Article Text

Abstract
Problem Research has demonstrated a knowledge and practice gap in the identification and management of chronic kidney disease (CKD). In 2009, published data showed that general practices in Greater Manchester had a low detection rate for CKD.
Design A 12-month improvement collaborative, supported by an evidence-informed implementation framework and financial incentives.
Setting 19 general practices from four primary care trusts within Greater Manchester.
Key measures for improvement Number of recorded patients with CKD on practice registers; percentage of patients on registers achieving nationally agreed blood pressure targets.
Strategies for change The collaborative commenced in September 2009 and involved three joint learning sessions, interspersed with practice level rapid improvement cycles, and supported by an implementation team from the National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care for Greater Manchester.
Effects of change At baseline, the 19 collaborative practices had 4185 patients on their CKD registers. At final data collection in September 2010, this figure had increased by 1324 to 5509. Blood pressure improved from 34% to 74% of patients on practice registers having a recorded blood pressure within recommended guidelines.
Lessons learnt Evidence-based improvement can be implemented in practice for chronic disease management. A collaborative approach has been successful in enabling teams to test and apply changes to identify patients and improve care. The model has proved to be more successful for some practices, suggesting a need to develop more context-sensitive approaches to implementation and actively manage the factors that influence the success of the collaborative.
- Chronic disease management
- healthcare quality improvement
- general practice
- evidence-based medicine
Statistics from Altmetric.com
Context
Chronic kidney disease (CKD) is common, affecting around 5%–10% of the adult population. CKD stages 3–5 represent moderate to severe disease and ascertainment of these stages has been included in the National Health Service (NHS) Quality Outcomes Framework since 2006/2007. These stages fall into a classic pyramid stratification of chronic disease1 with around 97% of patients in stage 3 disease,2 at which point patients tend to be asymptomatic from kidney disease and at least 10 times more likely to die, have a cardiovascular event or experience hospitalisation over 5 years than progress their kidney disease beyond stage 3.3 In all, 1.3% of patients in stage 3 disease will have end-stage kidney disease (ESKD) at 5 years.4 The percentage from stage 4 disease is 19.9%. The costs of ESKD are extremely high; 5-year survival on haemodialysis is worse than many cancers unless transplanted, the treatment regime is very burdensome and costs are for life. During 2008/2009, £1.3 billion or around 1.4% of the NHS budget was spent treating only 0.05% of the general population for ‘renal problems’.5 Secondary care accounts for 94% of total expenditure in this area.
The National Institute for Health and Clinical Excellence (NICE) developed guidelines for CKD in 2008, which aimed to promote earlier detection, intervention and prevention or delay of complications including ESKD. Careful economic analysis was performed to underpin the guidance which concluded that case finding in patients with diabetes or hypertension or aged over 55 years would identify up to 93% of CKD patients at stages 3–5.6 However, research in general practice has demonstrated potential barriers to achieving such evidence-based guidance in practice, including, for example, acceptance of CKD as a disease state in older people, knowledge gaps in monitoring, treatment and referral, concerns about anxiety generation by applying a chronic disease label to asymptomatic individuals, and inadequate time to deal with CKD in addition to other long-term conditions.7
Outline of the problem
At the start of the project, research findings2 and Quality Outcomes Framework data from Greater Manchester8 suggested a gap of around 2% between the recorded local prevalence and estimated national average prevalence of CKD, equating to around 41 000 undetected cases of CKD in Greater Manchester. The same data also demonstrated that of those diagnosed, some 30% were not receiving optimal disease management, such as monitoring of their blood pressure or testing for proteinuria.
Life expectancy at birth in Greater Manchester is one of the lowest in the UK9 and addressing health inequalities in vascular diseases is one step towards improving this. This is the focus of activities within the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care (CLAHRC) for Greater Manchester (GM), which is one of nine national initiatives established as collaborations between universities and the NHS to tackle the known gaps between evidence and practice. Its mission is to address health inequalities in vascular diseases (CKD, stroke, diabetes and heart failure) by conducting and implementing applied health research in the primary care trusts (PCTs) within Greater Manchester.
Practices from four of the 10 PCTs (NHS Stockport, NHS Salford, NHS Bolton and NHS Ashton, Leigh and Wigan (ALW)) were invited to participate in the project. Practices were selected to reflect a range of list size and CKD prevalence at baseline. The list size across practices ranged from 3248 to 12 274 patients, while the prevalence at baseline varied from a starting point of 1.5% up to 8.8% of the 18+ practice register.
Key measures for improvement
An expert faculty was formed to agree on the scope and aims of the collaborative, drawing on available evidence, such as the NICE guidelines on the identification and management of CKD. The faculty contained a mixture of patient representation, secondary and primary care experts, local primary care opinion leaders and improvement leaders. The faculty established two key objectives for the collaborative, namely, to halve the gap between recorded and estimated prevalence for each practice and for 75% of all CKD patients to have their blood pressure managed to targets recommended by NICE guidelines. A secondary measure was the number of CKD patients tested for proteinuria. The CKD specific guidelines from NICE recommend tighter blood pressure control for patients with CKD and proteinuria of <130/80, while CKD without proteinuria should be managed within <140/90.
Process of gathering information
Participating practices submitted data on a monthly basis. These data recorded the number of patients on the CKD register, the number tested for proteinuria, the number who had a result coded as positive or negative, and the number of patients meeting targets for blood pressure control (with and without proteinuria). The process of capturing the monthly data was completed by a member from each improvement team using searches carried out on their inpractice clinical systems. Each team submitted their practice data to their assigned CLAHRC improvement facilitator.
Analysis and interpretation
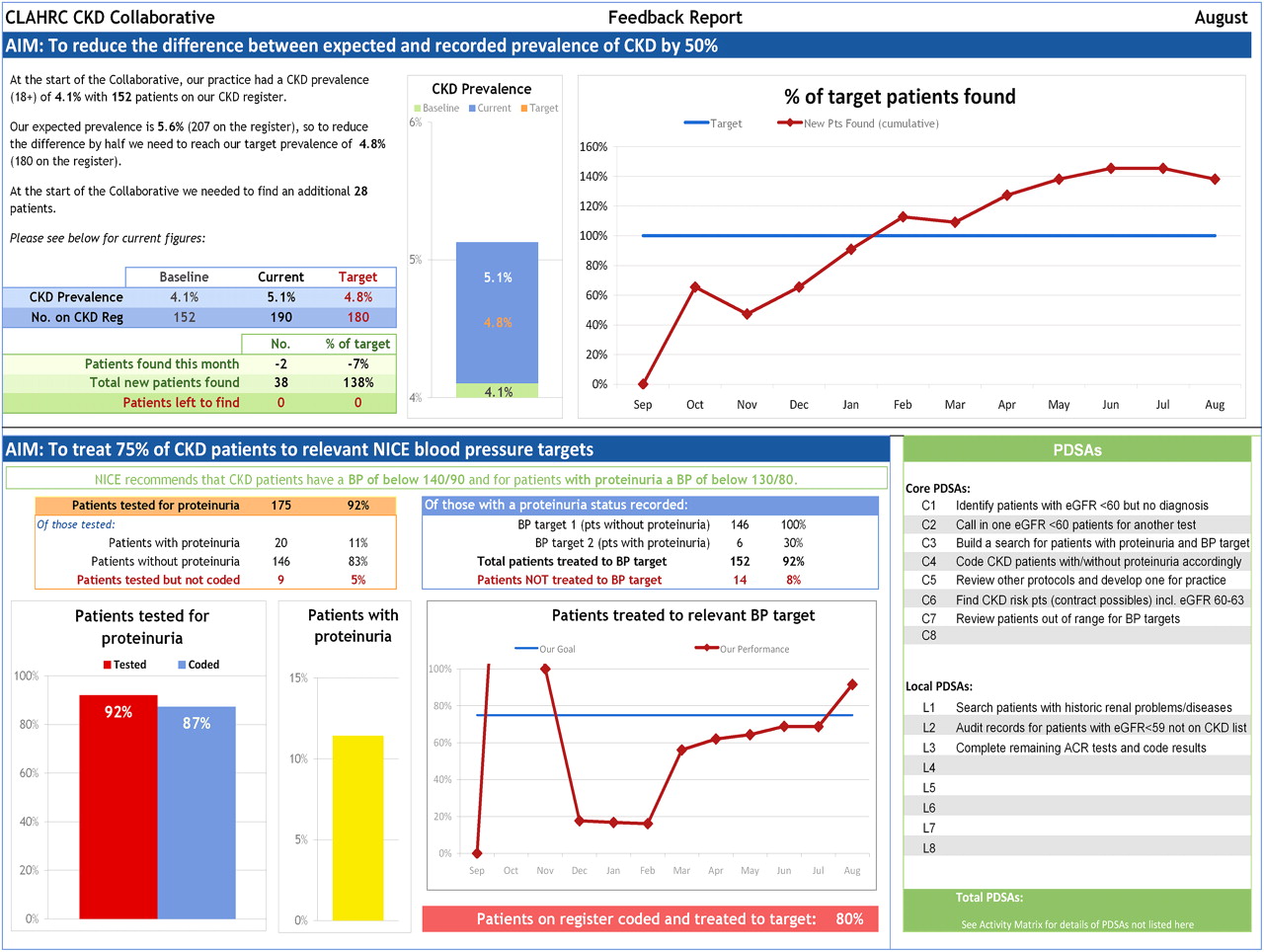
Data that were submitted by the practices to the CLAHRC project team were analysed and reported on a monthly basis. Data were presented back in a number of ways. At an individual practice level, run charts were used to present progress on the key indicators over time, alongside guidance on successful improvements, areas for development and useful comparatives with other practices within the collaborative. To increase the shared learning element of the collaborative, monthly practice feedback and dashboard reports (see figure 1) clustered by PCT were also presented back to the teams and made available for online viewing. This allowed teams to track their own progress against their peers. At the start of the collaborative, all the practices agreed that practice names should be unblinded for the duration of the collaborative, which enabled them to seek information or advice from other practices where appropriate. The clustering of progress by PCT also helped the CLAHRC to identify common trends within each area.

Example of a practice-level feedback report. CKD, chronic kidney disease.
The CLAHRC project team met on a monthly basis to review progress at a practice and PCT level. By assessing the data and comparing the progress of practices in relation to each other, strengths and weaknesses of each practice were identified to help facilitate focused improvements. Previous research on the factors known to influence the success of improvement initiatives in healthcare was used to inform these discussions and plan strategies to accelerate improvement in some of the lower performing practices. In particular, the project team applied the framework developed by Bate and colleagues,10 which suggests that the improvement trajectory of organisations is influenced by their ability to address six core challenges, namely, structural, political, cultural, educational, emotional and physical/technological challenges. Box 1 provides an example of the discussion and analysis at the monthly CLAHRC project team meetings to assess progress of individual practices and strategies for future facilitation support.
Example of practice level review at monthly CLAHRC project team meeting

Strategy for change
The GM CLAHRC has developed an approach to implementation that recognises the complex, multi-faceted process of translating research evidence into practice.11 Key building blocks of the CLAHRC implementation strategy include the Model for Improvement11 and the PARIHS framework,12 which proposes that the successful implementation of research evidence into practice is dependent on the complex interplay of the evidence to be implemented, the context in which the implementation is to take place and the way in which the process is facilitated (how and by whom). This wider perspective on implementing evidence-based practice provided a framework within which the improvement collaborative was designed and run, as outlined below.
The improvement collaborative itself was based on the breakthrough collaborative model, with its key elements of joint learning events and practice-level action periods.14 Over the 12-month collaborative, three learning sessions and a concluding summit event were held. In between learning events, improvement teams at each practice used Plan, Do, Study, Act (PDSA) rapid improvement cycles to test and apply changes. Each team was typically made up of a lead GP, a practice nurse and a practice manager to reflect the multi-professional nature of the changes to be made and the need for effective teamwork to make improvements. Practices were recompensed as part of the implementation strategy in order to secure protected time for the teams to carry out the improvement work and to cover the costs of attending learning sessions and also received a financial incentive for completing key stages of the collaborative. This involved each practice receiving an initial payment for baseline data collection, and three subsequent payments after attendance at each of the learning sessions. These three scheduled payments covered time out for attending the learning session and time spent by teams during action periods to implement the improvement work. Each practice was issued a final payment (between £500 and £1250) at the close of the project; the exact amount awarded was based on achievement against the key improvement measures. Table 1 summarises the costs associated with running the improvement collaborative.
Summary of costs associated with the improvement collaborative
Drawing on the key elements of the CLAHRC implementation model,11 a number of other strategies were employed to support and enhance the improvement collaborative. For example, to provide local, tailored facilitation, which has been shown to be important for successful implementation,15 improvement teams received regular site visits between learning sessions. These visits were made by two improvement facilitators, employed by the CLAHRC, who provided help with data searches and management, process mapping and design, project management and teamwork development. Recognising the impact of context on implementation and improvement,16 the facilitators also supported local practices to complete an assessment of their local context to identify any potential barriers to implementation, for example, issues relating to organisational culture, leadership, team work and communication.17 These assessments were used to plan specific strategies required at a practice level to enhance the likelihood of successful implementation, for example, introducing regular meetings for the whole practice team, making clinical guidelines more accessible, developing ways to communicate the content of the guidelines and so on. To increase the scope for support for improvement work at a wider organisational context level, the CLAHRC team also engaged with senior stakeholders at each of the participating PCTs to give them regular updates on progress and encourage them to contact teams and recognise their achievements.
Effects of change
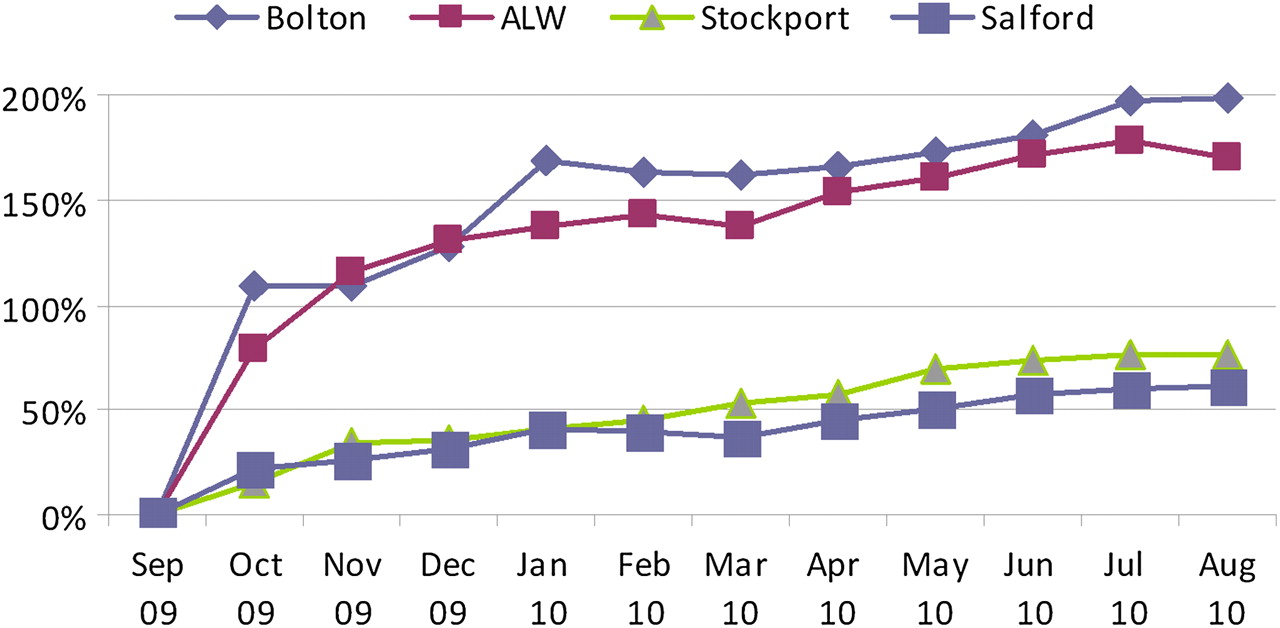
Overall, the 19 collaborative practices identified 1324 patients over 12 months, equating to 92% of the aim set (n=1441 patients). Ten of the 19 practices achieved their prevalence targets; however, there were wide variations in the level of achievement across the four PCTs (see figure 2). The highest PCT percentage prevalence achievement against target was 199%, and the lowest was 61%. The variation was further polarised at practice level with the highest achievement being 480%, and 40% being the lowest. Each PCT had a mix of practices and in each similar tests of change were tried. It is difficult, therefore, to account for the wide range of achievement against the prevalence targets, although some of the variation could be attributed to limitations in the prevalence modelling which does not account for variations in ethnicity and deprivation.

Prevalence achievement against target per PCT.
The aggregate improvement in prevalence in the collaborative practices across the four PCTs was 1.2%. During the same period, for comparison, the average improvement in prevalence for non-collaborative practices was sampled from two of the four PCTs (NHS Ashton, Leigh and Wigan and NHS Salford) and found to be 0.2%. If this level of improvement was replicated across all practices in the 10 Greater Manchester PCTs, we estimate that approximately 26 000 patients would be added to CKD registers (see figure 3).

Projections of number of patients found if a 1.2% increase in chronic kidney disease prevalence was repeated across Greater Manchester. QICKD, Quality Improvement in Chronic Kidney Disease;QOF, Quality Outcomes Framework; HMR, Heywood, Middleton and Rochdale; T&G, Tameside and Glossop; ALW, Ashton, Leigh and Wigan.
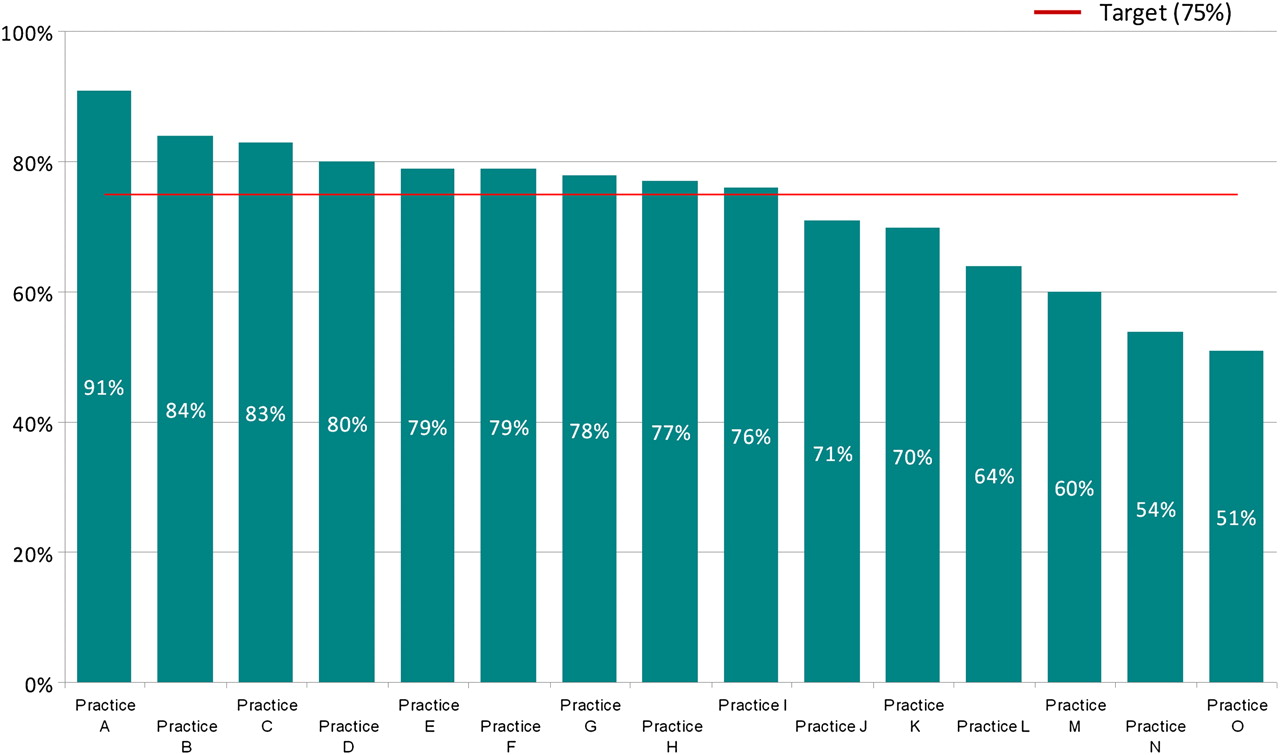
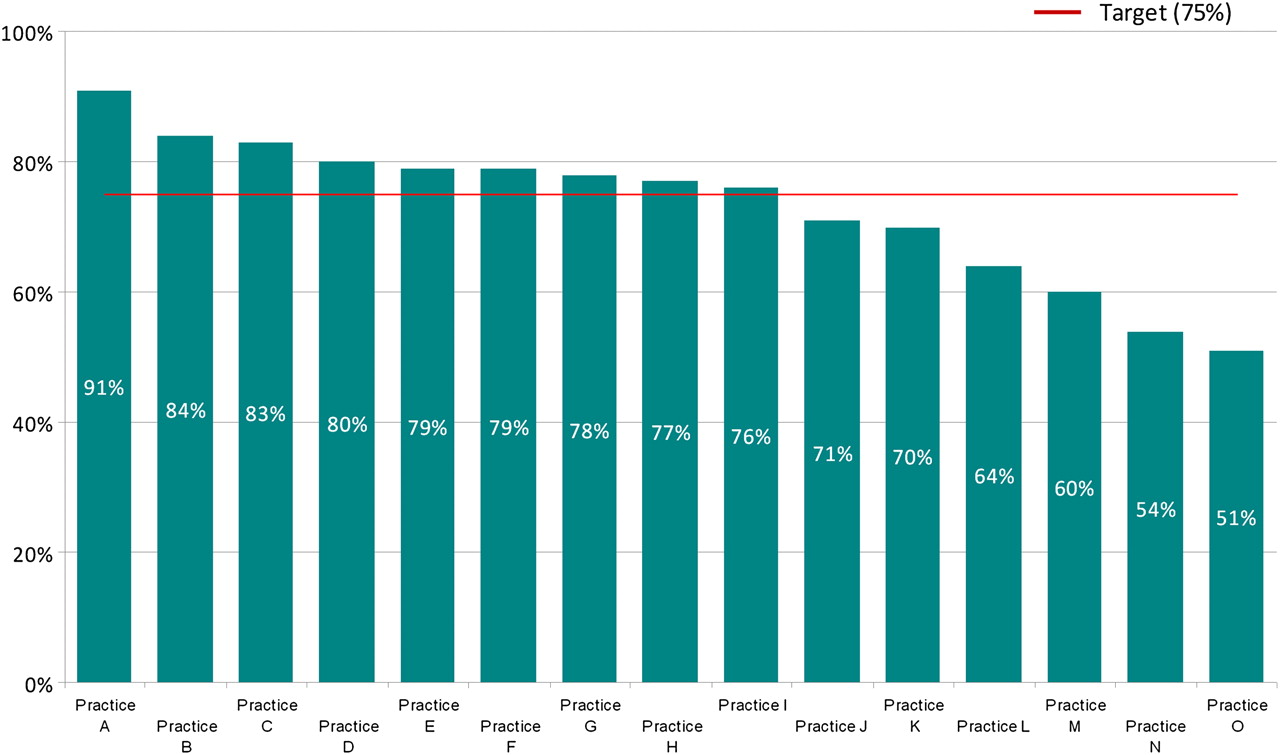
In relation to the second aim, an overall recorded improvement from 34% to 74% of patients on CKD registers being managed within NICE blood pressure targets was observed, the equivalent of up to 1800 patients experiencing better management of their blood pressure. The highest achieving PCT reached 81% of all recorded CKD patients meeting targets, the lowest 67%. Again, the variation in achievement was wider at practice level, ranging between 51% and 91% (see figure 4). Additionally, the data showed that only 23% of registered CKD patients had been tested for proteinuria in October 2009. By August 2010, this had improved to 78%.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Breakdown of spread in collaborative practices achieving blood pressure targets.
Although we were not resourced to perform a detailed cost–benefit analysis of the project, we examined sample data from two quarters to study the effect of participating in the collaborative on practice referrals, cognisant that in the short-term, initiatives to ‘find and treat’ chronic disease can incur additional costs. In one PCT, data from the participating practices showed a reduction by 43% of referrals into secondary care, with a resultant estimated saving of £48 000 per PCT per year, if replicated PCT-wide. This finding, along with the savings associated with better management of CKD and delayed progression of the disease to the highly resource intensive stage of dialysis, reinforces the findings from other studies which have demonstrated that interventions to improve detection and a more systematic approach to the management of CKD are cost effective.18
Lessons learnt
Overall, the improvement collaborative was largely successful in achieving the aims that were set. However, as the data illustrate, the rate of achieving the project aims varied considerably across the 19 practices. This is typical of the implementation of any complex intervention:19 ‘what works’ in one setting is rarely directly transferable to another setting, even within the same broad organisational setting, in this case a PCT. The collaborative model allows for flexibility so that specific changes can be tailored at a local level, using the PDSA approach. However, even with this flexibility, some practices were clearly more successful than others in implementing evidence-based changes for identifying and managing CKD; this despite the fact that all the practices were within the same regional area of the country and were subject to the same set of financial incentives and payments.
In order to better understand the reasons for this variation, we undertook process evaluation at the level of individual practices to examine local factors that might be impacting on the improvement project. This included asking practices to review and rate their own progress, informal interviews with practice staff and ongoing reflection about individual practice progress at monthly project team meetings. From this evaluation, a number of general lessons emerged (see box 2). These reinforce the findings from previous studies of improvement collaboratives,20 ,21 which highlight factors such as the importance of the topic for improvement being perceived as a priority, the need for measurable and achievable targets, senior leadership support and the need for a receptive and supportive context.
Lessons learnt during the collaborative
Benefits of learning sessions.
Important role of data feedback and benchmarking.
Importance of project aligning with local priorities.
Benefits of financial provision to buy out time for practice staff to participate in the improvement project.
Need to secure whole staff engagement, not leave all the work to some members of the improvement team.
Problems caused when there is senior staff opposition to the improvement project.
Problems caused by inadequate information technology (IT) systems or staff with poor IT skills.
Need for focused/directive facilitation, particularly in the early stages.
Benefits of undertaking a formal context assessment at the start of the project and using this to assess readiness to change and identify potential barriers.
It was notable that the shared learning element of the collaborative seemed to be effective and that the practices genuinely learnt improvement ideas from one another at the learning events. Data feedback processes and benchmarking—comparing at both PCT and practice levels within the collaborative—helped motivate practices and encouraged them to work together to increase overall progress. A common theme that emerged from the collaborative was a knowledge gap at the practice level and within the facilitation team around accurate data extraction from inpractice systems and at times this hindered the progress of the project in achieving its aims. As the collaborative progressed, practice teams and the improvement facilitators developed their knowledge and skills in this area, but the experience was very much one of learning by doing, supported by the PDSA method and regular input from the improvement facilitators. In this and other ways, the collaborative demonstrated that small PDSA cycles can be used as an effective tool within the primary care setting to facilitate effective changes and educate improvement teams around CKD. By testing the effects of change in a process in their practice environment, teams can measure the benefits that the change brings before deciding on whether and how to implement it on a practice-wide basis.
The feedback from practice teams suggested that the financial provision to buy out the improvement team's time to attend learning sessions and undertake improvement work at a local level during the action periods was important, particularly in the initial setup phases of the project. While the financial support provided did not completely cover the costs of the staff time spent on the work, it was helpful in securing commitment and offsetting some of the costs incurred. However, improvement work is often not a key priority in practices and it is important to ensure that improvement teams have the support from all staff to enable them to complete the work, including buy-in to the importance of the topic they are working on. Obtaining engagement from the whole staff team in a practice provides the improvement team with both emotional and logistical support to carry out the work. Those practices that faced staff opposition, particularly at a senior level, found the work significantly harder, despite the availability of financial support.
Next steps
The collaborative has proved to be a successful way to get practices working together to improve care. CKD registers have grown and improved in accuracy, and practices have more knowledge and confidence in managing the patients on these registers, as well as having newly developed skills in quality improvement. At the same time, as facilitators we have developed an increasing insight into the practical barriers and constraints that might limit the progress of improvement initiatives in primary care. Involvement in the collaborative has reinforced the importance of developing context-sensitive approaches to implementation and tailoring the facilitation strategy to meet local needs on a case by case basis.
As the collaborative progressed, the improvement teams typically focused on a number of key activities to implement the evidence around identifying and managing patients with CKD. These involved establishing the improvement team and processes at a practice level, validating practice registers, identifying patients with CKD, achieving optimal management of patients with CKD and introducing systems and processes to ensure that improvements were sustained once the collaborative came to an end. Learning from these different elements of implementation and from our reflections on the experience of the collaborative and the issues that practices had to address, we have distilled the lessons learnt into an improvement guide on closing the gap between evidence and practice for the identification and management of CKD in primary care (see box 3). This guide is being implemented and evaluated in a second phase of the project, working with a new set of practices, which commenced in March 2011. It is also available as an online resource for other primary care practices interested in improving the identification and management of CKD (http://clahrc-gm.nihr.ac.uk).
Improvement guide: implementing evidence-based changes to identify and manage patients with chronic kidney disease (CKD)
Creating a foundation for improvement
Establish a multi-professional improvement team in the practice: to make effective changes in practice, it is most suitable to have a complementary skill mix of staff from different disciplines within practice to fulfil the various roles required for improvement.
Assess the practice context and readiness to accept change: considering what potential blocks exist in each practice is the first step to resolving these and facilitating improvement.
Validate the CKD register: doing this standardises the register as a starting point removing patients coded incorrectly and coding those who have met the CKD criteria but are not coded.
Develop a practice CKD protocol: developing a protocol for all staff to follow should remove ambivalence, prevent incorrect coding and prompt that tests are followed up when appropriate.
Identifying patients with CKD
Identify patients with significant estimated Glomerular Filtration Rate (eGFR) results: before a protocol is developed, it is likely that many patients will have had tests showing low kidney function but not followed up. A search for patients with eGFR <60 will identify these patients for review.
Ensure that all high-risk patients have had eGFR tests: the National Institute for Health and Clinical Excellence suggests that a number of diseases cause a high risk to patients of developing CKD and that these patients should be considered for kidney function review. These are: hypertension, diabetes or cardiovascular disease, patients with a family history of stage 5 CKD or hereditary kidney disease or associated conditions such as polycystic kidneys, prostatic hypertrophy, structural renal tract disease or renal calculi and haematuria and proteinuria. This list is not exhaustive and other potential patients to be considered include those prescribed nephrotoxic drugs such as lithium.
Optimal management of CKD patients
Ensure that all patients have had a recent albumin-creatinine ratio (ACR) test: proteinuria is a significant additional risk factor for CKD patients putting them at a far higher risk of a cardiovascular event, all CKD patients should be monitored for this.
Manage blood pressure to recommended targets: good management of blood pressure relieves pressure on the kidneys and reduces the progression of CKD as well as lowering the risk for other cardiovascular events.
Encourage patients to get involved and self-manage: patients who are educated in the disease feel empowered and more able to control it.
Ensuring improvements are sustained
Involve and educate other staff: all staff at a practice need to understand the improvements that are made so that they can follow guidelines.
Develop systems for regular patient review: if patients are systematically recalled for reviews, the chances of a review date being missed are reduced. Audits will reinforce this resilience.
Ensuring CKD protocols are used in practice: if protocols are readily available to all clinicians, then they form a valuable point of reference and reduce the opportunity for error.
One challenge that could be made about the approach we have adopted is that it is too resource intensive to replicate more widely across a whole health system; the average per practice cost, including the external facilitation team and project management, was around £20 600. This funding was uniquely available via the NIHR and the NHS as part of a national programme aiming to reduce the research to practice gap. We would suggest, however, that a large proportion of the costs associated with this first phase are ‘setup costs’. With the learning and experience from the phase I project, we have been able to significantly reduce the externally provided costs of implementation in phase II, where the average practice payment is smaller, the length and cost of learning events have reduced and the amount of external support required is less. We also have access to improved analysis tools to reduce the time needed to search practice systems for appropriate patients. However, we do believe that there will always be costs associated with supporting the implementation of evidence-based practice. For the practice, the costs will largely be in the form of staff time to work on improvement initiatives and while the improvement guide that we have developed could be used independently by practice teams, there is evidence to suggest that the type of external facilitation provided to support implementation in this project is both beneficial and cost effective.22 For example, a recent systematic review by Baskerville and colleagues,23 which reviewed 23 studies of practice facilitation in primary care settings, concludes that practices are 2.76 times more likely to adopt evidence-based guidelines if they have the support of outreach facilitators.
From our experience to date, it appears that combining the structured approach of the collaborative with tailored implementation strategies is one that has merit, although more detailed evaluation is needed to systematically track the processes at work over time and assess impact and outcomes. This includes a more detailed assessment of the extent to which the improvement collaborative approach to implementing evidence into practice offers a reasonable return on investment. This is something that we aim to report more fully once the second phase of the implementation study is complete.
Acknowledgments
We are grateful to the participants in the CKD collaborative for their involvement, commitment and feedback on the experience of the collaborative. The views and opinions in the paper do not necessarily reflect those of the NIHR.
References
Footnotes
Funding The project reported in the paper was undertaken within the NIHR CLAHRC for Greater Manchester, which is funded by the NIHR and the 10 primary care trusts in Greater Manchester.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data available on request from the corresponding author.