Article Text

Abstract
Background Logic and experience suggest that it is easier in some situations than in others to change behaviour and organisation to improve patient safety. Knowing which ‘context factors’ help and hinder implementation of different changes would help implementers, as well as managers, policy makers, regulators and purchasers of healthcare. It could help to judge the likely success of possible improvements, given the conditions that they have, and to decide which of these conditions could be modified to make implementation more effective.
Methods The study presented in this paper examined research to discover any evidence reported about whether or how context factors influence the effectiveness of five patient safety interventions.
Results The review found that, for these five diverse interventions, there was little strong evidence of the influence of different context factors. However, the research was not designed to investigate context influence.
Conclusions The paper suggests that significant gaps in research exist and makes proposals for future research better to inform decision-making.
- Quality of care
- research
- safety culture
Statistics from Altmetric.com
Introduction
To date, much of the evaluative patient safety research has concentrated on whether or not a patient safety intervention reduces adverse events. This paper does not consider the evidence of the efficacy of patient safety practices (PSPs). Rather, it considers the research evidence about whether, or how, the implementation of five PSPs is influenced by features of the situation in which it is implemented (termed ‘context factors’), and the practical and research implications of this evidence.
Regulators and accrediting agencies are increasingly requiring health providers and healthcare services to implement changes which are thought to improve safety. These are usually clinical-level changes to behaviour or organisation which have been termed ‘PSPs.’1 At the provider level, it has been suggested that there are factors which affect how the provider responds to these external regulatory influences. One is whether the provider has an information system which already allows easy collection and reporting of quality indicators.2 Another is provider attitudes to safety and willingness to change.3 These factors may affect implementation of different safety changes but are more local than the national or regional context factors.
Commentators and implementers refer to the importance of ‘context’ for understanding why some PSPs are implemented successfully, and are more effective in some organisations and regions and not in others.4 But what is the research evidence of whether or how much context factors influence implementation? Are certain factors, such as an electronic medical record or the size of a healthcare organisation, more influential for implementing some PSPs, and not for others?
Method
The study reported in this paper was part of a larger programme to provide guidance for safety research by describing the strengths and limitations of different research designs for different questions, and by assessing the influence of context.5 The method for deciding which interventions to consider and for searching and reviewing researcher into these interventions is described in detail in the programme report and in this journal.6 7 In summary, the method involved compiling a comprehensive list of PSPs from different sources. This list and the criteria for selecting a limited number were discussed by a 22-member expert panel (TEP), first through a survey and then at a formal meeting. The steps in the selection are shown in figure 1.
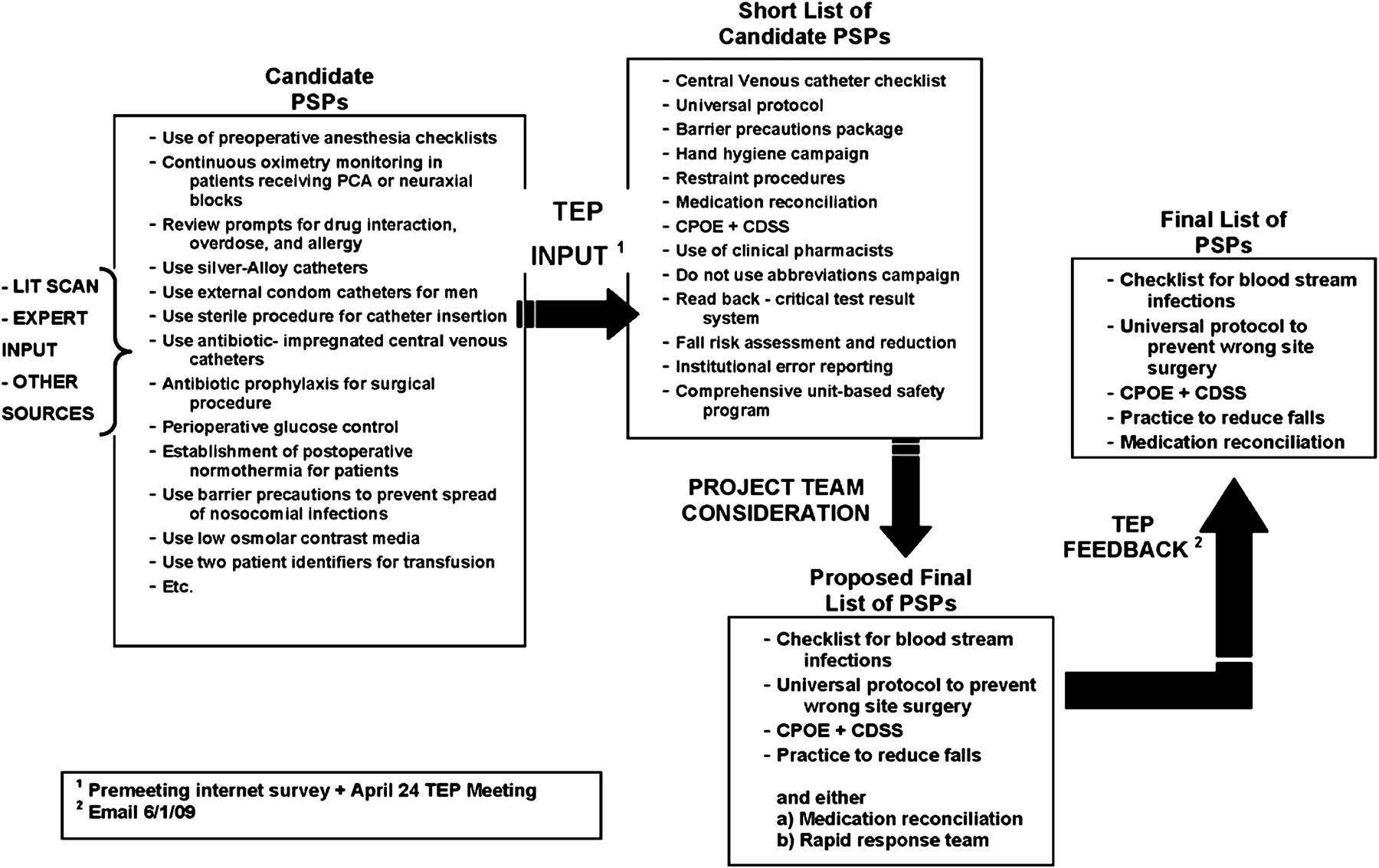
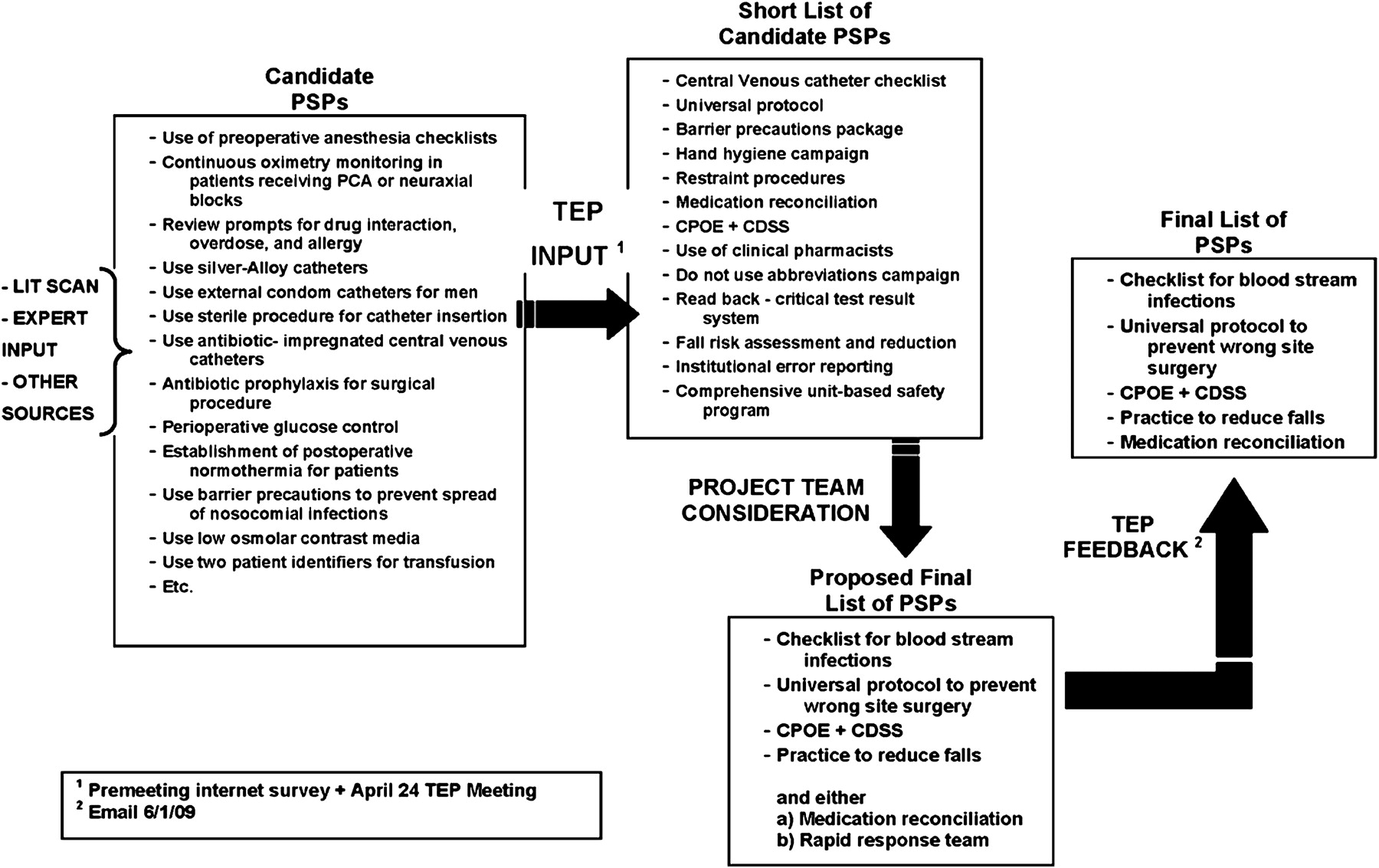{kind=link}
Selection of the diverse and representative patient safety practices (PSPs). (CDSS refers to computer decision-support system; CPOE refers to computer physician order entry).
The criteria agreed were: diverse in terms of the panel's assessment of ‘sensitivity to context,’ the range of settings to which the PSPs could apply, whether they were regulated or not, their feasibility, the strength of evidence about the PSP effectiveness and the extent of behavioural change required for implementation. The five chosen after applying these criteria were: interventions to prevent catheter-related bloodstream infections (CRBSI), universal protocol for wrong site surgery,8 medication reconciliation tool and process redesign, computer physician order entry (CPOE) and computer decision-support system (CDSS), and patient fall-risk assessment and reduction interventions in institutions.
‘Context’ was defined as everything else that is not the intervention, but especially those aspects which may influence the intervention implementation and outcomes. Different subgroups of the project team were established for each PSP to review the evidence of context influences.
The first stage was to assess ‘seminal studies’ proposed by the TEP which are listed in Taylor et al.7 These and other studies were then retrieved and assessed for evidence regarding the reporting or investigation of context. For three of the chosen PSPs (medication reconciliation, the Universal Protocol and CRBSI) additional searches were made within Medline, using standard search methods for studies of implementation, which were then examined for their reporting of contexts. For the other two chosen PSPs (Patient Falls, CPOE/CDSS), further searches found many hundreds of publications describing implementations, from which those likely to report context factors were selected on the basis of the title and abstract. This paper presents a summary of the evidence reported in these studies and summarised in table 1.
Summary of findings from reviewing evidence presented in studies of five patient safety practices
Findings
Patient fall-risk assessment and reduction in institutions
This review found one study which examined context factors affecting implementation.9 It found some other studies reporting context factors but not investigated systematically, or as a single focus of the study.10 Overall, there is no strong evidence either for or against context factors either helping or hindering implementation of falls interventions in institutions. There is some limited evidence that unit leadership may be important for implementing falls interventions successfully, and a positive safety culture is a helpful context factor, the absence of which can influence implementation.9 However, specifics were missing in this study about how these factors were defined, and how precisely they exerted their influence—for example, by providing any type of theory of context influence.
This review did not find any evidence that different context factors influenced implementation of falls interventions differently at different times during implementation. Theory and other research suggests that future research into falls interventions could report or assess the possible influence of the following context factors: general awareness of risks of falls, the existence of community falls programmes, leadership at different levels, regulation, reporting, financial incentives, resources of the unit (staffing, and other), implementation resources and support, and measurement and data support. In addition other research suggests, that different measures could be used to gather data about context factors, such as the ORCA readiness for change measure. 11
Medication reconciliation tool and process redesign
No studies of different types of medication reconciliation interventions were found which rigorously assessed the influence of different contexts factors in implementation or in relation to outcomes. However, nine out of the 25 eligible studies provided some modest data or qualitative assessment of context influences. Most of these nine studies focused on patient factors (eg, number of medications as a modifier of effect). Only one context factor was reported in more than one study—the use of ‘blocking functions’ in electronic systems to increase compliance with medication reconciliation steps.12
Other studies report some general descriptions of context factors. The quality of the studies, though not assessed formally, appeared to be poor, as did the definitions of context factors. This limited the review team's ability properly to compare studies to find patterns of context factors that might be influential in success or failure. Many articles reported details about the implementation, including adjustments made when spreading the use of a tool. It appears that pilot testing and adjustment may be important aspects of a successful medication-reconciliation programme, although no study compared using an iterative process against a one-time implementation. This, however, in some studies would be considered part of the intervention or implementation rather than a context factor—studies drew the boundary between intervention and context in different ways.
Prevention of CRBSI
Most studies did not mention or describe in any detail context aspects other than patient characteristics. Some made brief notes about type of hospital, or analysed and described context qualitatively. Koll (2008) conducted an interventions survey of hospitals participating in a collaborative based on a ‘bundle intervention.’13 The study describes some context factors in those hospitals which performed highly in the collaborative, including leadership involvement, teamwork (nursing staff empowerment and interdisciplinary rounds) and training resources (educational programmes). The study does not describe how an assessment was made to know these context factors were influential.
Bonello et al discussed the following context elements as barriers to success in one study: lack of sufficient time or resources, organisational regulatory barriers and lack of a quality improvement infrastructure within the organisation.14 Many of these are also mentioned by other studies. Render et al also mentioned context elements as barriers and facilitators, including involvement of hospital leadership, project leadership, quality improvement experience, education and motivation.19
Rosenthal et al noted that previous or concurrent hand-washing campaigns were likely to affect the success of CLABSI interventions, and this, or the culture changes associated with this could be considered one context factor.15 Pronovost et al used the Safety Attitudes Questionnaire16 to measure safety culture before and after a multifaceted CRBSI intervention, and found a statistically significant improvement in culture with the intervention.17 This study also describes context elements included in the intervention and, with some variation, of all the other collaborative studies, including education, teamwork and culture interventions, and leadership (both development of unit leaders and involvement of executives), as well as feedback and support of outside quality-improvement expertise.
Universal protocol for wrong-site surgery
The search did not find any studies in which context was systematically examined in relation to the uptake or impact of the ‘universal protocol.’ There was some limited research on how context factors influence the outcomes the practice aimed to eliminate. Blanco et al investigated wrong site surgery ‘near misses’ and actual occurrence at 97 facilities across Pennsylvania.18 They reported several risk factors that differentiated near misses from actual occurrences, and reported many contexts factors that appear related and which some might define as part of implementation and not as context, and some might define as part of the intervention. These included participation of the surgeon in preoperative verification, participation of all surgical team members in the time out, and the surgeon explicitly empowering team members to speak up if concerned and acknowledging concerns when expressed. ElBardissi et al also found a strong correlation between the occurrence of technical error and teamwork failures.20
CPOE and CDSS
More studies of this PSP noted contextual factors which appeared to be important to implementation success than did studies of the other four PSPs. Those factors reported in one comprehensive review18 included: regulation (100% of the 23 papers reviewed), external incentives (100%), organisational size and type (100%), teamwork (74%), leadership (30%), culture (9%), training (61%), internal incentives (52%), audit and feedback (35%), and quality improvement consultants (13%). Several articles describe factors that were thought to underlie notable successes at specific organisations, or failures at other organisations. Several of these are context factors, and others are related to the implementation process or the technical features of the CPOE systems.21
Overall, however, the effect of contextual factors on the success or failure of CPOE does not appear to have been examined in a rigorous manner, using either quantitative or qualitative methods. The search and review did not find any rigorous studies of the effect of context factors on the success or failure of CPOE/CDSS. Only one study attempted to consider factors associated with success or failure in a systematic manner, including some contextual factors, but found too much heterogeneity in study designs and outcome measures to do so in a statistical manner.22
Discussion
This assessment of evidence reported by research into PSPs was limited to research into five such PSPs. These were chosen to represent a diverse set of practices, but it is possible that studies of other PSPs have reported evidence of the influence of context factors. It is also possible that studies of these selected PSP do exist which report evidence of context influences, but that these were not identified in the title and abstract search used, or were not mentioned in the reviews of research. However, we are confident that the review summaries give an accurate picture of what is reported about context for the five PSPs examined. The aim of this paper was to report the findings from these reviews, which can be summarised as follows:
These reviews found little evidence reported in studies of five diverse PSPs that context factors influence implementation or effectiveness.
Lack of evidence about context is not evidence that context does not influence implementation or effectiveness. Most research to date has not been designed to investigate different context influences rather to control for context in order to establish the efficacy of the PSP.
In contrast, case studies and experiential evidence in the wider field of quality improvement suggests that different aspects of context are important. This evidence suggests that the spread and scale-up of PSPs is hindered by a lack of evidence about which aspects of context are critical for implementation.23 For this reason, and in order to develop safety science, more studies are required whose sole aim is to understand which aspects of context are important for different PSPs, and which use research designs suited to this aim. In such research, it will be important to consider the following issues, which were identified in discussions by the study team of the research reviewed above.
Definition of context
Context was defined in the early stage of the study and in this paper as ‘everything which is not the intervention,’ but there are different definitions of context, and of the related terms ‘intervention’ and ‘implementation.’22 Some definitions recognise that only some aspects of context influence implementation, and term these aspects ‘conditions influencing implementation.’24 Some view implementation as part of context, and as separate from the intervention; others view the intervention as including implementation actions. The findings from the reviews above suggest that context factors only influence effectiveness through their influence on implementation actions and on intermediate changes, by helping or hindering these actions and changes.
At this stage in the development of the science, it may be premature to define terms and a framework which all studies should use to report or investigate context, especially as it is possible that different context factors are more influential for some PSPs than for others. However, it is important that the definitions used in studies are made clear so as to avoid misunderstandings, and that there is a recognition of the different ways in which the terms are used. The paper later gives an outline framework which could be used as a starting-point in such studies.
Context and ‘readiness to change’
Some research includes context influences in change processes in healthcare organisations as part of the concept of ‘readiness to change’ (RTC).3 11 However, the evidence basis for readiness to change measures is limited. As a general measure of local organisational aspects, it may not cover some context influences which are important for some PSPs. The relation between the RTC construct and context for PSPs needs further elaboration, as it may be a useful method to use for studying some PSPs.
Conceptualisation of context and research methods
To date, most research has conceptualised context as separate, or separable and discrete influences, emanating from different levels of the health and government system to affect the PSP implementation or its effectiveness. Most of the research which did mention aspects of context noted these as likely influences and did so descriptively and in passing. Few studies have tried to measure the influence on either implementation or PSP effectiveness. Some progress might be made by pursuing this approach, but progress also is likely using other conceptualisations. Context can be viewed as influences which interact with each other, and interact with the implementation process. Here the relative arbitrariness of the boundary between intervention and context is recognised. This more dynamic view is perhaps congruent with the iterative or adaptive implementation process through which many PSPs are implemented, where implementers review progress and adjust implementation in order to respond to a changing context—as they perceive it. This way of conceptualising a safety change poses challenges for research, but also new opportunities for understanding context because it means studying context as perceived and responded to by implementers. It may be possible to combine methods for studying these perceptions and explanations for implementation-adjustments with methods for gathering more objective data about context in a mixed method study.
The findings from these reviews were discussed by the TEP as part of the larger study, which went on to identify the following domains of context as being likely to influence implementation and effectiveness of PSPs. The report and other publications in this Journal describe how context might be better described for research and for practical action.5–7
Implications for future research
The scientific field could be advanced by a recognition of the need for clarity about concepts and theory regarding context, and by requiring researchers to make these clear in proposals and in final reports. Second, there is a need for empirical research, informed by theory, which focuses on understanding which context factors influence implementation of different PSPs. Research needs to establish if these influences only affect implementation, and/or whether they affect the effectiveness of a PSP once implemented in those PSPs where implementation can be defined as ‘finished.’ Ideally, multiple studies of the same PSP in different contexts could be carried out, and this related to understanding variations in success in implementation and in outcomes.
In addition, studies of different PSPs are needed to find out if there are different contexts which are more or less influential for some PSPs and not for others. This could be through an organised strategy and programme of research so that each study could contribute to accumulating knowledge about context and PSPs. A key question is how similar the methods used in each study need to be in order to allow accumulation, especially given that a variety of research approaches may be useful. This relates to the third implication for research: that non-experimental and social science methods can be used more to advance understanding of context, especially for understanding context influences in ‘adaptive implementation processes’ for PSPs, and for understanding interactions between context influences and between these and the intervention.25 26 One set of methods for explicating the programme theory—the underlying assumptions about which actions will lead to which intermediate and final outcomes—is one such method which has been in use for over 25 years in evaluating social programmes.27 28
Conclusions
Experience suggests that ‘context counts’ for how easy it is to implement a safety intervention. A PSP may be effective in one or a few services, but can it be implemented in other types of services, and at what cost? This review of published research found some evidence that context factors influence implementation and that these factors vary between organisations, but it could not give a satisfactory answer to the title question. The review teams found both limited research into the subject and limited evidence about context in the research which had been carried out. There was little evidence from controlled experimental studies, possibly because they are designed to exclude context factors rather than examine their influence. There was some evidence from a few studies using measures of context, and from qualitative research. This showed influences at different levels of the heath system which helped and hindered the implementation of five selected PSPs, but the evidence was not strong or very specific.
Regardless of the research base, implementers and policy makers take context factors such as regulation into consideration in decisions about which safety practices to implement and how to implement them. Patient safety could be speeded and costs saved with a more research-informed approach to selection and implementation of PSPs which includes evidence of context influences; also with a recognition that many ‘interventions’ are not single-time changes but evolve over time in interaction with their context—perhaps better described as ‘inno-volutions.’23 Studies would be more useful to implementers and allow more strategic replication if they provided precise descriptions of the evaluated intervention and the implementation processes24; in addition, if they defined more clearly what is the intervention and what is not (‘context’), and which aspects of context were or may be important to implementation and outcome effectiveness.
Acknowledgments
The expert panel included AS Adams, DW Bates, L Bickman, C Brown, P Carayon, L Carr, L Donaldson, N Duan, DO Farley, T Greenhalgh, J Haughom, ET Lake, R Lilford, KN Lohr, GS Meyer, M Miller, D Neuhauser, G Ryan, S Saint, K Shojania, SM Shortell, DP Stevens and K Walshe.
References
Linked Articles
- Original research
- Original research
- Original viewpoint