Article Text

Abstract
Background There is widespread recognition that leadership skills are essential for effective performance in the workplace, but the evidence detailing effective leadership behaviours for surgeons during operations is unclear.
Data sources Boolean searches of four on-line databases and detailed hand search of relevant references were conducted. A four stage screening process was adopted stipulating that articles presented empirical data on surgeons' intraoperative leadership behaviours.
Conclusions Ten relevant articles were identified and organised by method of investigation into (i) observation, (ii) questionnaire and (iii) interview studies. This review summarises the limited literature on surgeons' intraoperative leadership, and proposes a preliminary theoretically based structure for intraoperative leadership behaviours. This structure comprises seven categories with corresponding leadership components and covers two overarching themes related to task- and team-focus. Selected leadership theories which may be applicable to the operating room environment are also discussed. Further research is required to determine effective intraoperative leadership behaviours for safe surgical practice.
- Leadership
- patient safety
- surgery
- teams
Statistics from Altmetric.com
Introduction
Surgical patients are at most risk of suffering an adverse event in hospital1 and analyses of adverse events in the operating room indicate that intraoperative failures may be due to a breakdown in teamwork, rather than in technical proficiency.2 Poor leadership is also a likely contributor and has been studied in critical care teams3 but not specifically examined in case reviews of surgical failure.1 4–9 This is in spite of recent statements regarding the importance of leadership in surgery (ie,10) and accounts of surgeons' intraoperative behaviour from sociologists,11 journalists12 13 and surgeons themselves.14
Leadership is defined as ‘…the process of facilitating individual and collective efforts to accomplish shared objectives’15 and has been consistently identified as a key component for the successful functioning of teams.16–18 The quality of supervisory leadership has been related to decreased errors, reduced costs, improved safety19 and increased compliance with safety standards.20–24 In studies of leadership in industry, supervisors' skills in planning, communication, motivation and role clarification have been shown to influence safety climate, team processes and operational safety.20 25–27 Specifically, taxonomies of team leadership have identified functions such as defining the team's mission, establishing expectations and goals, providing feedback, monitoring the team, and solving problems, among others.28
During the intraoperative phase of surgery, the lead surgeon can be likened to a front line supervisor in industry, responsible for task accomplishment by a small team. In this phase, the characteristics of the operating room (OR) match those of other high risk workplaces: the OR is inherently risky because of the complexity, dynamicity, and interdependent nature of surgical practice. Team members increasingly work with unfamiliar colleagues due to the new rota systems being introduced.
Although there may be more than one task specific leader in the OR (eg, circulating team leader or anaesthetist may be directing their subteam),29 the lead surgeon is an integral part of creating a good working environment and ensuring that surgical goals are realised.30 To this end, the Accreditation Council for Graduate Medical Education (ACGME) considers elements of leadership as core competencies in medical training.31 Professional bodies recognise leadership as a core competence for operating surgeons32–34 and leadership is highly valued among surgeons and operating team members.35 In terms of training and assessment in the UK, systems to assess trainee surgeons' intraoperative competence focus on technical ability and do not explicitly cover leadership.36 Medical workplace-based assessments which do cover skills such as the ability to work in a multi-professional team and communication are for the assessment of perioperative skills, often using interactions with patients rather than with other clinicians.37 Across these sources one thing is clear: neither surgical leadership nor particular behaviours thought to be associated with good outcomes are well-defined. Therefore, a first-principles (bottom-up) approach was adopted to determine the behaviours that surgeons engage in as team leaders in the OR and their relative effectiveness for efficiency and safety. This paper synthesises the research evidence in this area, proposing a categorisation of surgeons' leadership behaviours and suggesting candidate theoretical models from the team leadership literature for future investigation.
Method
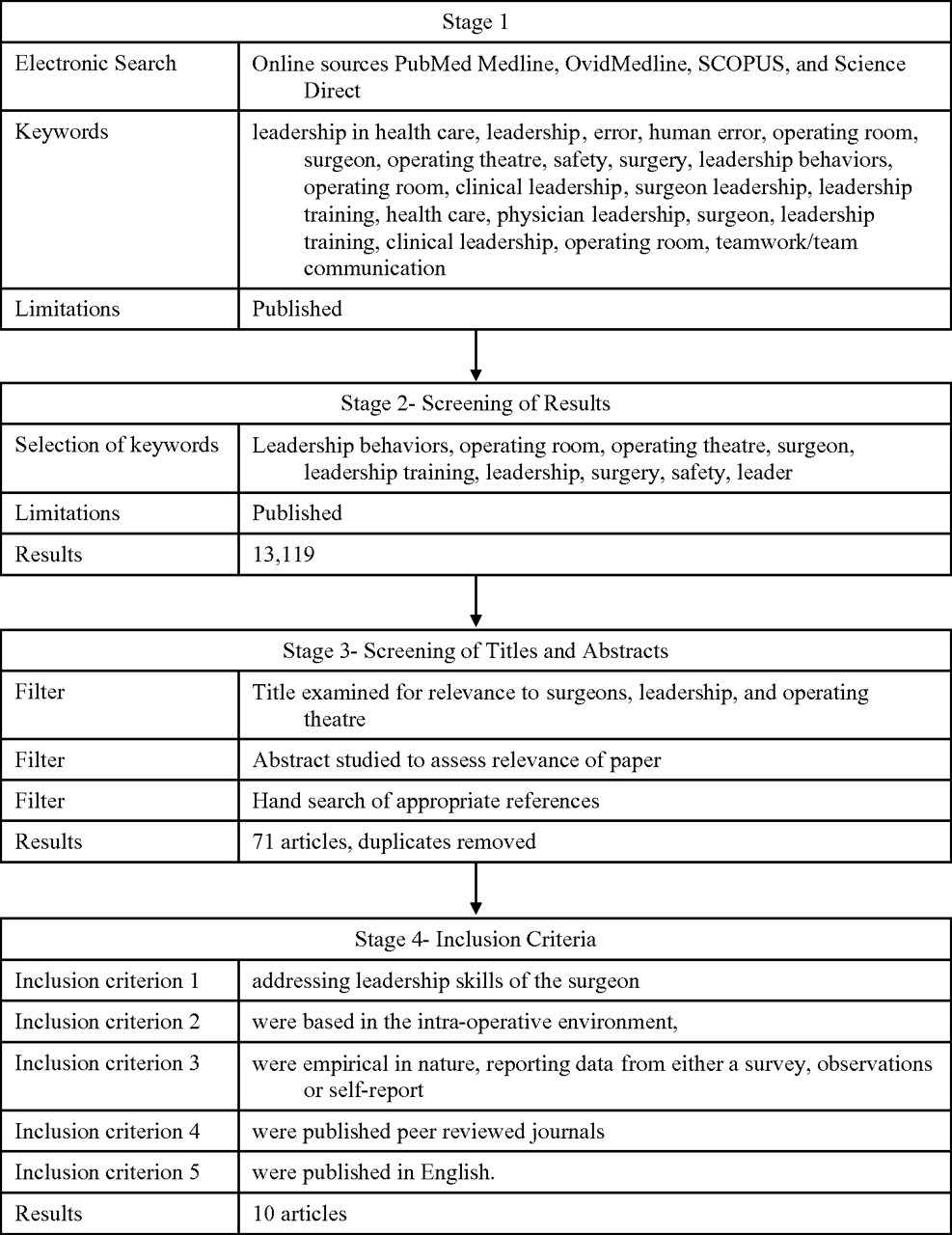
Boolean searches were conducted on online sources PubMed Medline, OvidMedline, SCOPUS and Science Direct, plus a hand search of relevant references from selected articles. No date limitations were set for articles, and the main search was conducted in March 2009. Figure 1 details the search terms and screening process.38 Articles were analysed according to study population, context, method, leadership factors and related clinical outcomes. During Stage 3, duplicates were removed, all articles were read by SHP and were assessed based on the criteria listed in stage 4 by SHP. During stage 3, a hand search of article references was also conducted. For a descriptive list of articles included, see table 1. In this table, articles are organised by primary method of data collection. A short description of the sample; the definition of leadership used by the authors; the method of analysis (A) and outcome measures (O) used, if any, are provided for each article.
{kind=link}
Systematic search method and inclusion criteria.
Leadership articles reviewed in the literature
Finally, leadership definitions and associated behaviours were analysed using a two-phase inductive coding technique, suitable for exploring data and building theory.49 Similar techniques have been used in the development of surgical non-technical skills taxonomies.48 In the first phase, leadership definitions (including behaviours) that emerged from the literature were grouped by SHP using a bottom-up technique, matching similar definitions to each other. Behaviours were assigned to only one category. In the second phase, a group of industrial/organizational psychologists (n=6) was given the sets of leadership behaviours and asked individually to identify a title for each set (table 2).
Proposed categorisation of intraoperative leadership behaviours
Results
The search returned 10 relevant articles in line with the criteria summarised in table 1. Definitions of leadership differed, and only two studies42 47 were designed to show the impact of leadership behaviour on the surgical team or patient safety outcomes. The following section will briefly discuss the articles according to the principal method used: (i) observation, (ii) questionnaire and (iii) interview. Finally, a categorisation of the reported leadership behaviours is proposed based on grounded theory coding.
Observation studies
Behavioural rating scales record observations of staff in ORs (real or simulated) and have been used in anaesthesia, and high risk industries to identify observable, non-technical skills, such as leadership.50 Several studies used behaviour rating systems to observe surgeons' leadership. Each of the behavioural rating systems discussed below include leadership as a subcategory of a taxonomy to assess non-technical skills. Therefore, only results pertaining to leadership will be discussed.48
Non-Technical Skills for Surgeons (NOTSS)
The NOTSS scale is an observational behaviour rating tool designed to assess non-technical skills for individual surgeons in the intra-operative setting.48 This instrument was developed using task analysis with subject matter experts, like measures developed in other industries (eg, NOTECHS in aviation).51 In NOTSS, leadership is one of four categories and consists of three elements: setting and maintaining standards, supporting others and coping with pressure. The NOTSS system has been used by consultant surgeons to rate non-technical skills using videos of simulated OR scenarios.39 Surgeons' ratings were assessed for reliability and internal consistency within six video scenarios and then compared to expert ratings. Leadership behaviour ratings were made immediately after the case based on notes taken ‘live’. Ratings reached acceptable within-group agreement (reliability) and moderate sensitivity measured by accuracy of participants' ratings against expert judgements.
Adaptations of non-technical skills scales from other industries
Sevdalis and colleagues40 revised the aviation Non-Technical Skills for Pilots (NOTECHS) scale50 51 for use in the OR. Leadership was one dimension, defined as adherence to best-practice during procedure, time management, resource utilisation, debriefing the team, and authority and assertiveness. Trainers rated clinical trainees after crisis simulation training on the Revised NOTECHS. Trainees rated themselves using the Revised NOTECHS after the scenario. For leadership and managerial skills across all participants, satisfactory inter-item correlation was found. Using the same scale, Undre et al41 assessed surgical teams on non-technical skill ratings during crisis simulation training. The same rating method as above was used. Surgeons scored adequately on the technical aspects of the assessment, however, both surgeons and anaesthetists scored lower on leadership skills than nurses. Overall, leadership scores were lower for the overall operating team than other non-technical skills.
The aviation NOTECHS scale51 has also been adapted for rating the behaviour of surgical teams, and called the Oxford NOTECHS.42 Their scale scored OR sub teams (surgeons, anaesthetists, and nurses) on non-technical dimensions within a single operation and was complemented by measures of errors in surgical technique, procedural problems, operating time and adverse events. Operating time was significantly correlated with both surgeons' and anaesthetists' leadership and management scores, and operation type. An increase in the leadership and management scores of the surgeon was related to a decrease in operating time, while an increase in the leadership and management scores of the anaesthetist was positively correlated with operating time. An increase in the leadership and management scores for nurses resulted in a significant decrease in procedural problems and errors. These findings should be interpreted with some caution as there are many other variables that may be unaccounted for such as the type of surgery and the specific skills required for a particular procedure.
Observational Teamwork Assessment for Surgery (OTAS)
The OTAS is an observation tool designed to assess OR teamwork.43 Leadership is defined as provision of direction, assertiveness and support among team members in OTAS. In one study, leadership was rated high to very high for each stage assessed (pre-, intra- and post-operatively), however, no reliability or validity measures were reported. The OTAS was also used to measure teamwork in 50 urological procedures, and two observers' ratings of leadership behaviour in the surgical team were significantly positively correlated (r=0.62, p<0.01).29 Data presented show that non-technical skills were significantly different across disciplines. Surgeons' intraoperative leadership behaviours were rated significantly higher than nurses' or anaesthetists'.
Questionnaire studies
Questionnaire studies are commonly conducted to determine workers' attitudes or perceptions towards leadership of self or others.
Multifactor Leadership Questionnaire (MLQ)
The MLQ52 measures transformational and transactional leadership styles and is the most widely used instrument for leadership research.53 Surgical residents in the USA completed the self-assessment version of the MLQ and self-reported leadership behaviours.44 In this study, it was found that during their initial training residents emphasise transactional leadership behaviours, but as they progress they adopt a more transformational style. Compared to the general population, surgical residents reported higher ‘management by exception’ behaviours, meaning they took more corrective actions with their followers and they were less supportive of each other, seeing themselves as highly independent. Generally, transformational leadership was strongly associated with high work motivation and job satisfaction in surgical residents.
Operating Room Management Attitudes Questionnaire (ORMAQ)
This scale was adapted from aviation54 55 to measure teamwork and leadership styles in the OR.2 Most consultant surgeons (54%) in Scotland stated that they use a consultative style of leadership, with few reporting using autocratic or delegative styles.45 However, trainee surgeons (30%) and nurses (59%) encountered autocratic leadership styles but preferred explanatory or consultative styles.
Safety Attitudes Questionnaire (SAQ)
Makary et al46 also found that perceptions of teamwork differed between surgeons and theatre staff. Utilising the SAQ, a refined version of the ORMAQ, they measured teamwork in the surgical setting. With respect to leadership, nurses reported that good collaboration was having their input respected, whereas surgeons reported good collaboration as having nurses that can anticipate needs and follow instructions.
Interview studies
Interview studies are also used to explore aspects of leadership.56 Yule et al48 conducted interviews with consultant surgeons using the critical incident technique, which asked surgeons to talk about behaviours during a challenging case. Leadership was regarded as important and examples of good leadership behaviours were: following theatre protocol, modifying behaviour according to trainees' needs, establishing a rapport with team members, remaining calm under pressure, emphasising the urgency of the situation, taking responsibility for the patient in a crisis situation and delegating tasks to achieve goals. Examples of poor leadership behaviour were failing to observe standards, not providing recognition for tasks performed well, showing hostility to other team members, failing to pass leadership of the case when the technical challenge requires full attention and losing one's temper.
In a study of introducing a new surgical technique, Edmonson47 interviewed members of cardiac surgical teams (surgeons, anaesthesiologists, nurses and perfusionists). She found that the most effective leaders helped teams learn by ensuring that the entire team understood the impetus for the change, and by motivating staff to speak up across ‘power gradients’ (ρ=0.70, p<0.01). This study is unique in that it shows learning outcomes (ease of integration of new technology) were positively associated with the perceptions of surgeons' leadership behaviour.
Although leadership has been examined as part of non-technical skills taxonomies, the authors themselves acknowledge48 that further investigation and evaluation of the subcategories is necessary. Leadership was also identified in questionnaires as important for team performance, but only once was it examined in isolation44 and has not been linked to patient or team outcomes in the OR. Interview studies found that leadership can influence team learning and innovation.47
Categorising surgical leadership behaviours
Leadership behaviours were identified in nine of the ten studies. Different definitions of leadership were used and no coherent pattern of effective leadership behaviours for surgeons emerged from the literature. Having identified a list of surgeons' leadership behaviours from the studies, imposing a higher order categorisation was necessary. One study44 was not included in this exercise because the leadership theory used did not articulate specific behaviours for surgeons. The two phase labelling procedure produced seven leadership categories and titles for each category (table 2).
Maintaining standards can be seen as behaviours that reinforce standards such as following rules and established procedures. Managing tasks refers to the ability to maintain task performance while ensuring timely and effective task completion. Making decisions refers to the ability to seek out appropriate information, synthesise the information and make an informed, prompt judgement. In making surgical decisions, there may be many different information sources to take into account, as well as differences in intra-operative risk to cope with.57 Managing resources refer to both people in the OR team and equipment required for surgery. A leader should be able to effectively assign resources depending on the situation or context. Directing and enabling behaviours are more interpersonal in nature and promote accomplishment of task and interpersonal goals through team members. Guiding and supporting behaviours suggest more of a teaching and coaching perspective, involving the team in decisions and allowing for input from team members. Finally, communicating and coordinating behaviours enable information exchange and help the team to perform as a unit, rather than as individuals.
Discussion
This paper reviews the literature describing surgeons' intraoperative leadership behaviours and builds on earlier studies by providing a proposed categorisation of surgical leadership behaviours. Although leadership in the intraoperative setting is regarded as an integral part of successful surgery, we found limited empirical literature describing surgeons' leadership behaviours. Only ten studies met the review criteria, and of these two42 47 were designed to show the impact of leadership behaviour on either the surgical team or patient safety outcomes. Although the scientific literature on industrial leadership theory is extensive, only one study44 used an established theory to determine the leadership behaviours required to enhance safety in the OR. The studies reviewed were mainly descriptive in nature rather than explanatory. Therefore, we still neither know what the explicit goals of intraoperative leadership behaviour are nor how good or poor leadership can impact on outcomes. Despite the anecdotal evidence of the importance of leadership in the OR, the empirical evidence is currently lacking.
In order to evaluate intraoperative leadership, specific, observable, behaviours must be explicitly defined. Only then can their predictive validity for task performance be tested. A preliminary set of core surgical leadership behaviour categories emerged from the literature and serves as an illustrative first step towards a model for intraoperative leadership.
The seven categories of leadership behaviour which emerged from this review were closely aligned with general models of effective task and team leadership.58 59 Task functions (eg, maintaining standards, managing tasks, making decisions, managing resources) ensure that the goal of the surgical team is achieved. Team functions (eg, directing and enabling, guiding and supporting, communicating and coordinating) ensure that the leader also focuses on enhancing the wellbeing of individual team members and the function of the team as a whole. The two functions are interrelated, and a superior team leader should focus on both.60 If a team is well supported by the leader, the members are more likely to work well together, which facilitates goal accomplishment. Similarly, if a team is efficient, productive and successful, it facilitates a positive working climate. This relationship is not one-way, but rather cyclical in nature. Deficiencies in either function will lead to a less successful team.61 Although this review was focused on surgeons' leadership, table 2 suggests that a surgeon may have to concentrate on performing the task, to the exclusion of maintaining the team. These findings are similar to other studies of leadership in healthcare teams.3
Another main finding of this review was that only one study was based on an established leadership theory. This was surprising given the breadth of scientific understanding regarding leadership in the workplace and the plethora of theories from which to select. Table 3 presents a judicial selection of leadership theories that we suggest are of particular relevance to the OR and worthy of further examination. Leader behaviours focused on the task and team such as those that emerged from the present literature review are embedded in many of these theories.62 63 Table 3 shows that leadership can be conceptualised as an individual or team phenomenon, that aspects of the situation may exert influence64–66 and that the process may be formal or informal. Leadership has also been characterised as transformational67 for followers based on an exchange between leadership and follower, and that team and task performance are a function of the leaders' adaptability, flexibility and ability to balance competing demands.68 70 Leadership can also be focused internally, exclusively for the benefit of individual team members, or externally, to deal with wider influences on team performance, or both. Finally, it is possible that leadership may not be restricted to one individual but be shared among team members69 or emerge from complexity.71 It is premature to decide which of these theories or models is most suitable for explaining the diffuse influences of leadership in the OR, but there are several potential candidate theories on which to base future research. The function or purpose of the leader is therefore dependent on the theory.
Suggested leadership theories for application in the OR
Conclusion
The goal of this review was to determine the current state of the literature regarding surgeons' leadership behaviours during an operation and to determine whether there is any evidence that certain behaviours might be more appropriate than others. We found mainly descriptive evidence of leadership behaviours, detailing when and how frequently certain behaviours are enacted, and only limited findings showing which behaviours were most appropriate for safety. This indicates that further research must be conducted. In planning future studies, it is important that intervening variables between leadership and outcomes such as the experience of the OR team; the urgency of the surgery; the type of procedure, or the acuity of the patient, must be taken into account. This basic research is essential in order to enhance our understanding of the myriad influences on operative safety. There are also practical benefits, such as developing evidence-based training for surgical residents,72 as is common in other industries.68 Extending the descriptive work conducted so far using one of the theoretical frameworks suggested, and then assessing the impact of leadership on team performance and patient outcomes are essential next steps.
References
Footnotes
Funding This work was supported by the Scottish Funding Council.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.