Article Text

Abstract
Background Computerised prescriber order entry (CPOE) systems users often discontinue medications because the initial order was erroneous.
Objective To elucidate error types by querying prescribers about their reasons for discontinuing outpatient medication orders that they had self-identified as erroneous.
Methods During a nearly 3 year retrospective data collection period, we identified 57 972 drugs discontinued with the reason ‘Error (erroneous entry).” Because chart reviews revealed limited information about these errors, we prospectively studied consecutive, discontinued erroneous orders by querying prescribers in near-real-time to learn more about the erroneous orders.
Results From January 2014 to April 2014, we prospectively emailed prescribers about outpatient drug orders that they had discontinued due to erroneous initial order entry. Of 2 50 806 medication orders in these 4 months, 1133 (0.45%) of these were discontinued due to error. From these 1133, we emailed 542 unique prescribers to ask about their reason(s) for discontinuing these mediation orders in error. We received 312 responses (58% response rate). We categorised these responses using a previously published taxonomy. The top reasons for these discontinued erroneous orders included: medication ordered for wrong patient (27.8%, n=60); wrong drug ordered (18.5%, n=40); and duplicate order placed (14.4%, n=31). Other common discontinued erroneous orders related to drug dosage and formulation (eg, extended release versus not). Oxycodone (3%) was the most frequent drug discontinued error.
Conclusion Drugs are not infrequently discontinued ‘in error.’ Wrong patient and wrong drug errors constitute the leading types of erroneous prescriptions recognised and discontinued by prescribers. Data regarding erroneous medication entries represent an important source of intelligence about how CPOE systems are functioning and malfunctioning, providing important insights regarding areas for designing CPOE more safely in the future.
- information technology
- medication safety
- patient safety
Statistics from Altmetric.com
Background
The US Academy of Medicine has estimated that more than 1.5 million people are harmed by medication errors each year. Computerized Prescriber Order Entry (CPOE) systems have been widely advocated as a way to reduce such errors.1 However, these systems may also introduce errors, and the National Academy of Medicine has recommended that studies should be conducted to better understand errors related to health information technology in general, and electronic prescribing in particular.2 Earlier studies by our team and others have identified a variety of ways in which CPOE may contribute to medication errors.3–5
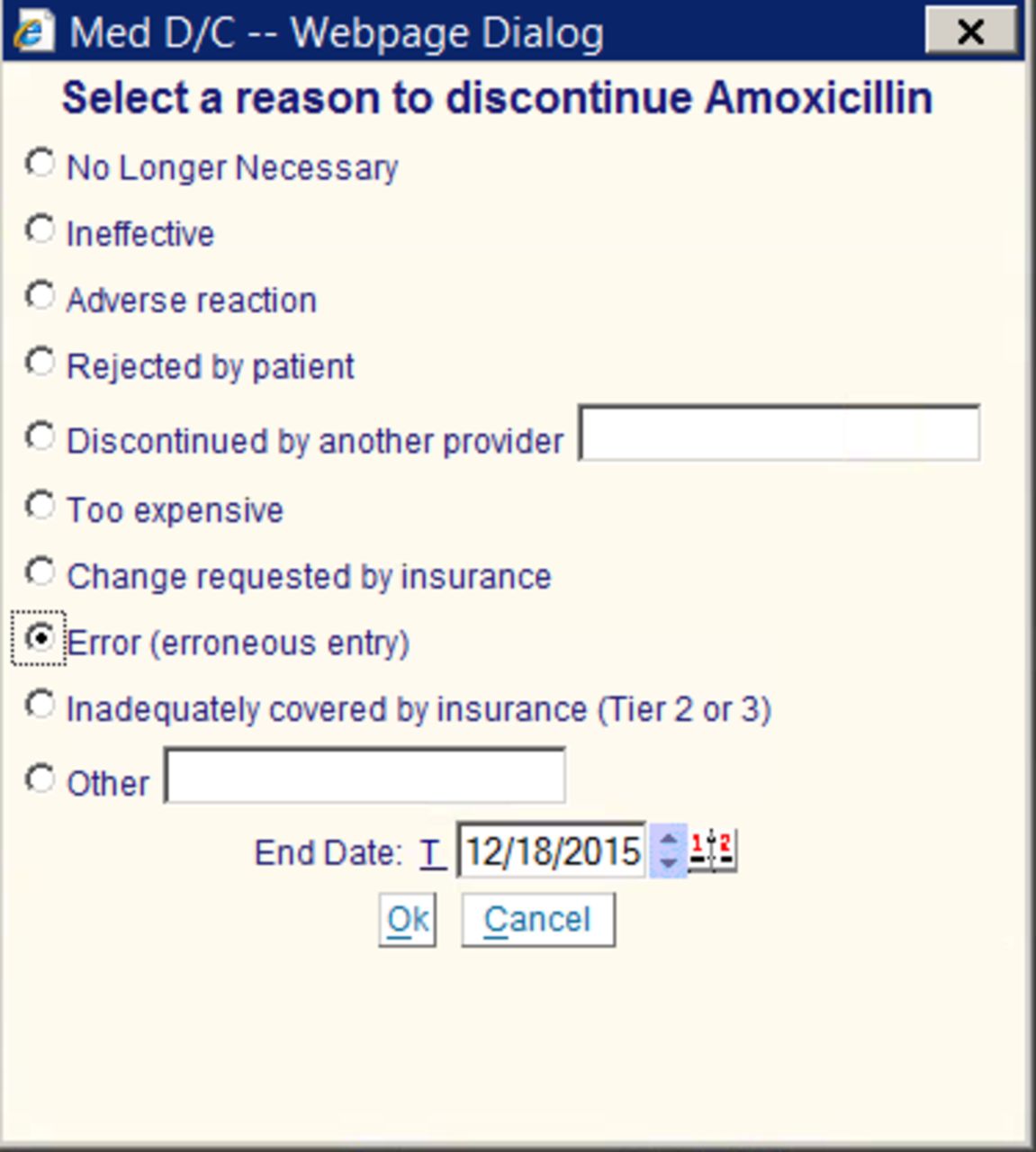
One potentially useful and innovative way to identify potential CPOE errors is to examine electronic orders placed, but subsequently discontinued.6–8 At Brigham and Women’s Hospital (BWH) in Boston, Massachusetts, any order discontinued in our home-grown outpatient electronic health record (EHR) system, the Longitudinal Medical Record (LMR), required the provider to give the reason for the discontinuation. Among the structured choices for reasons was ‘Error (erroneous entry)’ (figure 1). We discovered that thousands of orders were discontinued each year with this reason selected indicating that they were ‘erroneous.’ However, the descriptions of and reasons for these potential errors have not been previously studied.

Screenshot of prompt prescribers received to select a reason when discontinuing a medication in the BWH Longitudinal Medical Record, our legacy home-grown outpatient electronic health record system.
This study is part of a larger study funded by the US Food and Drug Administration, called the Computerized Prescriber Order Entry Medication Safety (CPOEMS) study that examined ways CPOE systems may contribute to or cause medication errors.9 The aim of the part of the CPOEMS study reported here was to investigate drugs discontinued with the reason ‘erroneous prescription’ entered by the discontinuing prescriber to better understand the types and causes of potential CPOE-related errors. We first performed a retrospective review of patient charts; however, because charts reviewed contained little or no information documenting reason(s) why prescribers discontinued these prescriptions and marked them as erroneous, we designed a prospective study to ask clinicians via email query in near real time to provide additional details about these ‘erroneous’ orders.
Methods
We carried out this study at BWH, a large US academic medical centre (AMC) with a home-grown EHR that prompts clinicians for a reason whenever a drug order is discontinued in the outpatient CPOE system. We initially undertook a retrospective study of a sample of nearly 60 000 discontinuations coded as ‘Error (erroneous entry)’ in a nearly 3-year period. We conducted chart reviews focusing on a sample of patients who most likely represented errors. We sampled and reviewed charts of medication discontinuations where the provider reordered a drug(s) with similar sounding names as well as medication orders that were discontinued shortly after being written. When chart reviews from several hundreds of these patients were found to have limited information about the errors, we elected to prospectively study consecutive patients by querying the clinician placing the discontinuation order in near real time (within 24 hours) to learn more about the erroneous orders. For a 4-month period from January 2014 to April 2014, we sent an email to the physician who signed a discontinuation order within 24 hours of discontinuing the drug, requesting additional details for the reason the drug was discontinued due to error. Working with a programmer, we developed a tool that automatically flagged all medication orders discontinued due to error and generated an email to the prescribers each morning about any drugs they had discontinued the previous day for which they had selected ‘Error (erroneous entry)’ as the discontinuation reason. All physicians (or other prescribing clinicians) at our hospital were included in the sample. To avoid burdening prescribers, these emails were sent only for one such erroneous entry discontinuation for each physician during the 4-month study period (thus, each flagged prescriber received only one email request).
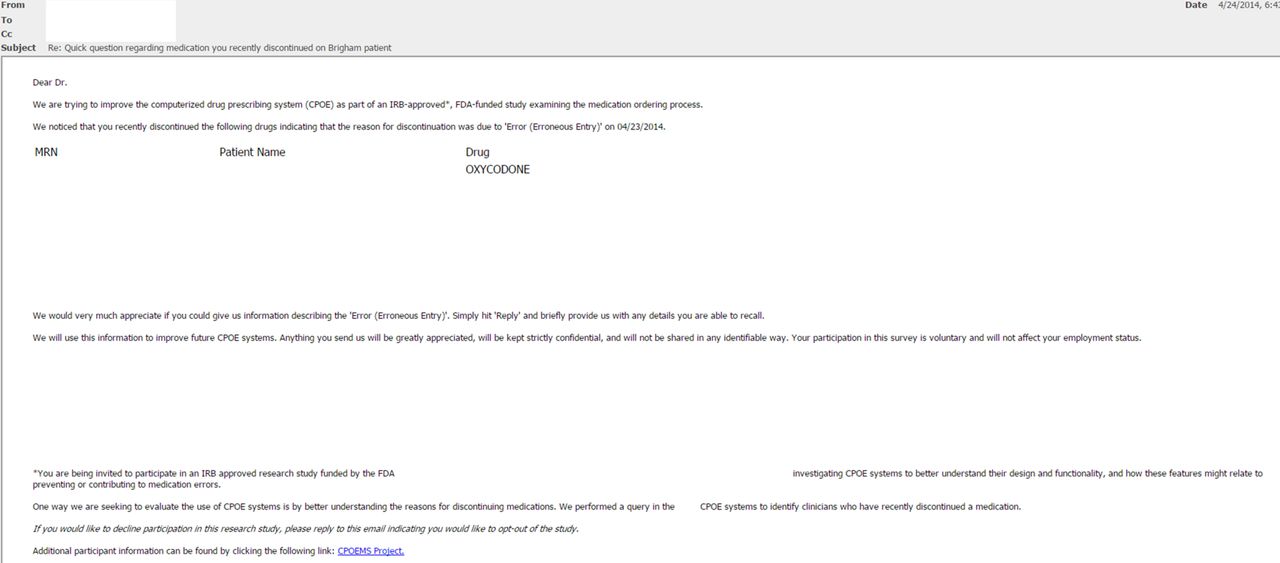
Ordering information details, such as patient name and medications, were provided in the email to remind clinicians of the specific patient and order involved. The email simply asked providers to reply to the message in free text providing more details about the error (see figure 2). Responses from the providers were compiled and coded by two pharmacists using a previously published taxonomy3 to describe what happened/what went wrong in the CPOE system and what happened to the patient. Any uncertainty or differences in coding between the pharmacists were adjudicated among our study team during team meetings. The study was conducted with the approval of the Partners HealthCare Human Subjects Research Committee.

{kind=link}
{kind=link}
Email sent to prescribers at our hospital who discontinued a medication indicating the reason ‘Error (erroneous entry).’
Results
During a nearly 3-year retrospective data period, a total of 57 972 drug orders were discontinued in the LMR with the reason ‘Error (erroneous entry).’ This represented 4.4% of all drug discontinuations between January 2011 and November 2013. When we retrospectively sampled these 200 charts to investigate, we discovered that we were unable to find documentation of the reasons or details related to why prescribers were indicating ‘Error (erroneous entry)’ as the reason for discontinuing the drug(s). There were no comments in the patients’ records or notes mentioning the reasons for the discontinuations.
A total of 250 806 medication orders were placed in the LMR during the 4-month prospective study period. Of these, 1133 (0.45%) were medications discontinued due to ‘Error (erroneous entry).’ We prospectively generated emails to 542 unique prescribers at BWH who discontinued a medication with ‘Error (erroneous entry)’ as the reason in these 4 months (ie, prescribers were only emailed once, and some had discontinued more than one medication within a single order). Of these 542 emails, we received responses from 312 (58%) of those contacted. Responses from providers regarding their reason(s) for choosing this discontinuation reason varied widely. Examples of the varying types of responses received regarding prescribers’ reasons for discontinuing a drug are listed in table 1. In some cases, clinicians explained that the reason for discontinuing the drug was not in fact related to an erroneous prior order, stating that they had erred in selecting this discontinuation reason with comments such as ‘…the auto choices were difficult to navigate for me, so my first attempt was wrong.’
Selected examples of verbatim responses from prescribers at Brigham and Women’s Hospital regarding their reasons for discontinuing a drug in error in the Longitudinal Medical Record
While we did not formally track clinical consequences, using as an example the mostly frequently discontinued in error drug, oxycodone (3%), we observed a variety of issues such as: the discontinued drug was initially written for with the wrong dose, the attending did not feel the drug was appropriate for this patient, it was already on the patient’s medications list (thus, it could have resulted in a duplicate prescription), the patient was unable to tolerate the pill form and instead needed the liquid form of the drug, the patient did not need opiates and the provider entered the drug in the wrong patient’s chart. Each of these reasons had the potential for undesirable clinical outcomes.
When the free text responses from the clinicians who replied to the email query were reviewed by two pharmacists and categorised using a previously validated taxonomy,3 the top reasons explicitly stated in their emails for ‘what happened in CPOE’ included: medication ordered for wrong patient (27.8%, n=60); wrong drug ordered (18.5%, n=40); and duplicate order placed (14.4%, n=31) (table 2). Prescriber responses also included comments that highlighted confusing aspects of the CPOE system and look-alike/sound-alike drugs. There were several instances where the response mentioned items had been erroneously added to the patients’ drug lists by non-physicians (eg, medical assistants) while assisting with medication reconciliation. Respondents never mentioned any information about what happened to the patient in their emails; thus, no responses for ‘what happened to the patient’ were coded.
Top reasons provided by survey responders for discontinuing medications with the reason ‘Error (erroneous entry)’
Discussion
Data regarding erroneous medication entries represent a potentially important source of intelligence about how CPOE systems are functioning and malfunctioning. We were disappointed to find that a retrospective manual chart review of a sample of clinical notes revealed no explanations or documentation of the reasons for these ordered-in-error orders. To overcome this limitation, we developed an automated approach to prospectively survey physicians who discontinued prescriptions as ‘Error (erroneous entry).’ We found the response rate and quality of their responses were remarkably high, as the majority of the emails were answered, and most all of the responses offered clear explanations of the reasons for the initial problematic order. Thus, this was found to be a fruitful source of information regarding reasons and details about reasons for errors in the original orders.
The leading cause of potential errors was found to be wrong patient errors, similar to findings in other studies using related methods such as so-called retract and reorder (RAR) triggers.6 RAR instances are cases when a provider orders a drug, cancels the order and then immediately places another order in another patient’s chart. Unlike RAR studies, however, our study directly solicited the clinicians’ exact reason(s) for why an erroneous drug order was discontinued. Numerous other reasons for erroneous prescriptions discontinued, such as confusing interface and look-alike/sound-alike issues, were also reported and are important from the quality improvement perspective and may require different types of interventions. Other frequent causes included wrong drug, wrong dose, duplicate order and wrong formulation.
Our method of information gathering from clinicians in near real time after an error or EHR issue occurred represents a potentially powerful method for improving clinical software or workflows, although it needs to be used parsimoniously to avoid further burdening busy clinicians. We were pleasantly surprised by the high response rate to the email queries, which we believe stems in part from our design that made responding easy, as well as allowing free text explanations that the research team coded. We recommend further exploration and use of such near-real-time feedback and learning as a helpful way to both engage clinicians and receive data to enable system learning and redesign.
It has been suggested that wrong patient errors may occur more often in CPOE systems than non-CPOE settings because of accidental selection of the wrong patient (eg, from pull-down menus of patient names), or features that allow prescribers to have multiple patients’ charts open simultaneously.3 6 To address the problem of wrong patient errors, our institution is now working on several research and improvement and research initiatives to these types of errors, including adding patient photographs as well as exploring ways the number of patients’ records open concurrently can influence the likelihood of wrong patient errors.
Many medications discontinued due to ‘Error (erroneous entry)’ in our prospective study were discontinued within a minute of the original order (7%), which we hypothesise (supported by a number of the free text comments) results in part from confusing CPOE interfaces. And even the ‘discontinued in error’ interface itself led to confusion, as some of the survey respondents provided a different reason for checking this box besides the original order being in error. Thus, organisations and prescribers need a better shared understanding of operational definitions for drug discontinuation checkbox reasons, and clearer indications of exactly what is going to be discontinued (eg, if two orders are duplicates, will one or both be discontinued). Ideally, such discontinuation reasons should be standardised across different commercial CPOE systems so that learning can be more easily and powerfully shared across systems. Even the nomenclature for this action is confusing and non-standardised, with some systems using, for example, ‘voided orders’ to similarly cancel and denote orders entered in error.10
In addition, CPOE and clinical decision support (CDS) developers should consider designing prompts for optional or required responses to capture details of the reasons when such a checkbox category is selected. Future work should also include analysis of time between placing a medication order and its discontinuation to gain a better temporal understanding of when errors are identified and how CPOE interfaces play a role. This type of real-time system for prescribers to enter a reason for the error could help better engage and empower them in uncovering problems and increase the ability to detect errors in the prescribing phase in a timelier way, contributing to organisational and vendor learning and improvement.
Although medication error observation studies typically identify the highest proportion of errors in the prescribing phase, in incident reporting systems, the majority of reported errors are reported in the administration phase.11 12 This suggests that prescribers may not have or take the time to report ordering errors, do not bother to report them since they are usually resolved before the medication reaches the patient, or may not realise that they have made an error. It is important to learn more about the most common types of errors that take place in the prescribing phase, as they may differ from those in other phases of the medication use process. In one study, our team previously found that the most common types of errors associated with CPOE found in incident reports were due to errors in the transmission of prescriptions, erroneous dosing and duplicate orders.3 Therefore, two of the three most common errors in the prescribing phase (wrong patient, wrong drug) in our study may not have been noted as most common through review of incident reports. While part of certification criteria for EHR technology in the US (Meaningful Use 2014) requires that vendors use user-centred design principles in developing their systems, the extent to which they do so is variable.13 Systems should be designed using these principles from the beginning, and it may also be valuable to perform studies such as this one to understand what has gone wrong and why in order to make iterative improvements in the applications.
Our study has several limitations. Despite the thousands of CPOE erroneous orders captured and documented with coded reasons at our institution, we suspect that such ‘erroneous’ orders are just the tip of a larger iceberg that our study methodology was not able to capture. Certainly, a clinician (either the same one who placed the order or a subsequent one caring for the patient) may not recognise an order as erroneous, which would preclude the error from being identified using the method described here. Also, as noted above, some of the ‘erroneous’ discontinuation orders were themselves erroneous checkbox errors (picking the wrong category of discontinuation reason). In addition, as we also previously mentioned, errors noted in the prescribing phase may differ from those found in other phases of the medication use process. This suggests the need for multiple methods to capture CPOE errors—something we have explored in other related studies in the CPOEMS project.14 Other limitations of our study include the good, but less than 100%, response rate and any biases this might introduce (eg, those committing more serious errors might be more or less willing to discuss them), the subjective nature of our classification of the events and that no formal reliability statistics were calculated for the pharmacists’ review of the email responses, the fact that the queries were generated only once every 24 hours, creating a lag and preventing prescribers from being able to recall the exact reason for the discontinuations, and the fact that in our legacy home-grown outpatient EHR system the default reason for discontinuing a medication was ‘No longer necessary,’ which may have led prescribers to accept this default as shortcut and thereby cause us to miss a potentially larger number of orders that were actually made in ‘Error (erroneous entry).’ Lastly, the study was performed at a single AMC using (at the time) a home-grown EHR that has since been replaced by a commercial EHR; thus, it may not be representative of other institutions, locales or vendors’ EHRs.
Conclusion
We found that for nearly 5% of drugs discontinued, prescribers indicate that the initial prescription was entered in error. While some prescribers, when asked about their discontinuation orders coded with this designation, were confused about the exact meaning of this coded field or mistaken in checking this reason-for-discontinuation checkbox, most responded with a range of useful reasons pointing to medication errors potentially facilitated by CPOE. Wrong patient and wrong drug errors were the leading reasons, but numerous other reasons were given (mostly related to dosage and form), each of which highlights an area for improved EHR and electronic CDS to ensure safer CPOE design and use. Approaches that take advantage of coded data routinely captured during drug discontinuation, thus, represent one promising source of information to help identify problems for such improvement in the future.
Footnotes
Contributors TTH and GS: responsible for writing and preparation of manuscript. GS, DWB and AW: responsible for study design. AS and MGA: responsible for review and categorisation of prospective study responses received. TTH, GS, DWB, AW, LAV, AS, MGA and AJLQ: responsible for critical review of the manuscript and data analysis. TTH and AJLQ: responsible for overall management and administrative aspects of this project, as well as management of data.
Competing interests None declared.
Ethics approval Partners Healthcare IRB.
Provenance and peer review Not commissioned; externally peer reviewed.