Article Text

Abstract
In a time of financial uncertainty and structural reform, the National Health Service (NHS) in England needs clinical leadership to help improve the quality of patient care. Increasingly, leadership development is being targeted at doctors in postgraduate training to help prepare them for their future leadership roles as consultants and general practitioners. However, there is a risk that we are missing an opportunity here by failing to recognise the role that doctors in training can play now, during their training. As our frontline clinicians they have a unique view of the health service and the inefficiencies therein. The London Deanery has been running an educational programme called Beyond Audit to provide doctors in training with quality improvement skills. During this programme we have been given a unique insight into NHS systems as viewed by junior doctors. They have identified a wide range of small system problems that, when combined, result in large-scale inefficiency and prevent the delivery of high quality patient care. These problems they identify have implications for cost, efficiency, patient safety, team-working and patient experience. Any attempt to improve the quality of care delivered in the NHS needs to look at the system from the point of view of those delivering the care, including our doctors in postgraduate training. By empowering them to make improvements to the systems that they see, there is the potential to make significant improvement in the quality of patient care that they deliver.
- Quality improvement
- graduate medical education
- leadership
- patient safety
- paediatrics
- medical education
Statistics from Altmetric.com
Introduction
There is no doubt that the National Health Service (NHS) in England is currently facing great change. The financial challenges and proposed structural changes bring with them an urgent need to focus on improving quality and value in the care that we deliver. At every level, managers and clinicians must make changes to improve the safety, efficiency and effectiveness of healthcare in the UK. A Quality, Innovation, Productivity and Prevention (QIPP) agenda1 has been developed to try and meet the ‘Nicholson Challenge’ of achieving £20 billion of efficiency savings. A new system of financial incentives has been developed in the form of Commissioning for Quality and Innovation (CQUIN)2 allowing health communities to develop their own schemes to support local quality improvement. At the same time, there is considerable investment in developing clinical leadership to enable the clinicians who deliver the health service to engage with the finances and structures that make that delivery possible.
Within all this, there is an increasing focus on our doctors in postgraduate training to lead or participate in change within the NHS. This was emphasised by both Lord Darzi3 and Sir John Tooke4 in 2008. The Medical Leadership Competency Framework5 and the General Medical Council's Good Medical Practice framework for appraisal and revalidation6 both emphasise the need for doctors to demonstrate participation in quality improvement. That our trainees are the clinical leaders of the future is clear, but are we making the most of their skills now?
Doctors in training: an underused resource?
Junior doctors are in a unique position in the health service. They move from Trust to Trust within the NHS and are responsible for the delivery of much of our acute healthcare (the Tooke Report4 suggested that 80% of ward-based activity is carried out by doctors in training). They are often the first persons to see a patient in a hospital and it is usually their early decision making that determines that patient's initial care. It is often their actions that determine when a patient is discharged or which drug is prescribed—decisions that can have a significant impact on efficiency and cost. They are highly educated and motivated individuals but are we making the most of their potential?
It is well known to doctors that August is a bad time to be unwell.7 Many junior doctors are changing posts and the hospitals are staffed with inexperienced trainees who may not know how local systems work in their new organisation. One assumes that NHS Chief Executives have sleepless nights at this time. But with changes to training aimed at increasing supervision and patient safety, we can imagine a future where the Chief Executives are awake with a different fear; a fear that an army of change agents will be entering their organisation, bringing experiences from nearby hospitals. These new arrivals will challenge the inefficiencies they encounter in their new workplace. They can bring experiences of safer services and will question inefficient systems. They will see the service from their unique perspective and will not be afraid to raise uncomfortable issues. Is this just an idealistic pipe dream?
Lessons from the frontline
Over the past year, London Deanery has been running a programme called ‘Beyond Audit—junior doctors leading for quality’. This scheme focuses on the much reviled trainee role in clinical audit and aims to support trainees in moving from meaningless data collection to managing lasting change. At workplace-based workshops, trainees are introduced to quality improvement theories and tools. They are then encouraged to think about the inefficient systems they encounter in their daily work; those ‘treacle-wading moments’ that prevent them from doing their job well. The workshops include developing these ideas into quality improvement projects that can be put into action.
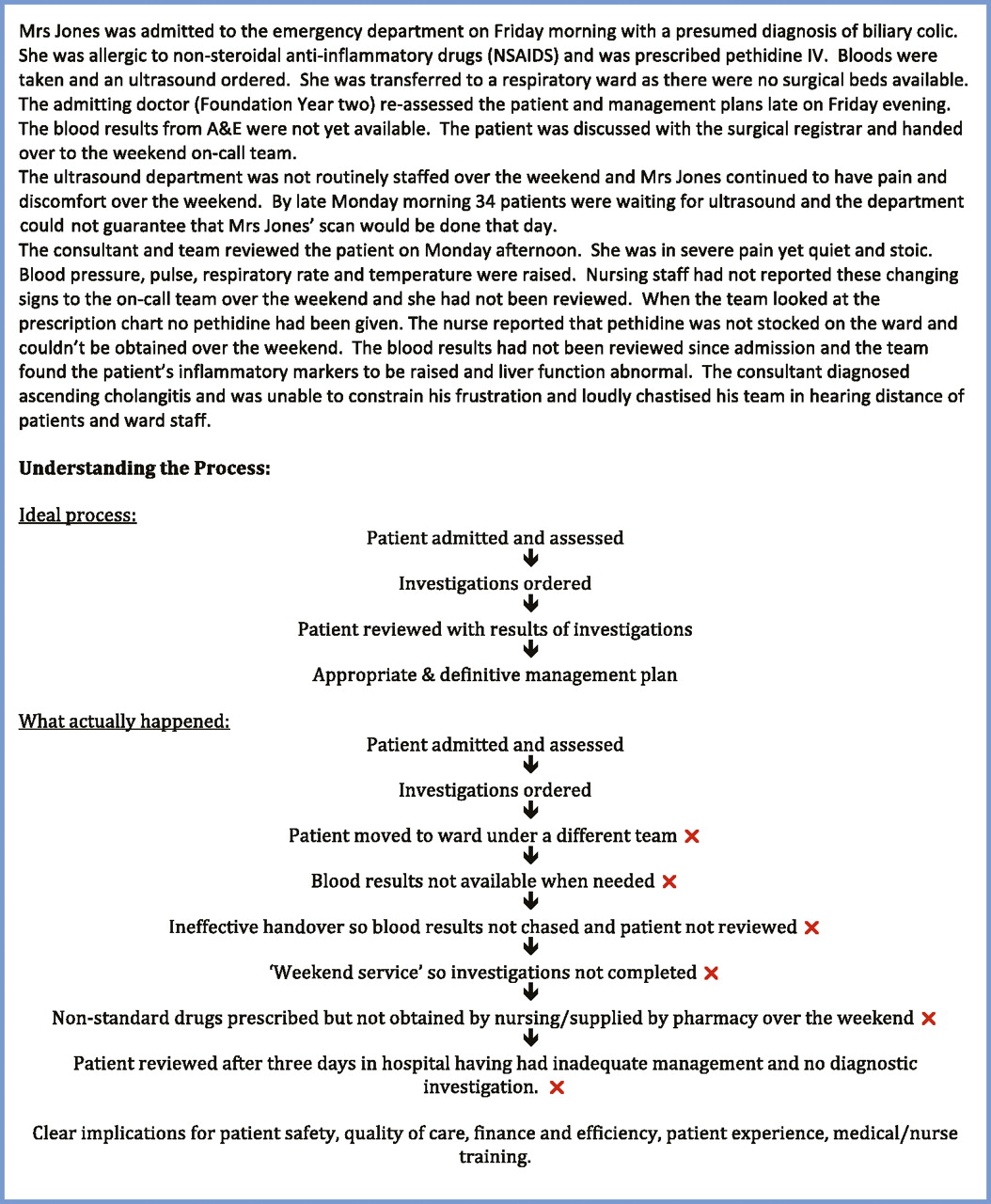
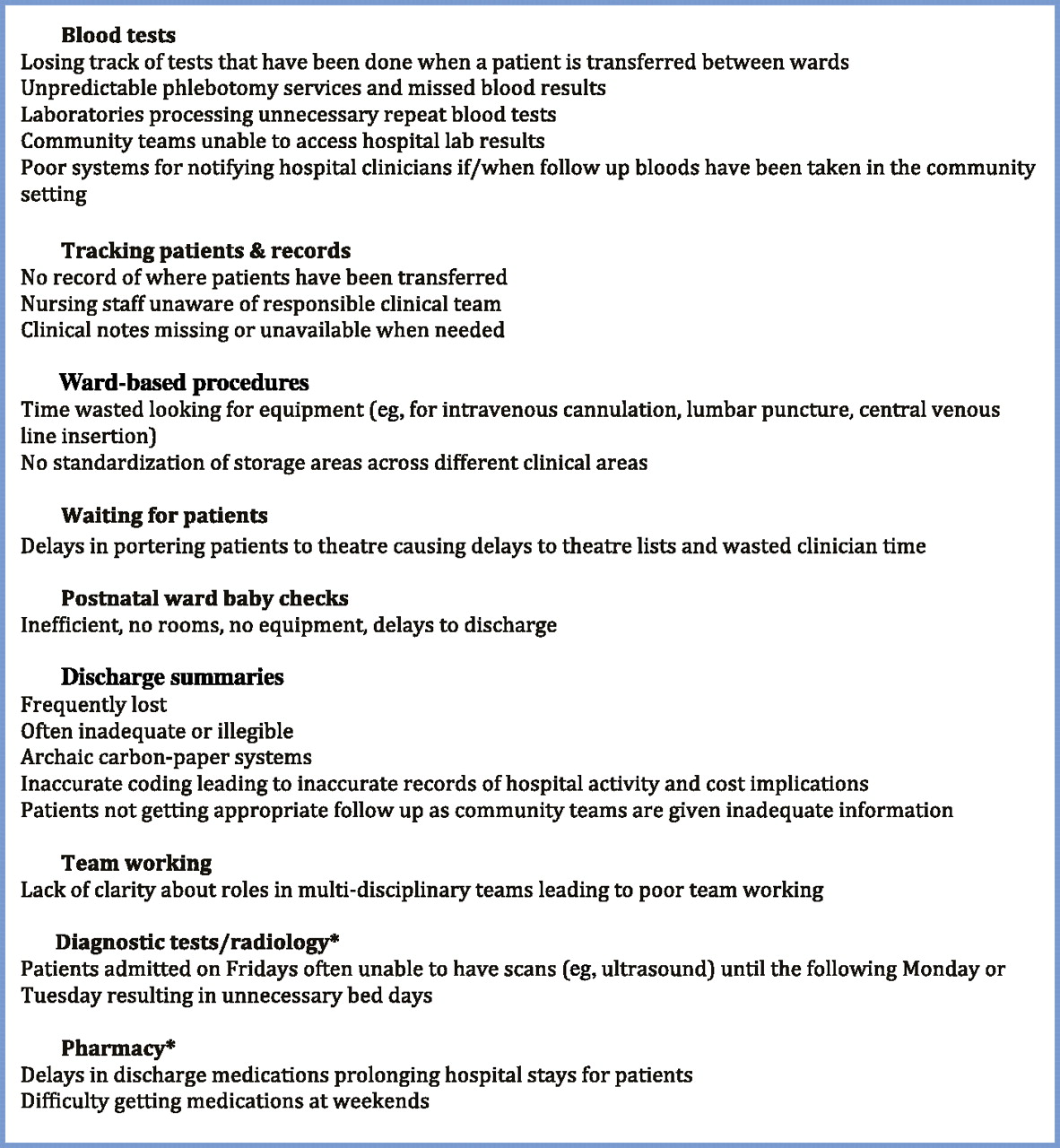
Since March 2011 we have run 26 workshops across London, reaching over 380 trainees. We have been amazed by the enthusiasm of the trainees and their readiness to challenge inefficient systems and start making changes. We have also had an unparalleled insight into the common problems that are faced by junior doctors in their work; the myriad small system problems that lead to wasted time and immense frustration. We have also been impressed by the ingenuity and resourcefulness that goes into ‘workarounds’ to avoid system problems. Figure 1 shows some of the problems that junior doctors are facing on a regular basis. Figure 2 shows an example case study demonstrating the impact of these inefficiencies on patient care. Each of the crosses indicates an area for a potential junior doctor-led quality improvement project.

System inefficiencies as identified by doctors in postgraduate training. *Problems specifically related to the inconsistency of providing key services in ‘working hours’ only (9:00–17:00, Monday to Friday) within a 24-hour, 7-day-a-week hospital service.
{kind=link}
{kind=link}
Case study highlighting the impact of inefficient systems on patient care. The crosses highlight the inefficient steps in the process that are amenable to junior doctor-led quality improvement projects. They correspond to the types of problem identified by doctors in training during the ‘Beyond Audit’ workshops (figure 1). Some of the problems will be easier to tackle than others. Junior doctors may need support from senior clinicians to help them choose achievable projects or to help them understand the wider impact that system changes might have.
Minor irritations or a bigger problem?
The problems listed are problems that are coming up recurrently in training workshops. Whilst the idiosyncrasies may be hospital-specific, the fact that the same problems occur across NHS Trusts points to a wider system problem. Whilst a poorly stocked phlebotomy trolley might not be a major priority for an Executive Board, these inefficiencies have serious implications for daily clinical care.
Cost implications
With the need to make financial savings in the NHS a high priority, a financial case can be made. Our trainees estimate that they are wasting an hour a day looking for clinical equipment. The current 2011/2012 payscales for junior doctors range from £25 000 to £65 000.8 A trainee in the second year of Foundation Training working a ‘band 2B’ rota can expect to be paid £44 000 pa. Working a 48-hour week over a year, this equates to an hourly rate of approximately £18/h. At the top of the payscale this is £26/h. With up to 750 trainee doctors in some of the larger NHS Trusts, all wasting an hour a day looking for equipment, a Trust could be losing £54 000–78 000 per week in wasted salaries (based on a doctor working an average of four 12 h days a week).
Efficiency
The efficiency of a hospital depends on many factors, including the throughput of patients through the service. Our trainees consistently report that patients are left waiting for discharge from hospital or to be seen in a clinical setting. It is often the junior doctors that need to complete the paperwork to admit/discharge a patient and so if they are held up in other unnecessary tasks this can lead to patient delays. In many cases, those in charge of the service many not be aware of how their junior colleagues are spending their time. Giving junior doctors a means to demonstrate the inefficiencies in the process and the tools to start improving this could have a dramatic effect on efficiency across the whole system.
Patient safety
Our trainees have consistently highlighted problems with missed blood results for inpatients. This may result from problems with the phlebotomy process or may be due to patients moving through healthcare settings. A recent review9 supports our trainees' observations that missed test results are a significant problem in healthcare services. The implications are significant for patient safety; missed diagnoses, inaccurate drug monitoring, unnecessary repeated tests will all have a negative impact on patient care. If our trainees are aware of this as a problem, how are we helping them change the system?
Timeliness
Another recurrent theme is the difficulty in accessing certain key services (most notably pharmacy and radiology) ‘out of hours’, There are many services within hospitals that are provided within working hours, that is, 9:00–17:00, Monday to Friday. This may pose problems for patients admitted to hospital on a Friday evening or over a weekend or public holiday. Patients may not be able to access important investigations or medications, thus delaying their care and prolonging their hospital stay unnecessarily. Junior clinicians are often chastised for failing to obtain a crucial investigation for a patient when, in fact, it is the inconsistent provision of services within the hospital that is at fault. Senior clinicians and managers who are not in the hospital ‘out of hours’ may be unaware of the impact of this problem.
Team breakdown
There is evidence that effective team working is key to high quality patient care.10 Yet our junior doctors report that team roles are often unclear and over-worked staff fall out over division of work. We have come across many instances of junior doctors and nursing staff being unable to identify who is responsible for a particular step in a patient pathway. As well as being inefficient and symptomatic of a poorly designed clinical system, this undermines effective team working.
Patient experience
The problems our trainees are seeing have a significant impact on their patients. Lost notes and results have both patient safety implications as well as leading to wasted time and unnecessary duplications. For patients with chronic conditions and multiple contacts with healthcare, every delay is disruptive to their lives. In all cases it makes the provider appear inefficient and can damage faith in the health service. It is our front-line clinicians who usually have the first and the most frequent contact with patients in hospital settings. In designing care that is patient-centred, we need to listen to and address the concerns of these clinicians in order to ensure that their patients are getting high quality care.
Quality care
It seems to us that our junior doctors are identifying multiple small system problems that stand in the way of high quality patient care. The Institute of Medicine defines ‘quality in healthcare’ as care that is safe, timely, efficient, effective, patient-centred and equitable.11 Yet the variation in the system and the stumbling blocks of poorly designed pathways are clearly preventing quality care from being delivered.
Whose problem is this?
Echoing the lack of clarity over roles in clinical teams, it is not always clear who should be responsible for fixing the system. Managers see a clinical system that they don't understand. Doctors see a ‘system problem’ and hope that managers will sort it out. The result is a series of complex workarounds and no one fixes the problem. Both doctors and managers may hope that a wider system change will come from ‘above’ and solve the problems.
Whilst we can wait for the big system changes, history shows us that is slow and may not work. Instead we need to listen to the problems from the frontline and support our clinicians to use their understanding of the service to make improvements. The concept of multiple small tests of change to improve a system is not new12 13 and needs to be embedded in our NHS. Toyota famously empowers every member of its staff to stop the whole production line if there is an error or problem. We need to be giving our frontline clinical staff the same power.
What can we do?
A first step in fixing these problems is to give the skills and recognition to the junior doctors to enable them to get involved in quality improvement. We must support their improvement endeavours and value and celebrate their successes. Increasing numbers of projects across the country are demonstrating that junior doctors can be highly effective in improving healthcare services. As well as the ‘Beyond Audit’ project in London, programmes such as the Royal College of Physicians ‘Learning to Make a Difference’,14 Doctors Advancing Patient Safety (DAPS)15 and other deanery-based programmes across the UK are providing training for junior doctors to undertake quality improvement projects. There is further support from medical communities such as ‘The Network’16 and ‘BMJ Learning’ to support junior doctors and their educational supervisors. A recent edition of Junior Doctor magazine focused on junior doctor-led quality improvement projects and included a ‘How-To’ guide for doctors in training.17 We must continue to build on these excellent endeavours and embed junior doctor-led quality improvement throughout the NHS.
The Beyond Audit workshops have highlighted huge enthusiasm from junior doctors to undertake improvement work. Where we have been able to demonstrate this enthusiasm to managers, they have had their eyes opened to a new resource. It is clear that this kind of work cannot be done by doctors or managers alone—they need to work together. The pairing of junior doctor with a manager can be hugely powerful. This has been demonstrated by some of the buddying schemes emerging across the country.18 If we can nurture effective working relationships between clinicians and managers from an early stage in training then perhaps we can develop a culture of grassroots improvement and innovation in the NHS and start to deliver care that is truly high quality.
Conclusion
Through delivering an educational programme to junior doctors, we have been able to highlight the unique insights into the workings of the NHS that our frontline colleagues can provide. In helping them to examine clinical systems, we have enabled them to describe the healthcare systems that they encounter. Far from being safe, efficient and effective systems, the systems they describe raise serious concerns. Yet, until recently, junior doctors have not had the voice or the language to raise these concerns effectively. The daily inefficiencies that these clinicians encounter, the moments that make them feel that they are wading through treacle to get their work done, are significant in preventing them from delivering high quality care. Additionally, we are aware that nursing and associated health professional colleagues face these problems too.
We can wait for large system changes to magically sweep away these problems, or, realistically, we can help develop our frontline clinicians to be ‘agents for change’. If we give them the right tools and knowledge and nurture their relationships with management staff, we can enable them to make the most of their unique understanding of the health service and bring about real change and improvement to patient care.
Acknowledgments
We would like to acknowledge the input of all the doctors in postgraduate training who have taken part in the Beyond Audit programme and contributed their insights to the NHS.
Footnotes
Funding The ‘Beyond Audit’ programme has been funded by the London Deanery.
Competing interests None.
Ethics approval This is a retrospective observation of a training programme, not a study.
Provenance and peer review Not commissioned; internally peer reviewed.