Article Text

Abstract
Objective To evaluate mortality differences between weekend and weekday emergency stroke admissions in England over time, and in particular, whether a reconfiguration of stroke services in Greater London was associated with a change in this mortality difference.
Design, setting and participants Risk-adjusted difference-in-difference time trend analysis using hospital administrative data. All emergency patients with stroke admitted to English hospitals from 1 January 2008 to 31 December 2014 were included.
Main outcomes Mortality difference between weekend and weekday emergency stroke admissions.
Results We identified 507 169 emergency stroke admissions: 26% of these occurred during the weekend. The 7-day in-hospital mortality difference between weekend and weekday admissions declined across England throughout the study period. In Greater London, where the reorganisation of stroke services took place, an adjusted 28% (relative risk (RR)=1.28, 95% CI 1.09 to 1.47) higher weekend/weekday 7-day mortality ratio in 2008 declined to a non-significant 9% higher risk (RR=1.09, 95% CI 0.91 to 1.32) in 2014. For the rest of England, a 15% (RR=1.15, 95% CI 1.09 to 1.22) higher weekend/weekday 7-day mortality ratio in 2008 declined to a non-significant 3% higher risk (RR=1.03, 95% CI 0.97 to 1.10) in 2014. During the same period, in Greater London an adjusted 12% (RR=1.12, 95% CI 1.00 to 1.26) weekend/weekday 30-day mortality ratio in 2008 slightly increased to 14% (RR=1.14, 95% CI 1.00 to 1.30); however, it was not significant. In the rest of England, an 11% (RR=1.11, 95% CI 1.07 to 1.15) higher weekend/weekday 30-day mortality ratio declined to a non-significant 4% higher risk (RR=1.04, 95% CI 0.99 to 1.09) in 2014. We found no statistically significant association between decreases in the weekend/weekday admissions difference in mortality and the centralisation of stroke services in Greater London.
Conclusions There was a steady reduction in weekend/weekday differences in mortality in stroke admissions across England. It appears statistically unrelated to the centralisation of stroke services in Greater London, and is consistent with an overall national focus on improving stroke services.
- health policy
- healthcare quality improvement
- quality improvement
Statistics from Altmetric.com
Introduction
Much attention has been paid in recent years to the association between weekend admissions and poor health outcomes following stroke. Several studies have investigated the impact of the day of admission on hospital mortality, reporting an increase in risk of death on weekends.1–5 Palmer et al observed higher 7-day in-hospital stroke mortality for weekend admissions in 2009/2010 when compared with weekday admissions (OR=1.18; 95% CI 1.12 to 1.24). Since that study, there have been major reforms in acute stroke services in England: the National Stroke Strategy (2007) was a major driver for improving stroke services.6 7 It stated that ‘people with suspected stroke should be immediately transferred to a hospital providing hyperacute services throughout the day and night—this included expert clinical assessment, rapid imaging and the ability to deliver intravenous thrombolysis’ and that ‘stroke networks should be established bringing together key stakeholders and providers to review, organise and improve delivery of services across the care pathway.’ This was a catalyst to review and improve services across the country.
In Greater London (a county and region in England which forms the administrative boundaries of London) and Manchester, this resulted in a move to a ‘hub-and-spoke’ model with patients with hyperacute stroke diverted by ambulance services to a smaller number of hyperacute stroke units (HASU). In London, any patient presenting with suspected stroke is now admitted to one of eight HASUs, which provide an immediate response to stroke 24 hours a day, 7 days a week. In Manchester, any patient presenting within 4 hours of developing stroke symptoms was admitted to comprehensive or primary stroke centres, although this was not a complete 24/7 service. Patients presenting outside the 4-hour window would be admitted to the nearest local stroke centre, as was done before reconfiguration.7 The changes to services in Greater London and Manchester were implemented in July and April 2010, respectively. If the weekend effect found previously1 is due to poorer quality of care at the weekend, and given the more complete reorganisation of services in London to provide better 24/7 care, then stroke care is uniquely positioned to shed light on changes in weekend mortality over time, and on the impact of large-scale service reorganisation.
Recent research8 9 has reported that the centralisation of acute stroke service in both areas was associated with better health outcomes. In other parts of the country, different regional approaches were taken, with more focus on improvement in all units, or more small-scale consolidation of local services. Furthermore, some studies showed that the reorganisation of stroke services may overcome the ‘weekend effect’.10 11 We defined the ‘weekend effect’ as differences in patient outcomes between weekend and weekday hospital admissions. We aimed to estimate whether there had been a change in the weekend/weekday in-hospital mortality ratio in Greater London following reconfiguration of services in comparison with the rest of the country. As changes in Manchester were less radical, we incorporated these in the rest of England in the baseline analysis but performed sensitivity analyses to assess whether exclusion changed the results.
Methods
Study design and setting
We extracted patient-level data from national routinely collected administrative data (Hospital Episode Statistics or HES) from 1 January 2008 to 31 December 2014. Records include information of all admissions to English National Health Service (NHS) hospital trusts. Each patient record contains information on demographics (eg, sex, age and ethnicity), the episode of care (eg, trust name, date of admission) and diagnosis.12 Diagnoses are recorded using the International Classification of Diseases, 10th edition (ICD-10). Each patient episode was linked into ‘spells’ (admissions to one provider) and spells were linked into ‘superspells’, the latter combining any interhospital transfers.
Our study covers a 30-month period before (January 2008 to June 2010) the reorganisation of stroke service in Greater London, and a 54-month period afterwards (July 2010 to December 2014). All admissions during the same period in the rest of England were used as controls.
Participants and outcomes
The main outcome of interest was the difference in all-cause mortality between weekend and weekday admissions (7-day and 30-day). We identified emergency stroke admissions using a primary diagnosis field in the first episode recorded as intracerebral haemorrhage (I61) or cerebral infarction (I63), or stroke, not specified as haemorrhage or infarction (I64). If the primary diagnosis in the first episode was recorded as symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified (R00–R99), we used the primary diagnosis field in the second episode. The weekend was defined as the period from midnight on Friday to midnight on Sunday and the rest as weekdays (time of admission is not collected in HES).
Statistical analyses
We carried out a descriptive analysis of our population, separating them based on the weekend/weekday, pre/postcentralisation and by area (Greater London and the rest of England). The crude risk, adjusted relative risk (RR) and 95% CIs by financial years, and before and after centralisation were estimated using logistic regression.13–15 Based on the literature and data available, we included the following patient-level variables in the logistic regression model: age (measured in 6-year bands), sex, ethnic group, small-area socioeconomic deprivation (Carstairs quintile),16 comorbidities (Charlson score, NHS adaptation),17 number of previous admissions, month of discharge, source of admission and stroke subtype.
We used a difference-in-difference approach to examine whether the reconfiguration of stroke services in Greater London was associated with a change in the mortality difference between weekend and weekday emergency stroke admissions over time compared with the changes over time in the rest of England. This statistical approach is often used to assess the changes that occur following a natural experiment or the implementation of healthcare policy.8 18–20 The difference-in-difference approach has a key assumption known as parallel trends. It states that the trends in outcome of interest are the same before the policy was implemented between the treated and comparison groups.18
First, logistic regression models (adjusted for patient-level variables described above) were fitted using the data for all England before the reorganisation and the estimated coefficients were used to predict the probability of in-hospital mortality for each patient (pre/postreorganisation). Then these were aggregated to create a data set of the observed and the expected number of deaths in hospital by quarter, weekend/weekday and area (Greater London and the rest of England). The adjusted in-hospital mortality rate was calculated as:

where O is the number of observed deaths, E is the number of expected deaths, and NCR is the in-hospital mortality national crude rate before reorganisation (number of deaths/number of admissions). The assumption that the trend for adjusted in-hospital mortality difference between weekend and weekday admissions was the same in Greater London and in the rest of England (the parallel trends assumption) was tested by examining the precentralisation trends in both groups (online supplementary figure 1) and by assessing the significance of the interaction term between time and area using a regression model. In our model, the interaction term between time and area was not significant which justified the parallel trends assumption.
Supplementary file 1
Whether the change in the difference between weekend and weekday admissions was associated with reorganisation was tested using a regression framework:

In this equation, time is a variable of time and covers the 28 time periods (quarters), area is a dummy variable for region (1 if Greater London, 0 if the rest of England), and policy refers to the introduction of centralisation (0 precentralisation; 1 postcentralisation). The interaction term area×policy indicates if the effect of the area on the mortality difference between weekend and weekday admissions differs depending on the policy, for example, if the interaction term is significant (p≤0.05), then the centralisation of stroke services in Greater London is associated with a different effect on the mortality difference between weekend and weekday admissions. Each observation in the regression model was weighted by the number of hospital admissions in each quarter. By examining the correlation between time and the difference in rates, the linear time trend assumption was assessed and found to be valid.
In Greater London, the implementation process was carried out in the following steps: service development (October 2009 to July 2010), launch of full system (July 2010) and opening of final HASU/closure of interim HASU (October 2011).5 A sensitivity analysis was conducted with the different time points of the introduction of centralisation: October 2009 (precentralisation period: January 2008 to September 2009 and postcentralisation period: October 2009 to December 2014) and October 2011 (precentralisation period: January 2008 to September 2011 and postcentralisation period: October 2011 to December 2014).
There are over 60 hospitals in Greater London. Before the centralisation, 30 hospitals provided acute stoke care. From July 2010, eight hospitals in Greater London were designated as HASUs. Online supplementary figure 2 shows how the number of hospital admissions in HASUs changed over the study period. An additional analysis was done to evaluate the impact of the reorganisation in these hospitals on the mortality difference between weekend and weekday admissions. Using the same approach as described above, we estimated crude risk, adjusted RR and 95% CIs before and after centralisation. The difference-in-difference approach was used to examine whether the reconfiguration of stroke services in these eight hospitals was associated with a change in the mortality difference between weekend and weekday admissions over time compared with the changes over time in the rest of England (excluding the rest of the hospitals in Greater London). The stroke care service centralisation was implemented in Greater London and Manchester using different approaches and in the latter region the changes were less radical.21 As a sensitivity analysis, we excluded Greater Manchester from the rest of England and repeated our analysis. A p value <0.05 was considered statistically significant, and all analyses were carried out with SAS V.9.4 software package (SAS Institute).
Patient involvement
We have run two focus group consultations with groups of patients and members of the public since December 2014 to discuss the patient-level records we hold and the research we use them for.
Results
We identified 507 169 emergency stroke admissions from January 2008 to the end of 2014. Almost 26% (130 200) of these admissions occurred during the weekend (table 1). Patients in Greater London were slightly younger, more likely to be male and less likely to be white or admitted from home compared with the rest of England. The proportion of intracerebral haemorrhage stroke (I61) was slightly higher in Greater London. Weekend patients were slightly older, more likely to be female and be presenting with intracerebral haemorrhage stroke. Unadjusted risk for in-hospital mortality remained lower in Greater London than the rest of England throughout the study period.
Characteristics of the study population before and after service reconfiguration in Greater London and the rest of England
During the study period, 7-day and 30-day in-hospital mortality in England was 8.8% and 16.5%, respectively. It was significantly higher for patients admitted during weekends than during weekdays (7-day: 9.7% vs 8.4%, p<0.001; 30-day: 17.9% vs 15.9%, p<0.001). Simple before-and-after comparisons show that after the reorganisation of stroke services in Greater London, a 14% (adjusted RR=1.14, 95% CI 1.03 to 1.26) higher weekend/weekday 7-day mortality ratio declined to 6% (adjusted RR=1.06, 95% CI 0.98 to 1.16) (table 2). In London HASUs, an even higher reduction in the RR was observed, declining from 14% (adjusted RR=1.14, 95% CI 0.99 to 1.32) higher weekend/weekday 7-day mortality ratio to 4% (adjusted RR=1.04, 95% CI 0.93 to 1.15). For the rest of England, a 14% (adjusted RR=1.14, 95% CI 1.11 to 1.18) higher weekend/weekday 7-day mortality ratio declined to 12% (adjusted RR=1.12, 95% CI 1.09 to 1.16). During the same period, in Greater London a 12% (adjusted RR=1.12, 95% CI 1.10 to 1.14) higher weekend/weekday 30-day mortality ratio declined to 10% (adjusted RR=1.10, 95% CI 1.04 to 1.17). For the rest of England, a 10% (adjusted RR=1.10, 95% CI 1.07 to 1.13) higher weekend/weekday mortality ratio increased to 12% (adjusted RR=1.12, 95% CI 1.03 to 1.20).
Unadjusted/adjusted RRs and its 95% CIs before and after centralisation
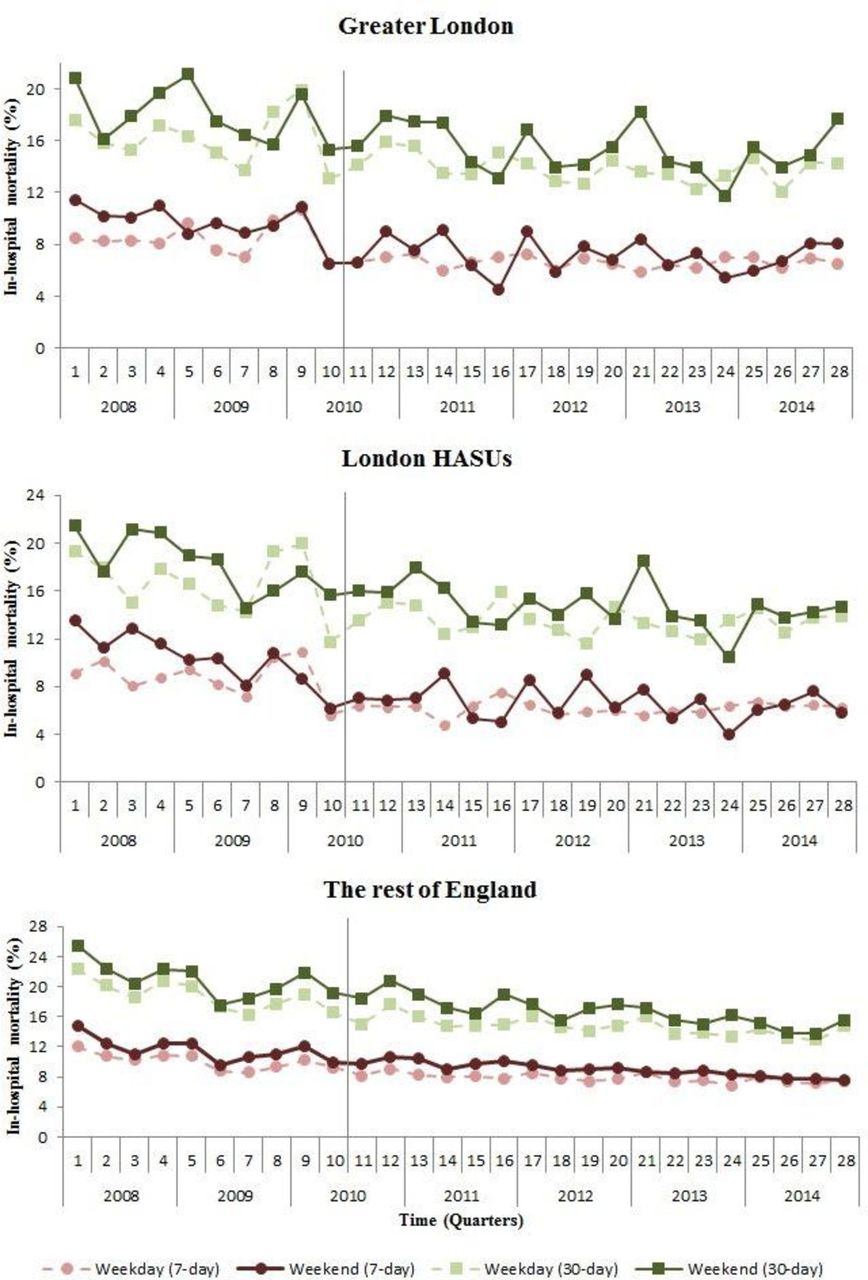
The trends presented in figure 1 show that 7-day and 30-day in-hospital mortality was declining throughout the study period for weekend and weekday admissions in Greater London and in the rest of England. Similar patterns in trends were observed after adjusting for age, sex, ethnic group, small-area socioeconomic deprivation, comorbidities, number of previous admissions, month of discharge, source of admission and stroke diagnosis (figure 2). In Greater London, an adjusted 28% (RR=1.28, 95% CI 1.09 to 1.47) higher weekend/weekday 7-day mortality ratio in 2008 declined to a non-significant 9% higher risk (RR=1.09, 95% CI 0.91 to 1.32) in 2014. For the rest of England, a 15% (RR=1.15, 95% CI 1.09 to 1.22) higher weekend/weekday 7-day mortality ratio in 2008 declined to a non-significant 3% higher risk (RR=1.03, 95% CI 0.97 to 1.10) in 2014. During the same period, in Greater London an adjusted 12% (RR=1.12, 95% CI 1.00 to 1.26) weekend/weekday 30-day mortality ratio in 2008 increased to 14% (RR=1.14, 95% CI 1.00 to 1.30); however, this was not significant. In the rest of England, an 11% (RR=1.11, 95% CI 1.07 to 1.15) higher weekend/weekday 30-day mortality ratio declined to a non-significant 4% higher risk (RR=1.04, 95% CI 0.99 to 1.09) in 2014.

Crude 7-day and 30-day in-hospital mortality rate change in Greater London, London HASUs and the rest of England by quarters (vertical grey line represents the time moment when stroke services were centralised in Greater London). HASU, hyperacute stroke unit.

{kind=link}
{kind=link}
(A) 7-day and (B) 30-day in-hospital mortality relative risk with 95% CI in Greater London, London HASUs and in the rest of England by year. HASU, hyperacute stroke unit.
Table 3 represents results of a difference-in-difference analysis (parameter estimates, standard errors and p values). The time coefficient is significant and negative in both models, indicating that the mortality difference between weekend and weekday admissions was trending downwards to a statistically significant degree. The parameter estimate for area×policy is the main coefficient of interest. It shows whether the centralisation of stroke service in Greater London may have been associated with a different change in weekend/weekday mortality difference. In both models, the coefficient for area×policy is not significant (p>0.05), indicating that the decline in weekend/weekday mortality difference in Greater London was not significantly different compared with the rest of England. Almost 70% of all emergency hospital admissions had cerebral infarction as a primary diagnosis (data not shown). We repeated the difference-in-difference analysis including only these admissions and obtained similar results. Sensitivity analysis showed that excluding Manchester (another region where services had been reorganised) from the analysis did not change the results (online supplementary table 1). Furthermore, choosing different time points of the centralisation of stroke services in Greater London showed comparable results (online supplementary figure 2 and supplementary tables 2 and 3).
Results of the regression analysis assessing the effect of time, area and policy on the mortality difference between weekend and weekday admissions for 7-day and 30-day in-hospital mortality
Discussion
Across England, the higher 7-day and 30-day in-hospital mortality risk associated with patients with stroke admitted during weekends compared with weekdays declined during the study period, to the extent that it is no longer statistically significant in the most recent year (2014) (figure 2). In Greater London, an adjusted 28% (RR=1.28, 95% CI 1.09 to 1.47) higher weekend/weekday 7-day mortality ratio in 2008 declined to a non-significant 9% higher risk (RR=1.09, 95% CI 0.91 to 1.32) in 2014. For the rest of England, a 15% (RR=1.15, 95% CI 1.09 to 1.22) higher weekend/weekday 7-day mortality ratio in 2008 declined to a non-significant 3% higher risk (RR=1.03, 95% CI 0.97 to 1.10) in 2014. During the same period, in Greater London an adjusted 12% (RR=1.12, 95% CI 1.00 to 1.26) weekend/weekday 30-day mortality ratio in 2008 slightly increased to 14% (RR=1.14, 95% CI 1.00 to 1.30); however, it was not significant. In the rest of England, an 11% (RR=1.11, 95% CI 1.07 to 1.15) higher weekend/weekday 30-day mortality ratio declined to a non-significant 4% higher risk (RR=1.04, 95% CI 0.99 to 1.09) in 2014. We found no statistically significant association between the decreasing mortality difference between weekend/weekday admissions and the centralisation of stroke service in Greater London.
Previous studies showed that stroke centres with 24 hours a day, 7 days a week access to stroke specialists and necessary medical care may overcome the ‘weekend effect’. Albright et al 22 23 found no statistically significant difference in hospital mortality between weekend and weekday admissions when examining comprehensive stroke centres (CSC) in the USA. In their study23 of eight different CSCs, there were no significant differences in in-hospital mortality found for patients with ischaemic stroke admitted during weekends compared with weekdays. Another study in the USA analysed whether the change in mortality between weekend and weekday admissions was associated with stroke centre designation in the state of New Jersey.11 The study included 134 441 patients with cerebral infarction admitted to hospitals between 1996 and 2007, and a significant reduction in 90-day risk of death (HR=0.86; 95% CI 0.82 to 0.91) was observed during the time when stroke centres were designated.
Several studies in the UK8 24 investigated whether the centralisation of stroke services was associated with changes in mortality and better quality of care. Morris et al 8 found a significant larger decline in risk-adjusted mortality at 3, 30 and 90 days in London compared with the rest of England. Ramsay et al 24 observed that after centralisation, patients admitted to hyperacute units were significantly more likely to receive clinical intervention than patients admitted to non-hyperacute units. A population-based study in Dijon (France)10 reported that the higher risk of 30-day all-cause mortality in patients admitted during weekends or bank holidays (HR=1.26, 95% CI 1.06 to 1.51) disappeared after the implementation of a stroke unit (HR=0.99, 95% CI 0.69 to 1.43). A recent study based on clinical audit data in the UK3 found there was no difference in 30-day survival between weekends and weekdays in 2013/2014 data. This, together with the two other UK studies,1 4 is consistent with our findings. We found no statistically significant association between the declining mortality difference between weekend/weekday admissions and the centralisation of stroke services in Greater London compared with the rest of England. Our study covers a time period twice as long after the change than in Morris el al 8 (54 months vs 21 months). After centralisation, patients presenting with suspected stroke should be transferred to HASUs for treatment and assessment. However, not all London patients in our data set were admitted to HASUs (online supplementary figure 2). This may reflect a significant proportion of complex elderly patients, whose stroke is incidental to other conditions and/or they may have a significantly different risk profile. It is likely, given the apparent success of specialised stroke units25 and a huge focus on service improvement in stroke services across the rest of England,26 27 that any apparent benefits to the London reconfiguration have been eclipsed.
Turner et al 21 stated that ‘While services were more fully centralized in London, a less radical transformation of services took place in Manchester… In Manchester, the original model in which patients would be eligible for HASU care within 24 hours from onset of symptoms was revised so as to maintain consensus, such that only patients presenting within 4 hour of developing symptoms were eligible for treatment in a HASU and no provider lost their stroke services.’ Morris et al 8 found that in Greater Manchester the changes in mortality after the reconfiguration of services were not significantly different from the changes seen in the rest of England during the same period. Furthermore, Ramsay et al 9 showed that fewer patients with stroke were admitted to HASU in Greater Manchester (39%) compared with Greater London (93%). Following this, we expect that we would not find a significant association between the decrease in the mortality difference between weekend/weekday admissions and the centralisation of stroke service in Greater Manchester.
The main strength of this study is the use of national data which cover all hospital admissions and contain information on outcomes and patient characteristics. Another strength is the use of a difference-in-difference approach. Figure 1 shows that in-hospital mortality was declining across England even before reorganisation of stroke services in Greater Manchester and London. This suggests that the quality of care received by patients with stroke was improving before reorganisation, making a simple before-after analysis potentially misleading. The difference-in-difference approach overcomes this issue by using a comparison group, in our case the rest of England, that is experiencing the same trends in the outcome but is not exposed to the change in policy.
However, there are a few limitations. First, stroke severity, which is an important predictor of mortality,28 is not recorded in the HES data set. There may be changes in casemix that are not being reflected in our analysis, although changes in resident population casemix over time, which would have to occur specifically at weekends, would seem unlikely to account for our findings. Our results are consistent with two recent UK papers3 4 which were both able to account for stroke severity. The first paper looking at Stroke Improvement National Audit Programme (SINAP) data for 2011–2012 found a borderline weekend effect, and the second more recent paper looking at more recent data (2013–2014) found no significant weekend effect. Second, our definition of time of admission does not allow us to identify whether in-hospital mortality was higher for the off-hours period during weekdays. Ogbu et al 29 observed a higher 7-day case-fatality odds for patients admitted during weekday nights, and more recently Bray et al 3 identified different patterns and magnitudes of temporal variation in the delivery of care, including off-hours and night-time care. Another study30 has sought to ascribe data quality as an explanation for the weekend effect, but the study was based on a small number (n=9) of general practitioner practices in Oxford and may simply reflect local practices. In addition, much of the alleged incorrect coding appeared to be due to the inclusion in the study of coded elective cases, and a much wider selection of diagnosis codes (I60–I68), which included non-stroke diagnoses. A sensitivity analysis failed to take into account the combined effect of these biases. We have restricted our analysis to non-elective admissions and stroke-specific ICD-10 codes, making coding issues a less likely explanation for the observed reduction in weekend/weekday differences in our study.
Conclusions
While other research has suggested that centralisation of stroke care in London is associated with better outcomes generally, we in addition observe a gradual reduction in the weekend effect for emergency stroke admissions across England between 2008 and 2014. Although we cannot rule out an effect from centralisation, we found no statistical association with the reorganisation of services in London. This is unlikely to be due to changes in casemix or coding, and is consistent with a more general pattern of service improvement across the country with increased specialisation, as well as improved 24/7 delivery of care. While we have not specifically looked at staffing levels, it has not escaped our notice that our observed reductions in the ‘weekend effect’ occurred before any contractual changes for medical staffing in the UK.31
Acknowledgments
This work uses data provided by patients and collected by the NHS as part of their care and support.
References
Footnotes
Handling editor Kaveh G Shojania
Contributors All authors contributed to the original research proposal. PPA was instrumental in securing the data. All authors helped refine the classification of outcomes used and the procedure groups for further analysis. PPA, AB and VB carried out the analysis. PPA, AB and VB wrote the first draft. All authors commented on subsequent drafts of the manuscript.
Funding The Dr Foster Unit is an academic unit in the Department of Primary Care and Public Health, within the School of Public Health, Imperial College London. The unit receives research funding from the National Institute of Health Research and Dr Foster Intelligence, an independent health service research organisation (a wholly owned subsidiary of Telstra). The Dr Foster Unit at Imperial is affiliated with the National Institute of Health Research (NIHR) Imperial Patient Safety Translational Research Centre. The NIHR Imperial Patient Safety Translational Centre is a partnership between the Imperial College Healthcare NHS Trust and Imperial College London. The Department of Primary Care & Public Health at Imperial College London is grateful for support from the NW London NIHR Collaboration for Leadership in Applied Health Research & Care (CLAHRC) and the Imperial NIHR Biomedical Research Centre.
Competing interests None declared.
Ethics approval The principal investigator has approval from the Secretary of State and the Health Research Authority under Regulation 5 of the Health Service (Control of Patient Information) Regulations 2002 to hold confidential data and analyse them for research purposes (CAG ref 15/CAG/0005). We have approval to use them for research and measuring quality of delivery of healthcare, from the London - South East Ethics Committee (REC ref 15/LO/0824).
Provenance and peer review Not commissioned; externally peer reviewed.