Article Text

Abstract
In the wake of adverse events, injured patients and their families have a complex range of needs and wants. The tort system, even when operating at its best, will inevitably fall far short of addressing them. In Australia and New Zealand, government-run health complaints commissions take a more flexible and expansive approach to providing remedies for patients injured by or disgruntled with care. Unfortunately, survey research has shown that many patients in these systems are dissatisfied with their experience. We hypothesised that an important explanation for this dissatisfaction is an ‘expectations gap’; discordance between what complainants want and what they eventually get out of the process. Analysing a sample of complaints relating to informed consent from the Commission in Victoria (Australia's second largest state, with 5.2 million residents), we found evidence of such a gap. One-third (59/189) of complainants who sought restoration received it; 1 in 5 complainants (17/101) who sought correction received assurances that changes had been or would be made to reduce the risk of others suffering a similar harm; and fewer than 1 in 10 (3/37) who sought sanctions saw steps taken to achieve this outcome initiated. We argue that bridging the expectations gap would go far toward improving patient satisfaction with complaints systems, and suggest several ways this might be done.
- Patient satisfaction
- complaints
- patient safety
- compensation
- communication, Adverse events
- epidemiology and detection
- checklists
- health policy
- medical error
- health care quality
Statistics from Altmetric.com
- Patient satisfaction
- complaints
- patient safety
- compensation
- communication, Adverse events
- epidemiology and detection
- checklists
- health policy
- medical error
- health care quality
Introduction
In the wake of adverse events, injured patients and their families have a complex range of needs and wants. These include remedial treatment, information about what went wrong and why, an apology, monetary compensation, assurances that steps have been taken to prevent future harm and, in some cases, disciplinary action against a responsible healthcare provider.1–3 The medical negligence system focuses on one class of events (substantial injury due to substandard care) and a single remedy (monetary compensation). It is not designed to address other types of patient dissatisfaction or deliver other remedies. Indeed some of the negligence system's core features, such as its emphasis on fault finding and the cloak of confidentiality with which it shrouds settlements, actively inhibit opportunities for patients to secure other forms of succour, such as explanations, apologies, prevention and learning.4–6
In the Antipodes, health complaints commissions have emerged as a bold attempt to fill this void.7 8 New Zealand and all eight Australian states and territories have established state-based ‘commissions’ over the last 25 years. Commissions have statutory responsibility for receiving, investigating and resolving disputes relating to the provision of healthcare services; collectively, they handle about 10 000 complaints per year.
Filing a complaint is free and legal representation is unnecessary. The role of commissions is to act impartially and resolve complaints cheaply, effectively and quickly. To achieve this, commissions deploy an impressive range of procedures (eg, advocacy, mediation and conciliation, formal investigation, referral to other agencies) and remedies (eg, explanations, apologies, monetary payments, corrective action and provider sanctions). The Australian commissions coexist with the civil liability system. In theory, patients have a choice about whether to lodge a complaint, litigate, or do both. In practice, plaintiffs' lawyers often wait for the outcome of complaints before determining whether to take up the matter as a negligence claim. In New Zealand, medical malpractice litigation is essentially barred. In lieu of this, a system of government funded no-fault compensation9 operates in parallel with the Commission's complaints processes.
In summary, commissions fill many of the gaps commentators have long lamented in the medical negligence system.5 6 10 It thus comes as a surprise to find emerging evidence that commissions often fall short in meeting the expectations of patients and families who turn to them for relief. Studies from Australia,11–13 and similar schemes in other countries,14 15 have all found that a third or more of patients express dissatisfaction with how their complaint was handled.
This article probes this puzzle. We use a case study of complaints from Victoria, Australia's second largest state with 5.2 million residents, to test the hypothesis that there may be a significant mismatch between what patients want from dispute resolution and what they get. We conclude by considering lessons for Australian commissions, counterpart agencies in other countries and other institutions (eg, hospitals, practitioner registration boards) involved in the resolution of healthcare complaints.
Understanding expectations
Studies of what drives consumer satisfaction with complaints resolution processes inside14 16 and outside17–19 healthcare settings point to three dimensions of the experience: the perceived fairness of the procedures used to arrive at the outcomes, the quality of interpersonal interactions during the process and the extent to which the outcomes obtained match those sought. The third dimension, whether consumers get what they want, is a core concern in commerce20 21 but is often poorly understood in human services.
This is certainly the case for healthcare complaints in Australia and New Zealand. Only one study,11 now a decade old, has explored complainants' expectations and the extent to which they are met. After identifying widespread dissatisfaction with the Health Care Complaints Commission in New South Wales, the authors concluded that ‘understanding what (patients) expect, as well as what they can feasibly and legitimately expect by way of resolution, may obviate some of the difficulties and disappointments revealed by our survey’.
Using data on a sample of complaints lodged with Victoria's Commission (‘the Commission’), we identified remedies sought by complainants at the outset of their complaint and correlated them with the remedies complainants ultimately obtained.
A case study from Victoria
Data collection and key variables
As part of a larger study of informed consent disputes between patients and doctors, we identified every complaint lodged with the Commission over a 7-year period (1 January 2002–31 December 2008) that alleged problems with the informed consent process and was serious enough to progress to conciliation. Specifically, ‘cases’ were defined as complaints in which a patient (or patient representative) alleged that the quality or quantity of information provided about a treatment prior to the patient's decision about whether to undertake it, or the process through which the patient was asked to consider such information and make a decision, was deficient.
Details of how the informed consent complaints were identified and reviewed are described elsewhere.22 In summary, the Commission received 9115 complaints over the study period, 1898 (21%) of which proceeded to conciliation. Two medically-qualified reviewers screened these complaints to determine which met the study definition of a case. For those that did (n=218), the reviewers used an electronic data collection instrument to collect a range of variables about the complaint.
Variables indicating what remedies complainants sought and what remedies they obtained form the focus of this analysis. Information on remedies sought came from the initial complaint letter and responses to the following question on the Commission's standard complaint form: ‘What do you hope to gain from lodging the complaint? What outcome are you seeking?’. Information on remedies obtained came from the conciliator's written report on the outcome of each case.
The screening and reviews were conducted onsite at Commission offices in Melbourne between March 2009 and January 2010. The study was approved by the University of Melbourne Human Research Ethics Committee.
Typology of remedies
The instrument directed reviewers to classify remedies sought and obtained into four categories: restoration, communication, correction and sanction. This classification system has been used in previous research2 and aligns well with the range of possible outcomes publicised by the Commission.23 24
Several of the categories warrant further explanation. Although restoration includes monetary compensation, commissions have no legal powers to award monetary damages. Rather, financial settlements occur through the negotiations and dispute resolution processes that commissions oversee; this may involve reimbursement or waiver of out-of-pocket expenses, or more comprehensive forms of financial restitution, such as compensation for lost wages or pain and suffering. Commissions also do not have direct authority to sanction health practitioners and institutions, but they may act as gateways, referring matters to other medico-legal agencies that do, such as health practitioner boards. Finally, the correction remedy refers to action taken by commissions to leverage improvements in the quality and safety of healthcare in response to particular complaints. The two main ways in which this occurs currently is through the making of formal recommendations and the targeted dissemination of findings.25
We counted a remedy as being ‘obtained’ if it was provided in any form. In most cases, it was not possible to make qualitative determinations of the degree to which the remedy's content matched what the complainant sought. So, for example, a complainant who sought payment and received it was counted as having obtained restoration, even though the amount obtained may have been less than what they desired.
Reliability of complaint file review
To test the reliability of the review, a random subsample of around 15% (n=37) of the complaints was re-reviewed by the second reviewer, who was blinded to the first review. The reviewers agreed on the remedies sought in 89% of cases and agreed on the remedies obtained in 92% of cases.
Remedies sought
Table 1 shows the frequency with which the four forms of accountability were sought by complainants in the study sample. The vast majority (87%) of conciliated complaints included a request for restoration. Other complaints research has identified this as an important outcome for many patients and their families, particularly those who have suffered serious financial consequences as a result of medical injury.2
Remedies sought in complaints regarding informed consent in Victoria (n=218)
However, restoration stood alone as a remedy sought in only 25% of the informed consent complaints in our study. This finding resonates with previous research from New Zealand,2 the UK,1 the USA,26 and The Netherlands14 showing the considerable weight patients place on non-monetary remedies following adverse outcomes.
Over half (57%) of complainants sought communication in the form of information about what had happened in the care breakdown, an expression of responsibility, or an apology. The desire for information and better communication is well established as a common motive for initiating medico-legal action.1 2 27
Nearly half (46%) of all claimants sought corrective action to reduce the risk of harm to future patients. As a motivator of medico-legal action, the sentiment that that ‘this should never happen again’ has received much commentary,7 28 but only a few empirical studies have quantified its prevalence.1 2 14
Less than one-fifth (17%) of complainants sought sanctions (in the form of disciplinary action or other punitive measures) against specific individuals or organisations.
Remedies obtained
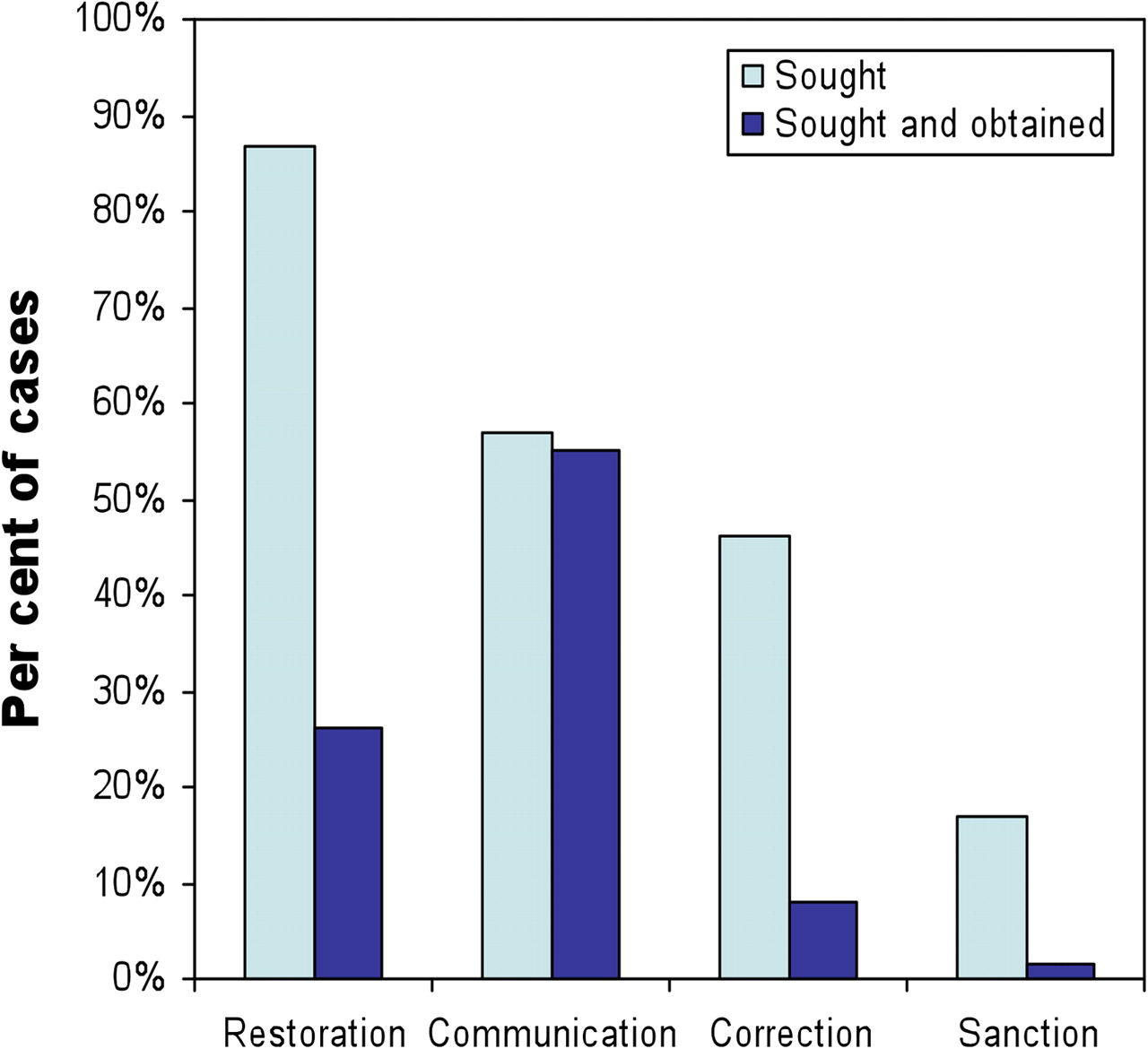
Nearly all patients who sought communication got it (figure 1). This result was somewhat preordained by the fact that, regardless of what patients sought, 94% of all complaints delivered a communication-related remedy. This is because the complaints resolution process is essentially built around facilitating communication between the parties to a complaint. When a complaint is first received, staff will usually encourage the complainant to discuss his or her concerns directly with the health service provider involved. If that is unsuccessful in resolving the matter, written correspondence from the Commissioner's office may follow, inviting the provider to respond to the complaint. If the complaint is still unresolved, mediation or conciliation may follow, which the main parties typically attend (and all of the complaints in our sample went to conciliation). At any of these points in the process, complainants may receive additional information about what happened to them and why, answers to their questions and perhaps an apology.

{kind=link}
Remedies sought and obtained in a sample of informed consent complaints in Victoria (n=218).
By contrast, a large ‘expectation gap’ was evident in relation to the other three types of remedies. A third (59/189) of complainants who sought restoration received it; 1 in 5 complainants (17/101) who sought correction received assurances that changes had been or would be made to reduce the risk of others experiencing a similar harm; and fewer than 1 in 10 (3/37) who sought sanctions saw processes to achieve this outcome initiated.
Implications of the expectations gap
Of all dimensions of complainants' experiences, the outcome may be the strongest determinant of overall satisfaction.18 Summers and Granbois have described consumer dissatisfaction as “a function of the comparative level of consumers' expections and their actual experiences of goods and services”.29 Our study suggests that, in the field of health care, an expectations gap between the remedies sought and achieved by complainants may contribute to dissatisfaction with dispute resolution processes.
This focus on outcomes must be tempered by recognition that, while complainant satisfaction is important to commissions, it is not their only priority and they are not patient advocates. When the views of complainants are at odds with those of healthcare providers, as commonly occurs, commissions must play the role of honest broker and facilitate an outcome that is fair to all parties.
Limitations
Our data has several limitations. First, the complaints we examined involved conciliated disputes over informed consent in Victoria; the findings may not be generalisable. Because problems in the informed consent involve communication breakdowns, the proportion of cases seeking improved communication may be higher than other types of disputes. However, the generalisability of other aspects of our findings to other types of disputes, or to dispute resolution agencies in other states or countries, is not known.
Second, because the remedies that form the focus of our analysis came from retrospective reviews of written documentation, they are crude in some respects. For example, complainants may have ‘unspoken’ expectations, and certain outcomes of conciliation may not have been recorded in the conciliator's final report. Third, we recorded only the presence or absence of various remedies obtained, not qualitative aspects of their nature (eg, the completeness of an explanation, sincerity of an apology, or adequacy of a payment), which undoubtedly affect the extent to which patients' expectations are met. Finally, the remedies sought by complaints were determined by statements made at the time they first lodged their complaint. Some complainants' expectations are likely to have changed during the resolution process, as they gained a clearer picture of what happened or of the feasibility of certain remedies. The likely effect of constraints on our inability to observe these three aspects of complaints (hidden preferences, degrees of preference satisfaction and changing preferences) on the expectations gap identified in our findings is unknown. Nonetheless, it seems implausible that accounting for these factors would eliminate all or even most of the divergence between remedies sought and obtained.
Conclusions
Characterisations of discontented patients as ‘greedy, angry and eager to sue when medical error occurs’ miss the mark30; they do not match the complex mix of factors that motivate patients and their families to seek medico-legal redress. In the Australian healthcare system, health complaints commissions offer the broadest range of remedies and, ostensibly, are well placed to meet the heterogeneous expectations of patients who are dissatisfied with their care.
However, this breadth and flexibility is a double-edged sword. Patients' baseline expectations on entering complaints systems may be high, and sometimes unrealistic, creating ample scope for dissatisfaction when commissions either do not have authority to meet those expectations or determine that doing so in the circumstances at hand would be inappropriate. Such ‘discordant’ outcomes may cause anger and frustration, and may lead to disillusionment with the complaints system. Our findings suggest that many complainants find, despite the range of remedies mentioned on commissioners' websites, that ‘you can’t always get what you want'.
There are two logical ways in which this expectation gap can be narrowed: by delivering to more complainants the remedies they are seeking and by decreasing unrealistic expectations.
The first tactic requires an improved understanding of what complainants want. Frontline staff who handle complaints should be closely attuned to patients' and families' motives for complaint. Without this understanding, satisfaction of preferences will be a fluke. Next, wherever possible, the remedies a complainant prizes should be articulated and carefully considered during the complaint resolution process. In cases where, for example, corrective measures could be taken, the desired outcome should not be denied simply because no-one considered whether lessons could be learnt.
On the other side of the divide, there must be clear-eyed recognition within complaints agencies of the fact that, for many complainants, the complaints resolution process will not—and sometimes cannot—deliver the remedies patients and their families seek. For example, commissions have no statutory power to sanction errant doctors and few cases are referred on for consideration in disciplinary proceedings. A dose of reality should be administered early in the process to help manage expectations and avoid unnecessary distress and disappointment. (In Victoria, for example, Commission staff strive to identify and discuss unrealistic expectations early on.)
When complaints are poorly handled, there are real risks of worsening relations between patients and providers and extinguishing opportunities for corrective action.21 25 Complaint management techniques that identify and take seriously the remedies complainants are seeking, and then coach them from an early stage through the range of feasible outcomes, could go far in bridging the expectations gap and improving satisfaction with healthcare complaints resolution processes.
Acknowledgments
The authors thank Beth Wilson, the Health Services Commissioner of Victoria, and Grant Davies, the Deputy Commissioner. Without their support and the assistance of their team in preparing the data, this study would not have been possible.
References
Footnotes
Linked article 000343.
Funding This study was supported by a Linkage Grant from the Australian Research Council (LP0989178), with partner contributions from the Office of the Health Services Commissioner of Victoria and Avant Mutual. DMS was supported by a Federation Fellowship from the Australian Research Council.
Competing interests None.
Ethics approval This study was conducted with the approval of University of Melbourne Human Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.