Article Text

Abstract
Background Hospitalised patients whose inpatient teams rotate off service experience increased mortality related to end-of-rotation care transitions, yet standardised handoff practices are lacking.
Objective Develop and implement a multidisciplinary patient-centred handoff intervention to improve outcomes for patients who are critically ill during end-of-rotation transitions.
Design, setting and participants Single-centre, controlled pilot study of medical intensive care unit (ICU) patients whose resident team was undergoing end-of-rotation transition at a university hospital from June 2017 to February 2018.
Intervention A 4-item intervention was implemented over two study periods. Intervention 1 included: (1) in-person bedside handoff between teams rotating off and on service, (2) handoff checklist, (3) nursing involvement in handoff, and (4) 30 min education session. Intervention 2 included the additional option to conduct bedside handoff via videoconferencing.
Main outcome measures Implementation was measured by repeated clinician surveys and direct observation. Patient outcomes included length of stay (LOS; ICU and hospital) and mortality (ICU, hospital and 30 days). Clinician perceptions were modelled over time using per cent positive responses in logistic regression. Patient outcomes were compared with matched control ‘transition’ patients from 1 year prior to implementation of the intervention.
Results Among 270 transition patients, 46.3% were female with a mean age of 55.9 years. Mechanical ventilation (64.1%) and in-hospital death (27.6%) rates were prevalent. Despite high implementation rates—handoff participation (93.8%), checklist utilisation (75.0%), videoconferencing (62.5%), nursing involvement (75.0%)—the intervention did not significantly improve LOS or mortality. Multidisciplinary survey data revealed significant improvement in acceptability by nursing staff, while satisfaction significantly declined for resident physicians.
Conclusions In this controlled pilot study, a structured ICU end-of-rotation care transition strategy was feasible to implement with high fidelity. While mortality and LOS were not affected in a pilot study with limited power, the pragmatic strategy of this intervention holds promise for future trials.
- hand-off
- transitions in care
- patient safety
- critical care
- checklists
Statistics from Altmetric.com
Introduction
Medical errors resulting in patient harm are a leading cause of death among Americans,1 2 and are an increasingly recognised result of miscommunication during transitions of care.3–11 However, increasing restrictions to resident work hours mean patient handoffs have increased12 and continuity of care may be compromised.13 Adverse events associated with shift handoffs, during which a physician transfers care of a patient to another physician for a brief amount of time, such as with overnight coverage, are well documented.3–6 8 9 14–16 Similarly, patients transitioning between locations17 18 or to home from the hospital may be at risk related to ineffective handoffs.19–21 Evidence-based practices targeting these handoffs have been developed that may improve both communication and patient outcomes.4 5 22–25
However, the effects of end-of-rotation or ‘service’ transitions in care may be equally detrimental to patient care but have received substantially less attention.10 26 27 During this transition, one physician permanently transfers the care of an entire list of patients to another physician. Unlike shift handoffs, times at which the original physician resumes care, service transition is permanent—the clinician signing out has no further contact with these patients or their new care team. While early studies suggested patients affected by these transitions experience increased length of stay (LOS) and cost,28 29 rigorous large-scale studies have suggested a significant increase in mortality in patients exposed to these transitions.10 11 Unfortunately, this specific and substantial transition has not been investigated in the critically ill—a population often considered one of the most vulnerable to medical errors. Organised structure facilitates care in the intensive care unit (ICU), and recent work found that a structured ICU-specific handoff template may improve perceived outcomes during resident shift handoff at night,24 but interventions aimed at service handoff have not been tested.
Given the lack of standardisation regarding this critical transition of care, we developed and implemented a multidisciplinary patient-centred handoff intervention aimed at improving patient outcomes.
Methods
Study design, setting and participant characteristics
This was a single-centre, controlled pilot study of adult medical patients exposed to end-of-rotation resident transitions in care in the medical ICU (MICU) at a large, academic, quaternary referral hospital. The Standards for Quality Improvement Reporting Excellence 2.0 guidelines were followed in reporting this manuscript.30 The MICU is a ‘closed unit’ (patients in the ICU are covered by four distinct ICU resident physician teams made up of one resident and one intern per team dedicated to care of the ICU only on call every fourth day) with resident teams rotating onto or off service every 28 days at the same time. Prior to this study, residents and interns performed end-of-rotation handoff individually (resident to resident and intern to intern) by required written email communication and occasional verbal handoff but never at the bedside. The MICU is staffed with two attending physicians who rotate on a 1 or 2-week cycle and one fellow per month. MICU attending and fellow handoff techniques vary, but involved an email and/or phone call. The average daily census is between 5 and 10 patients per resident team. One attending physician is assigned to round with two of the four resident teams daily. Each patient in this study is one that was exposed to an ICU service transition. Each one of these patients (whether control or intervention) was included if he or she was currently present on a MICU team at 07:00 on day 1 of each 28-day resident rotation. This is the time when house staff started new rotations, and therefore, the new team would be accepting this entire list of patients from the last team of house staff going off service. The intervention patients were those present at 07:00 on service transition days during the current year of the study. The control patients were those present at 07:00 on service transition days from the same month but during the prior year (when there was no study taking place). These patients were included in one of four groups: control 1, control 2, intervention 1 and intervention 2. Intervention 1 included patients from September through November 2017 while intervention 2 included patients from December 2017 through February 2018. Controls 1 and 2 included patients from the same time frame a year prior (September 2016 to February 2017) for comparison. Patients experiencing more than one ICU transition were included in the transition group initially assigned for all analyses. Similarly, subsequent admissions did not alter the original group classification.
Intervention
The intervention was developed using previously published data on care transitions4 5 31–33 and informed by three resident and nursing focus groups conducted before the study period aimed at determining current practice patterns and expected limitations. The intervention included four separate components aimed to be patient centred, multidisciplinary and pragmatic: (1) in-person bedside handoff (including patient/family if possible), (2) bedside handoff checklist, (3) nursing presence at handoffs, and (4) 30 min education sessions for residents instructing them in the new process. In-person bedside handoff took the form of a structured interaction at the patient’s bedside with the nurse present using a checklist to ensure completeness of handoff for each patient. The checklist used for bedside handoff (online supplementary material 1) was adapted for an ICU setting from a prior publication using a similar checklist to transition care at the end of the house staff rotation.32 One novel component, termed the ‘diagnostic certainty score’, was included in this checklist. The aim of the diagnostic certainty score was to address the potential for anchor bias in verbal communication by recognition at the onset of handoff communication. Residents were asked to start their verbal handoff with an estimation of how confident they were in the accuracy of diagnosis for the transitioning patient. Depending on the level of diagnostic certainty, the receiver might comprehend information differently. To accommodate scheduling logistics, flexibility was incorporated in handoff timing and written communication was simplified so the verbal handoff was minimally duplicative with any written documentation. The written component of handoff was already being used in this ICU by means of a standard electronic medical record (EMR)-embedded handoff template, a separate written email and an ‘end-of-rotation’ progress note. We simplified this component of the handoff process to only use the already in place EMR-embedded template that was to be copied and securely emailed ahead of transition between residents. This template included standard free-text components of a written sign-out (ie, patient name, medical history, current diagnoses, procedures, medications, 24 hours’ events, to do’s, consulting services). The final component of the intervention was an education session which occurred on Thursday mornings before each rotation at a scheduled time given by study personnel (JLD, JK). The contents of this session included a brief presentation on prior evidence, presentation of expectations, introduction to checklists and expected questions/concerns.
Supplemental material
Intervention 1 began its first study period in September 2017 and was implemented for three consecutive 28-day rotations. Feedback and observations during the initial period revealed concerns regarding the scheduling logistics (poor satisfaction with timing/ability to actually hand off in person) and education of house staff (written communication declined due to misunderstanding by residents). Intervention 2 addressed these limitations in two ways. First, emphasis was added during the education session to continue written communication in addition to bedside handoff. Second, to improve satisfaction with in-person handoff logistics, a prespecified option to videoconference at the patient’s bedside was implemented during intervention 2. The videoconferencing occurred via FaceTime34 on a secure wireless network and again included the patient, resident physicians rotating on and off service and the bedside nurse. Participation was voluntary and no incentives were given to individuals involved at any part of the study as per regulations of the funding source.
Data collection, study cohorts and outcome measures
Implementation was measured using direct observation data. Direct observations of bedside handoff by research personnel (without deliberate interference) took place each rotation after the initiation of intervention 1 for data collection about intervention and checklist adherence characteristics. Acceptability, perceived efficacy and balancing metrics of participants (including attending physicians, nurses and residents) were measured by serial surveys with anonymous responses. Surveys were administered monthly to internal medicine residents at the beginning of each rotation following service change via in-person and email administration, while attending and nursing surveys were administered at three occurrences to entire staff: baseline, following intervention 1 and at completion of intervention 2. All survey questions were developed using prior publications on transitions in care31–33 35 36 and tested using an iterative review process with local stakeholders, institutional survey design experts and non-study clinicians (online supplementary material 2). For all resident, nurse and attending surveys, per cent positive response (agreement) was created from collapsing other categories. Depending on the question, per cent positive response was defined as either strongly agreeing/agreeing or always/often/sometimes, while negative responses were defined as disagreeing/strongly disagreeing or rarely/never.
Supplemental material
Patient demographic and outcome data were collected for all patients who met inclusion criteria. Patient data were collected using Health Data Compass, an enterprise health data warehouse that integrates patient clinical data from the EMR and the state-wide All Payer’s Claims Database (APCD) from the Center for Improving Value in Health Care, and managed using the electronic data capture tool Research Electronic Data Capture.37
Patient data included: age, sex, race, ethnicity, hospital admission date, ICU admission date, discharge date, all comorbidities indexed by International Classification of Diseases, Tenth Revision, Clinical Modification codes, hospital death, state resident status, state death status (only for in-state residents collected from APCD to determine 30-day mortality) and the Acute Physiology and Chronic Health Evaluation (APACHE) II38 score components. Comorbidities were used to construct the Charlson Comorbidity Index, which has been associated with the risk of hospital death.39 40 Clinical outcomes included LOS (hospital and ICU) and mortality (hospital, ICU and 30 days). A power analysis was not performed for this pilot trial.
Statistical analysis
Descriptive statistics were used to compare patient and clinician characteristics in both control and intervention periods and to summarise clinicians’ adherence to the intervention. Differences in handoff and checklist direct observation characteristics were tested between intervention periods 1 and 2 with two-proportion Z-tests. In transition interventions 1 and 2, mortality was modelled between control and intervention periods with unadjusted and adjusted logistic regressions, and LOS was modelled between control and intervention periods with unadjusted and adjusted linear regressions. Adjusted models accounted for age, sex, race/ethnicity, mechanical ventilation required, APACHE II score and Charlson Comorbidity Index. Mean (SD) and linear regressions were used for summarising and modelling LOS since the sample size was sufficiently large. Two sensitivity analyses were considered for LOS models to exclude outliers over 50 days or over 30 days, but the results were unchanged, so the results presented include all LOS data.
Results
Study populations
The study included 270 ICU patients exposed to end-of-rotation transitions of care (table 1). Among them, 46.3% were women with a mean age of 55.9 years. Ventilatory support was required for 173 (64.1%) individuals while mean APACHE II and Charlson Comorbidity Index scores were 20.4 and 15.0, respectively. Notably, all 270 study patients were exposed to end-of-rotation transition, and the overall mortality was high with 73 (27.0%) patients expiring in the hospital and 55 (20.3%) expiring in the ICU. Among 318 ICU clinicians surveyed, response rates were 58/64 (90%) for residents, 109/197 (55%) for nurses and 28/57 (49%) for attendings. As outlined in table 1, demographic characteristics for patients and clinicians were similar between groups.
Patient and clinician characteristics
Intervention adherence and implementation
During the baseline observation period reported in table 2, resident reported written sign-out communication was reliably completed (95.5%) with variable in-person handoff completion (50.0%) and rare nursing involvement (13.6%). Following the onset of intervention 1, implementation of the transition bundle components increased: bedside handoff participation (85.0%), checklist utilisation (70.0%), nursing involvement (60.0%); however, a decline in written sign-out communication (30.0%) was noted. With the onset of intervention 2, improved adherence was noted: bedside handoff participation (93.8%), checklist utilisation (75.0%), bedside videoconferencing (62.5%), nursing involvement (75.0%) and written sign-out communication (68.8%).
Clinician adherence to intervention
Table 3 portrays the individual patient handoff observations (n=136) completed during the first and second intervention periods. Observations revealed the frequency of nursing involvement and patient/family involvement in bedside handoff improved significantly from intervention 1 to intervention 2 (53.4% to 71.4%, p=0.04; 48.1% to 81.0%, p<0.001, respectively). Direct observation data validated resident respondent data—similar levels of frequency for bedside handoff participation and checklist utilisation (93.4% and 83.8%, respectively). Using direct observational data, in-person handoff took an average of 39 min (±13.6 min) to round on 5.4 patients (±2.0 patients). All checklist components were used frequently (>75%) including the diagnostic certainty score which was used often (73.5%).
Handoff and checklist direct observation*
Clinician acceptability
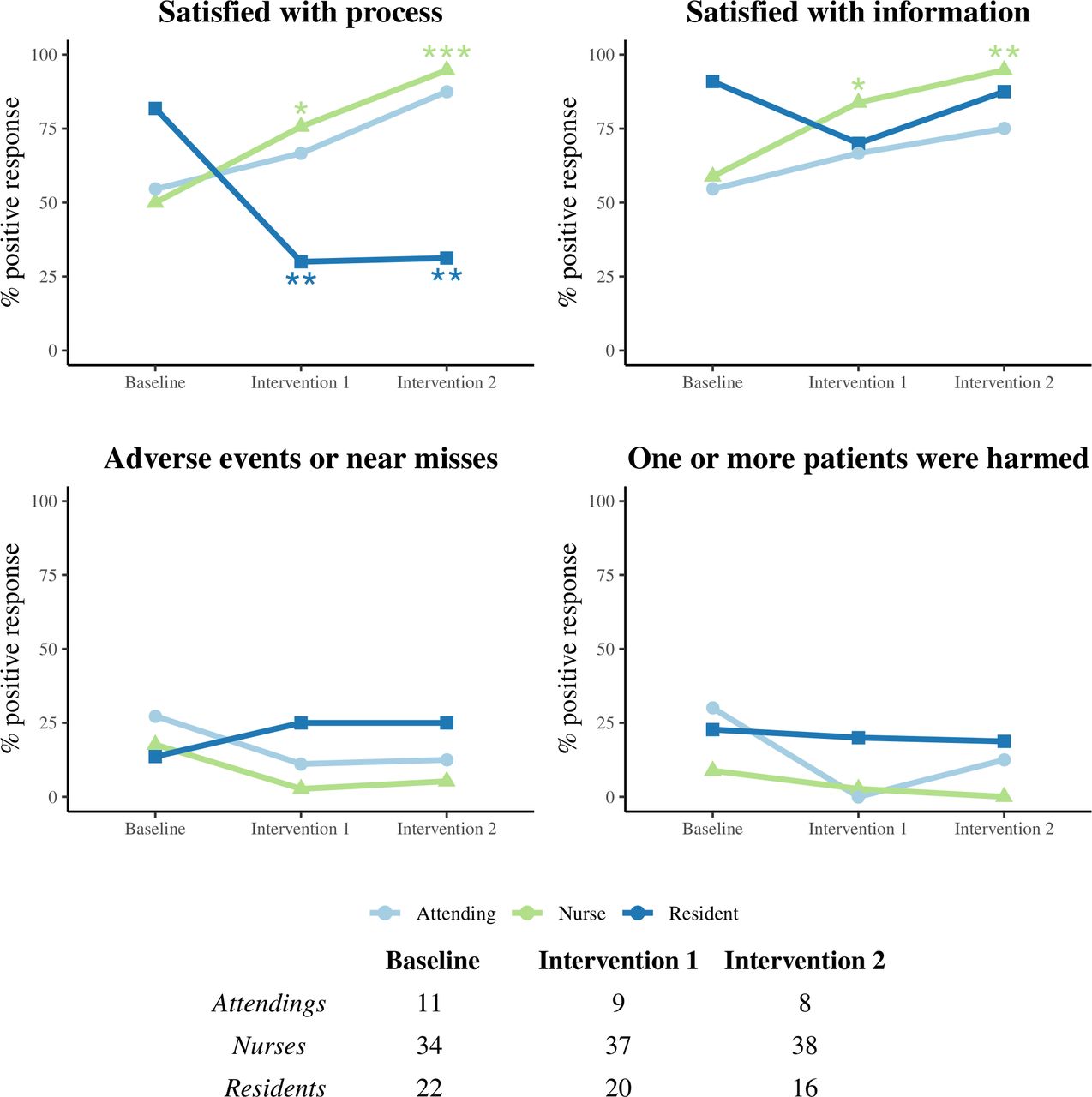
As shown in figure 1, nursing staff experienced significantly increased satisfaction with the multidisciplinary transition intervention (both the transition process and the information exchange), but did not perceive a significant change in patient harm or adverse events/near misses. Attending physicians expressed similar satisfaction, but these results were not statistically significant. In contrast, resident satisfaction with the transition process and information exchange significantly decreased after intervention implementation, and had similar rates of perception of change in patient harm or adverse events/near misses as attendings and nurses.
{kind=link}
Intensive care unit (ICU) clinician acceptability and perceptions over time. Repeated questionnaires were administered to ICU residents, attendings and nurses throughout the entire study. Per cent positive response (agreement) was created from collapsing other categories. Depending on the question, per cent positive response was defined as either strongly agreeing/agreeing or always/often/sometimes, while negative responses were defined as disagreeing/strongly disagreeing or rarely/never. The table summarises the number of responses by group at each time point. Intervention 1 and intervention 2 survey data were compared with baseline data, respectively. *p<0.05; **p<0.01; ***p<0.001.
Length of stay and mortality
As shown in table 4, mean hospital LOS was not significantly different for intervention patients as compared with controls for both intervention 1 and intervention 2 (19.2 days vs 18.6 days, adjusted difference, −2.3 (95% CI −8.7 to 4.2), p=0.49, and 19.8 days vs 16.7 days, adjusted difference, −2.5 (95% CI −6.3 to 1.4), p=0.21, respectively). Mean ICU LOS similarly was not significantly different for both intervention 1 and intervention 2 patients as compared with respective controls (adjusted differences: −2.8 days (95% CI −6.7 to 1.2), p=0.17, and −1.8 days (95% CI −4.9 to 1.2), p=0.24, respectively). Similar to LOS, mortality outcomes (ICU, hospital and 30 days) were not significantly different for intervention as compared with control patients. As a sensitivity analysis, we compared the two collapsed intervention time periods with the two collapsed control time periods and similarly found no significant differences.
Mortality and length of stay for intervention versus control patients
Discussion
In this single-centre, controlled pilot study, a novel end-of-rotation care transition bundle using bedside handoff and videoconferencing was successfully implemented with high clinician adherence. We found acceptability was a perceived barrier, although resident adherence to the intervention was high throughout the study period. Attending physicians and nurses both were more satisfied with the handoff process and the information transfer, but we did not find this translated into perceived or measured improvements in patient outcomes. However, the large effect sizes (a 2-day shorter ICU LOS and 7% lower rate of mortality) suggest lack of power may partially explain our null results. Similar to how Nanchal and others used structure to improve ICU shift handoffs,24 this novel intervention bundle holds promise to provide structure to service transitions in a meaningful way. Despite the lack of incentive as motivation or extra time to complete, resident and nursing adoption of the transition bundle was impressive with 98% of handoffs completed at the bedside, 72% including nurses, 81% including patients or families and 81% using the structured ICU transition checklist. Given the noted ambiguity among residency programmes in how resident handoffs are performed,10 26 27 41 this pragmatic approach may prove valuable.
There are several reasons why shift handoff interventions may not apply or may require modification to be effective for end-of-rotation transitions. First, the lack of recognition for the significance of these transitions has led to inadequate standards; for example, in a survey of 10 academic institutions, only one required transitioning physicians to hand off their patients in person, omitting components of communication encouraged by both The Joint Commission and the Society of Hospital Medicine.10 42 Second, the ‘culture’ of this handoff is different, making an already complex, time-consuming strategy even more difficult to systematically implement.4 5 41 42 The key differences are that physicians who are transitioning off service are frequently transitioning to other rotations or vacation, as are physicians rotating on service, making an in-person handoff logistically more difficult to accomplish even if preliminary data suggest residents value in-person end-of-rotation handoffs.32 Further, since these physicians are permanently transitioning responsibility to another team, an attitude of ‘out of sight, out of mind’ must be addressed. Thus, interventions in this setting must be pragmatic and implementation must acknowledge these cultural differences.
Transition of care-related adverse patient events and outcomes are well documented,3–6 8 9 14–16 yet evidence-based recommendations for how to mitigate miscommunication during end-of-rotation transitions are lacking. As a result, residency programmes and hospitals nationwide have embraced unsupported, ad hoc transition strategies to fill this under-recognised void. A key component to this study’s transition intervention was the bedside handoff using in-person or videoconferencing handoff that provides a situational awareness not addressed in many physician handoff strategies. The strategy of meeting in person is not a foreign concept to the US Marine Corps who recognised this potential pitfall and invested in a long-standing process by which active duty military members transition service when rotating in and out of combat operations in Afghanistan.43 These transition processes are known as ‘left seat, right seat’ operations and occur regularly in Afghanistan when one battalion takes over for another battalion assuming responsibility for the operation. ‘Left seat’ refers to outgoing units who are handing off operational details to incoming units, which are the observing ‘Right seat’. This process can take a variable amount of time, but prior to the outgoing team leaving duty, team leaders switch places to ensure the incoming unit is familiar with the environment and can perform all operations acting as ‘left seat’. In this study, implementation was successful, but acceptability from the resident providers was diminished, mostly due to time and scheduling constraints. Although further exploration is needed, we believe if given dedicated time and/or appropriate compensation as the US Marine Corps has done, in-person transition should become an accepted standard of care when transitioning patients who are critically ill.
Although end-of-rotation care transitions have been studied in hospitalised medical patients,10 11 this is the first description of patient outcomes related to end-of-rotation care transitions of patients who are critically ill. All patients included in this study were adult medical patients located in a closed ICU at the time of service change by resident teams without stringent exclusion criteria. The hospital mortality rate for the entire cohort of ‘transition’ patients was 27.6% which is as high or higher than many patients admitted with septic shock.44 45 Similarly, both ICU and hospital LOS were longer (10.2 and 18.6 days, respectively) than anticipated for these patients which, unlike other studies targeting patients with high risk of death,46 did not necessitate a higher illness severity or specific diagnosis to be included. Although these data may be explained solely by the fact that a sicker population exists in this ICU studied, one might argue the transition itself selects for patients with higher mortality as previously suggested for end-of-rotation transitions in hospitalised medical patients.10 This unanticipated finding deserves attention to elucidate possible mechanisms, but was out of the scope for this project. A future study to examine this finding in greater detail is underway.
It is paramount to highlight that both mortality and LOS may be difficult outcomes to improve with an intervention that targets a single transition of care. Accordingly, there are several relevant and more proximal outcomes that might be investigated such as preventable adverse events or medical errors, both of which were previously shown to improve with a handoff intervention.5 Other related outcomes that might be considered for future studies in an ICU cohort include time to extubation, LOS from the time of transition itself, ventilator-free days, medication errors/changes, or even changes in code status. Mortality and LOS outcomes were chosen in this study based on the hypothesis that a service transition is uniquely different from other more temporary care transitions. The differences are apparent for provider teams (that often switch permanently and all at once) and patients. For example, when teams rotate off service, physicians typically try to reduce their patient lists in anticipation of handoff with the lower acuity patients discharged or, in the case of an ICU, transferred to the medical floor ahead of a significant service transition. The remaining patients, those ultimately exposed to the transition itself, are presumably a more complex group of patients. It is therefore reasonable to assume that an intervention targeting these patients might improve either mortality or LOS or both. The current study does not answer this question but is an important first step in highlighting an often overlooked shortcoming of the modern-day ICU.
This study has limitations. First, this was a pilot study to collect data on a novel intervention in a newly studied patient population (ICU transition patients), therefore we did not perform a power analysis leaving power as a significant concern. However, these data have numerous strengths including serial assessments over time of multidisciplinary perspectives (nursing, attendings, residents), careful attention to balancing measures (not just using self-report) and careful measurement of patient outcomes. Additionally, we have now successfully pilot tested an ICU-focused transition checklist, multiple components to a pragmatic intervention and the first description of ICU videoconferencing to aid in bedside handoff. Second, this is a single-centre study of medical resident trainees which lacks the generalisability to other health systems and those without training physicians. The non-randomised study design and lack of a non-transition patient comparison group are also limitations, but we were fortunate to have chosen to use quality improvement methodology which allowed for adaptability in implementation from intervention 1 to intervention 2, thereby improving provider coordination. Third, an important limitation was our inability to include attending continuity as this could be a significant confounder that may affect patient outcomes. Additional limitations include a short postintervention period, the potential for bias (both Hawthorne for direct observation data and recall bias for survey response data) and the lack of written handoff quality assessment limiting fidelity for this component of the intervention.
Conclusions
Among MICU patients exposed to end-of-rotation transitions of care, a bundled multidisciplinary, patient-centred transition intervention using bedside handoff and a structured ICU transition checklist was successfully implemented with high fidelity and a non-significant trend towards improved LOS. Conspicuously, mortality rates were high among this patient population with more than one in every five patients expiring in the hospital. Attending and nursing staff found the intervention acceptable, but resident satisfaction was limited by scheduling and time logistics. Face-to-face in-person transition via ICU videoconferencing may improve tolerability and should be evaluated further using interoperable health technology innovations.
References
Footnotes
Twitter @jdensonMD, @com543, @BBurkeMD
Presented at Portions of these data were presented at the 2018 & 2019 International Conferences of the American Thoracic Society.
Funding This project was supported by grant funding from the UCH Clinical Effectiveness and Patient Safety Small Grants Program (#63500549) and the NIH/NCRR Colorado CTSI Grant Number UL1 RR025780.
Disclaimer The contents of this study are the authors’ sole responsibility and do not necessarily represent official NIH views.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was reviewed and approved by the Institutional Review Board (protocol number 17-1762).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.