a popular modality for vascular access in hospitalised patients.1 2 Growth in the use of PICCs reflects inherent advantages of these devices, including safety during insertion,3 availability of nurse-led vascular access teams that offer bedside placement4 and ability to facilitate transitions of care.5
However, rapid adoption of PICCs has also led to concerns regarding inappropriate use. For example, a multicentre study showed significant variation in indications for PICC insertion, rates of PICC use and catheter dwell times.6 Notably, 25% of PICCs were removed within 5 days of insertion, a duration not considered appropriate by the Centers for Disease Control and Prevention professional guidelines.7 8 Similar concerns regarding PICC use have been reported by studies in adults and paediatric subsets.9 10
Variability in PICC indications and utilisation is concerning because these devices are associated with complications.11 For instance, PICCs are associated with rates of central line-associated bloodstream infection (CLABSI) that parallel conventional central venous catheters (CVCs).12 Similarly, PICCs are known to have a 2.5-fold greater risk of venous thromboembolism (VTE) when compared with traditional CVCs.13 Importantly, choices regarding PICC characteristics may moderate this risk. For instance, multilumen PICCs are associated with higher rates of occlusion, VTE and CLABSI than single-lumen devices.14–16 Yet physician knowledge of these factors is variable, at best.17 18 In order to ensure patient safety, strategies to improve PICC use appear necessary.
The Michigan Appropriateness Guide for Intravenous Catheters (MAGIC) is a tool designed to inform and improve clinical decision making with respect to vascular access devices.19 Although an important step forward, whether implementation of MAGIC can improve PICC use and decrease complications is not known. Therefore, in conjunction with a state-wide collaborative, we designed a study to implement MAGIC and evaluate its impact on PICC use and patient outcomes.
Methods
Study setting and design
We followed the Standards for Quality Improvement Reporting Excellence guidelines for this study.20 The intervention site was a 600-bed urban, community teaching hospital that participates in a large, multihospital, state-wide quality improvement collaborative.21 The design and setting of this consortium have been previously described.19 22 23 In brief, hospitals belonging to the consortia have been prospectively collecting data on a sample of hospitalised patients with PICCs since 2014. Adult patients admitted to a general medicine ward or intensive care unit (ICU) of a participating hospital who receive a PICC for any reason during clinical care are eligible for inclusion. Patients who are (1) under the age of 18; (2) pregnant; (3) admitted to a non-medical service (eg, general surgery); or (4) admitted under observation status are excluded. Trained data abstractors collect data directly from medical records. Following PICC placement, all patients are followed until PICC removal, death or 70 days (whichever occurs first). For this study, we selected nine control sites including academic and community hospitals focused on improving PICC use and outcomes.
Study intervention
A quasi-experimental, interrupted time series design was used. All sites collected PICC data and participated in quarterly collaborative meetings, where they received an overview of MAGIC and practices to improve PICC use and outcomes. At the study site, a MAGIC-based intervention was implemented through the vascular access team and included (1) a MAGIC-based tool to evaluate appropriateness of PICC placement prior to insertion; (2) training for vascular access nurses on alternative peripheral venous access devices as recommended by MAGIC; (3) changes to the electronic medical record (EMR) that incorporated MAGIC recommendations; and (4) provider education regarding the importance of appropriate vascular access device selection.
MAGIC-based appropriateness tool
During the intervention, the vascular access team evaluated appropriateness of every PICC order using a standardised approach. In accordance with MAGIC, three criteria were used to determine PICC appropriateness: indication for PICC insertion, proposed duration of PICC use and the nature of the infusate (online supplementary appendices A and B). If a PICC was deemed appropriate, it was placed as requested; however, if the PICC was deemed inappropriate, the vascular access team contacted the ordering provider to discuss alternative devices in accordance with MAGIC recommendations (eg, ultrasound-guided peripheral intravenous or midlines).
Dedicated training on peripheral venous access alternatives
To support insertion of MAGIC-recommended devices, all vascular access team nurses were enrolled in a 4-hour education programme that included ultrasound training and peripheral venous alternatives to PICCs. Training on midline and ultrasound-guided intravenous catheter insertion, indications for use and management was provided. Midline devices are vascular catheters approximately 3–8’ in length that are placed in the veins of the upper arm and terminate distal to the subclavian vein; thus, they are considered peripheral catheters.24 Ultrasound-guided intravenous catheters include standard peripheral catheters (approximately 1’ in length) as well as extended dwell peripheral catheters (devices that are 2–3’ in length) that can reach deeper veins of the arm, both inserted under direct ultrasound visualisation.25
EMR changes that incorporated MAGIC recommendations for device choice
In addition to vascular access nurse triage, changes to the EMR were introduced to identify the appropriate vascular access device for intravenous medications based on MAGIC and Infusion Nursing Standards.7 19 Working with a multidisciplinary committee, devices were highlighted by pharmacists in the order entry and medication section of the EMR so that the ordering provider could easily (1) determine whether central venous access for a particular medication was required; and (2) determine the need for a multilumen device (see online supplementary appendix C).
Supplementary file 3
Provider education
Ongoing physician and trainee education through departmental meetings (eg, medical grand rounds), dedicated resident education sessions (eg, morning reports) and nursing huddles were used to inform providers about the intervention. These meetings were also used to highlight risks associated with multilumen PICCs, capabilities of midlines and MAGIC criteria for PICC use.
External control sites
In order to account for secular trends, a contemporaneous external control that included nine peer hospitals was used. Like the intervention site, all control sites collected PICC data and participated in quarterly meetings. Control sites also engaged in ad hoc quality improvement initiatives that included changes to EMR systems, provider education, and audit and feedback of PICC characteristics and outcomes. However, control sites did not implement MAGIC in a formal fashion during the study period.
Data sources
Data on patient characteristics, appropriateness measures and device-related complications at the study and control sites were collected through the quality collaborative. Additionally, data on the number of single, double and triple lumen PICCs, midlines, and number of patient-days for all hospitalised patients (to estimate overall PICC and midline utilisation) were obtained from the intervention site.
Definitions
The overall rate of PICC and midline insertion was expressed as the total number of PICCs or midlines placed per month divided by the total number of patient-days for all hospitalised patients. In accordance with MAGIC, inappropriate PICC use was defined as a composite of (1) PICC placement for peripherally compatible infusions for ≤5 days; (2) PICC placement in a patient in an ICU for ≤14 days; or (3) placement of a multilumen PICC when a single-lumen PICC would have been appropriate. VTE included symptomatic upper extremity deep vein thrombosis (DVT) or pulmonary embolism that was radiographically confirmed (ie, ultrasound or CT). In accordance with the Centers for Disease Control and Prevention/National Healthcare Safety Network criteria,26 CLABSI was defined when a patient had a confirmed positive blood culture with a PICC in place for 48 hours or longer without another identified infection source, or if a PICC tip culture was positive in the setting of clinically suspected infection. Catheter occlusion events were captured when documented in the medical record, or when tPA was administered for problems with PICC aspiration or infusion.
Outcome measures
The primary outcome of interest was the composite measure of inappropriate PICC use before and after implementation of MAGIC in study versus control sites (expressed as a proportion and as a rate per 1000 PICC days). Secondary outcomes included (1) individual measures of PICC appropriateness and (2) PICC-associated complications between preimplementation and postimplementation period in study and control sites. Additionally, post hoc analyses that examined (1) overall PICC and midline utilisation per 1000 patient-days and (2) the proportion of single, double and triple lumen PICCs from the preimplementation to postimplementation period in the study site were performed.
Statistical analysis
Descriptive statistics were used to tabulate patient characteristics and summarise age, length of stay (LOS), body mass index (BMI) and Charlson Comorbidity Index (CCI) across sites. Differences between preimplementation and postimplementation populations were assessed using t-test, Χ2 test and Wilcoxon rank-sum test. Similarly, differences in the mean rate of PICC and midline utilisation from preimplementation to postimplementation were assessed using paired two-sample t-tests. Differences in inappropriate PICC use between preimplementation and postimplementation periods were assessed using logistic regression, adjusting for patient age, gender, race, LOS, BMI and CCI. An interaction term (time×site) was added to assess pre–post differences between the intervention and control sites.
Segmented Poisson regression was used to assess the effect of the intervention on rates of inappropriate PICC use. Separate models were fit to intervention and control sites, adjusted for age, gender, race, LOS, BMI and CCI per month. Models were tested for overdispersion and autocorrelation using recommended methods.27 28 Counts were offset by the natural logarithm of the total number of PICC days per month with robust estimators of variance. Pre–post differences in the rates of inappropriate PICC use between sites (study/control) were tested by including an interaction term.29 Results were reported as incidence rate ratios (IRR) and 95% CIs. All statistical tests were two-sided, with P<0.05 considered statistically significant. All analyses were conducted on Stata V.14.
Results
Data were collected between 1 August 2014 and 31 July 2016. The intervention was launched on 1 August 2015; thus, information was available for 12 months preimplementation and postimplementation. At the intervention site, a total of 2131 PICCs were placed during the study period. Sixty per cent (n=1278) of PICCS were placed prior to implementation, whereas the remaining 40% (n=853) were placed in the postimplementation period. Of these patients, data on 517 and 446 inpatients with PICCs in the preimplementation and postimplementation period were evaluated. In comparison, data from a total of 3530 and 3083 inpatients with PICCs were included from 9 (control) hospitals preimplementation and postimplementation, respectively.
Differences in patient characteristics between the baseline and postintervention period at the intervention site and controls were noted (table 1 and online supplementary appendices D and E). For example, at the intervention site, patients in the preimplementation period were more often female (60.9% vs 47.8%, P<0.001) and less often diagnosed with mild liver disease (5.8% vs 9.4%, P=0.033), chronic kidney disease (26.7% vs 39.7%, P<0.001) and chronic obstructive pulmonary disease (35.2% vs 44.0%, P=0.006) than patients postintervention. Similarly, patients in the preperiod had a shorter median length of hospital stay and lower CCI when compared with patients in the postperiod (11 vs 12 days, P=0.015 and 3.05 vs 4.18, P<0.001, respectively).
Supplementary file 4
Patient characteristics at the intervention ite
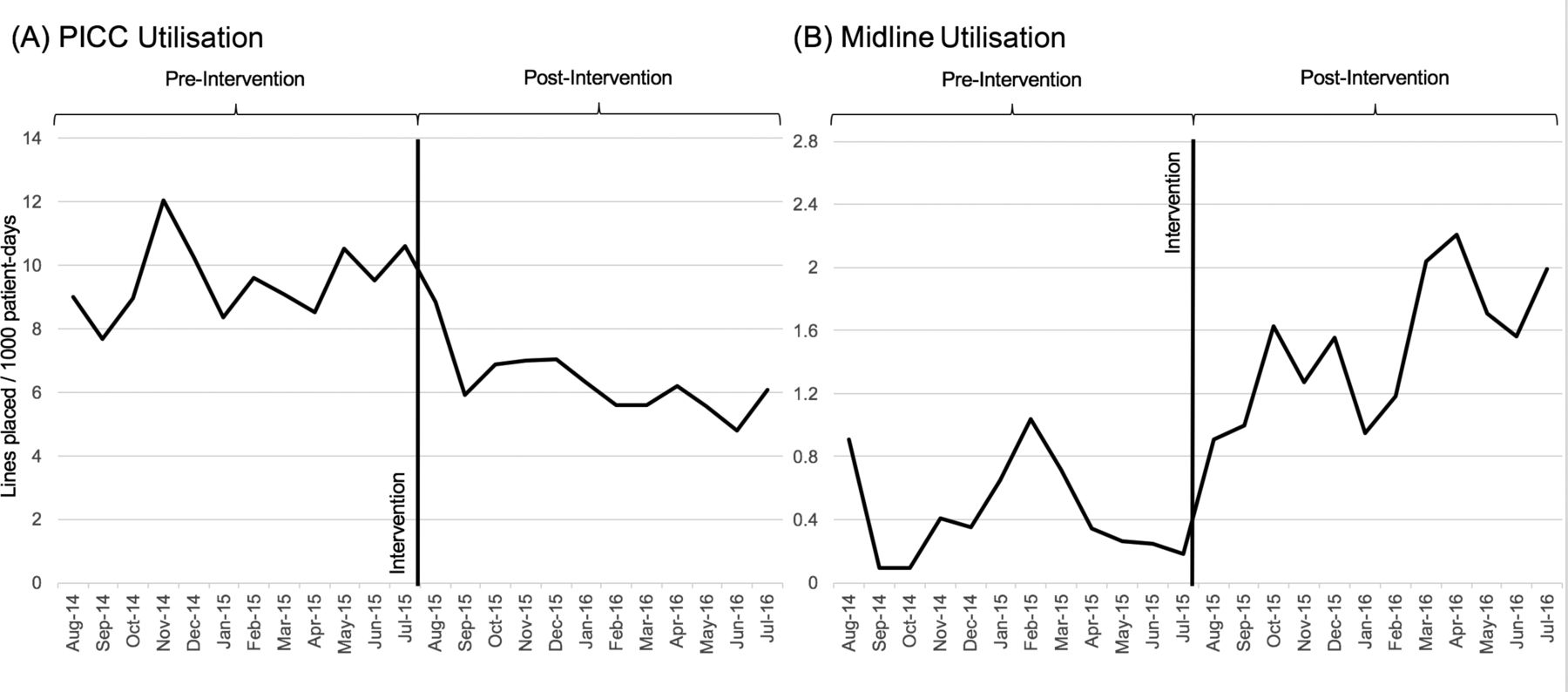
Following implementation of MAGIC, the mean rate of PICC use at the intervention site significantly decreased from 9.51 to 6.31 PICCs per 1000 patient-days (P<0.001) (figure 1A). As the rate of PICC utilisation declined, the rate of midline use increased from a mean of 0.44 to 1.50 midlines/1000 patient-days (P<0.001) (figure 1B). Use of multilumen PICCs decreased at the intervention site from 85.7% to 54.3%, while use of single-lumen PICCs increased from 14.3% to 45.7% between the preimplementation and postimplementation period (P<0.001 for both) (figure 2).

Utilisation of (A) peripherally inserted central catheter (PICC) and (B) midlines before versus after implementation. All rates expressed as devices per 1000 catheter days at study site.

Proportion of single-lumen, double-lumen and triple-lumen peripherally inserted central catheter (PICC) use at the intervention site before versus after implementation.
After adjusting for patient characteristics, inappropriate PICC placement decreased from 91.3% (n=472) to 65.3% (n=291) at the intervention site, representing an absolute decrease of 26.0% (P<0.001). In comparison, a smaller but statistically significant decline in inappropriate PICC use was observed at control sites (72.2% vs 69.6%, absolute decrease of 2.6%; P<0.001). The extent of the decrease was greater at the intervention site compared with the control (P<0.001). The greatest improvement in individual measures of PICC appropriateness occurred for PICC use ≤5 days and PICC use ≤14 days in ICU at the intervention site (24.6% to 13.5%, P<0.001; 32.3% to 18.6%, P=0.003, respectively). At control sites, both PICC placement ≤5 days and ICU PICC placement ≤14 days minimally increased. There was a 26.7% decrease in multilumen PICC use (89.5% vs 62.1%, P<0.001) at the intervention site. The extent of this decline was significantly greater than the 3.8% decrease (67.3% vs 63.5%, P<0.001) at the control sites (P<0.001 for the interaction term) (table 2).
Measures of PICC appropriateness before versus after implementation of MAGIC
After accounting for underlying trends and adjusting for patient characteristics by month and site (age, race, gender, LOS, BMI and CCI), a 13.8% decrease in the rate of inappropriate PICC use was observed at the intervention site (IRR: 0.86; 95% CI 0.74 to 0.99, P=0.048). No significant changes in the rate of inappropriate PICC use was observed for controls (figure 3). The interaction term was significant (P=0.003), indicating that the extent of the decline was greater at the intervention site compared with control sites.

{kind=link}
{kind=link}
{kind=link}
Effect of MAGIC on rate of inappropriate PICC use in intervention versus control sites. Inappropriate PICC use= a) PICC dwell for ≤5 days for peripherally compatible therapy;b) PICC placement in an intensive care unit for ≤14 days; c)multilumen PICC use when single lumen appropriate. Control sites=9 peer collaborative hospitals. Models adjusted for patient age, gender, race, body mass index, length of stay and Charlson Comorbidity Index. MAGIC, Michigan Appropriateness Guide for Intravenous Catheters; PICC, peripherally inserted central catheter.
The proportion of patients with (any) PICC-related complication decreased at the intervention site compared with controls (33.9% to 26.7%, vs 22.4% to 20.8%, in the preimplementation vs postimplementation periods, respectively). The extent of the decrease at the intervention site was greater than control sites (P=0.036, interaction term). With respect to individual complications, the proportion of patients experiencing catheter occlusion at the intervention site decreased by 6.4% (28.4% to 22.0%, P=0.011) from preimplementation to postimplementation; no significant change in the proportion of patients with occlusion was observed at control sites. No significant change in the proportion of patients with VTE or CLABSI at intervention or control sites was observed (table 2).
Discussion
In this study, implementation of MAGIC led to improvements in PICC use and outcomes. Although rates of inappropriate PICC use improved overall, the magnitude of improvement at the study site following adjustment was modest. While the change in performance did outpace the secular trend (suggesting that MAGIC was effective), the size, scope and effort needed to improve PICC use were substantial. Specifically, a multimodal intervention that included education, changes to the electronic order set, training of vascular access nurses and a decision tool was necessary. As MAGIC recommendations regarding the number of device lumens and dwell time in ICU and ward settings improved at the study site, this may have been the ‘active ingredient’ in moderating change. Similarly, while a reduction in the overall proportion of patients who experienced a PICC complication only occurred at the study site, the effect was largely due to reduction in catheter occlusion likely from choices regarding lumens. Somewhat disappointingly, major complications such as CLABSI and DVT did not change, perhaps owing to low rates overall as well as our sampling strategy.30 Collectively, while these data suggest that an intervention using MAGIC has the ability to improve PICC safety in hospitals, whether or not such interventions are pragmatic in the context of resource use and impact is unclear.
The question as to which of the intervention components was the ‘active ingredient’ in improving PICC use is important to consider. For example, standardising recommendations via an appropriateness tool empowered vascular access nurses to apply evidence at the ‘point of care’. Similarly, introducing alternative peripheral venous access devices for patients that require short-term venous access led to decreased reliance on PICCs. The vascular access team also developed new and enhanced skills, including use of ultrasound for ‘difficult’ venous access and a midline programme. The creation of these alternatives, in turn, necessitated education and orientation of ordering clinicians not familiar with these devices. This type of education is labour-intensive and requires longitudinal reinforcement. Finally, introduction of EMR-based changes helped implementation for both physicians and the vascular access team. Importantly, this initiative has allowed the vascular access team at the intervention site to move from being viewed as ‘operators’ who place PICCs to ‘consultants’ for the right vascular device for the right patient at the right time.
It is important to acknowledge that implementing MAGIC was not without financial commitment from the hospital. For one, the initiative included purchase of additional hand-held ultrasound equipment (approximately $10 000) and expenses related to educational sessions. Although the return on this investment was considered reasonable in terms of cost savings from reduced PICC use and increased appropriateness, the only significant reduction in complications observed was occlusion. While an overall decrease in rates of CLABSI and VTE was noted, these did not reach statistical significance. Thus, future quality improvement initiatives seeking to deploy MAGIC (or related real-world, multimodal initiatives) must carefully consider whether the effort and resources required are reasonable when weighing return on investment. In this context, it is important to acknowledge that this work was conducted in a collaborative whose member hospitals were actively engaged in PICC quality improvement—predisposing to a strong secular trend or ‘rising tide’ phenomenon.31 Effects in more ‘naive’ settings might vary and would be important to evaluate in future studies.
Our study has limitations. First, the intervention was conducted in a single community hospital; thus, findings are difficult to generalise to other settings. Furthermore, since data collection through the quality collaborative is focused on hospitalised adult medical patients, impact of the intervention on surgical patients is unknown. Second, the intervention had multiple components; thus, it was not possible to isolate which MAGIC element served as the ‘active ingredient’ or whether all elements were necessary. Third, while overall rates of complications improved, the magnitude of the impact was less than anticipated and largely limited to catheter occlusion.
Our study also has important strengths. First, we used rigorous methods including an interrupted time series design with external controls to assess the influence of MAGIC on PICC outcomes and complications. Second, MAGIC was effective despite implementation within collaborative hospitals that are actively focused on measuring and improving PICC outcomes. Third, our findings highlight the importance of a multidisciplinary approach to improving decisions in vascular access. By engaging and empowering vascular nurses to improve decision making related to PICCs, important gains in safety were made. Given that vascular access is one of the most commonly used procedures in hospitals and reports of inappropriate PICC use are growing, these data are of importance to hospitals and health systems across the nation.
In conclusion, we found that implementation of MAGIC improved overall PICC use and appropriateness. Future studies to validate this effect across multiple sites, assess cost-effectiveness and evaluate impact on complications such as CLABSI and VTE among patients with PICCs now appear necessary.
Supplementary file 1
Supplementary file 2
References
Footnotes
Funding Agency for Healthcare Research and Quality, 10.13039/100000133, 1-K08HS022835-01.
Competing interests SF discloses royalties from Wiley Publishing; honoraria for various talks at hospitals as a visiting professor; grants from CDC Foundation, Agency for Healthcare Research and Quality (AHRQ), and Blue Cross Blue Shield of Michigan; and expert witness testimony. All other authors disclose no conflicts.
Ethics approval University of Michigan Medical School. Since the purpose of this state-wide collaborative is to measure and improve the quality of existing care practices, this study was assigned a ’not regulated' status based on hospital-specific IRB criteria.
Provenance and peer review Not commissioned; internally peer reviewed.