Article Text

Abstract
Background Bloodstream infections from central venous catheters (CVC-BSIs) increase morbidity and costs in intensive care units (ICUs). Substantial reductions in CVC-BSI rates have been reported using a combination of technical and non-technical interventions.
Methods We conducted a 2-year, four-cluster, stepped non-randomised study of technical and non-technical (behavioural) interventions to prevent CVC-BSIs in adult and paediatric ICUs in England. Random-effects Poisson regression modelling was used to compare infection rates. A sample of ICUs participated in data verification.
Results Of 223 ICUs in England, 215 (196 adult, 19 paediatric) submitted data on 2479 of 2787 possible months and 147 (66%) provided complete data. The exposure rate was 438 887 (404 252 adult and 34 635 paediatric) CVC-patient days. Over 20 months, 1092 CVC-BSIs were reported. Of these, 884 (81%) were ICU acquired. For adult ICUs, the mean CVC-BSI rate decreased over 20 months from 3.7 in the first cluster to 1.48 CVC-BSIs/1000 CVC-patient days (p<0.0001) for all clusters combined, and for paediatric ICUs from 5.65 to 2.89 (p=0.625). The trend for infection rate reduction did not accelerate following interventions training. CVC utilisation rates remained stable. Pre-ICU infections declined in parallel with ICU-acquired infections. Criterion-referenced case note review showed high agreement between adjudicators (κ 0.706) but wide variation in blood culture sampling rates and CVC utilisation. Generic infection control practices varied widely.
Conclusions The marked reduction in CVC-BSI rates in English ICUs found in this study is likely part of a wider secular trend for a system-wide improvement in healthcare-associated infections. Opportunities exist for greater harmonisation of infection control practices. Future studies should investigate causal mechanisms and contextual factors influencing the impact of interventions directed at improving patient care.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Introduction
Blood stream infections (BSIs) from central venous catheters (CVCs) increase morbidity and are estimated to increase mortality risk by 25% and costs of care in the USA by US$16 550 on average per patient1 ,2 (box 1). A substantial body of evidence suggests that rates of CVC-BSIs are modifiable.3–13 The Michigan-Keystone project13 in 103 intensive care units (ICUs) in the USA reported a major reduction in CVC-BSIs from 7.7 to 1.4 CVC-BSIs per 1000 CVC-patient days using a complex intervention targeting specific technical practices (box 2), combined with support for cultural, behavioural and systemic change.14 A 3-year follow-up study reported sustained improvement15 and accelerated the trend for a reduction in case mix-adjusted mortality rates.16
Background
-
Central venous catheters (CVCs) are widely used in patients in intensive care units (ICUs) and other hospital locations for monitoring, drug delivery, and dialysis
-
CVCs increase the risk of blood stream infections (BSIs) which increase mortality and costs of care
-
CVC-BSIs can substantially be prevented when clinicians use best practice guidance during catheter insertion and subsequent maintenance
-
CVC-BSI rates in the NHS in England are unknown
-
This study examined the impact of benchmarking and best practice guidance on minimising CVC-BSIs in English ICUs
Technical interventions to reduce central venous catheters (CVC)-blood stream infections
-
Hand hygiene, gown, gloves, hat, mask. Eye protection when indicated
-
Skin antisepsis: 2% chlorhexidine gluconate in 70% isopropyl alcohol
-
Maximal sterile precautions including full barrier drapes
-
Site of insertion: avoid the femoral route
-
CVC maintenance: aseptic access technique, daily site review, and remove CVCs at earliest opportunity
The NHS Next Stage Review in 200817 announced that the National Patient Safety Agency (NPSA) would run a ‘national patient safety initiative to tackle central line catheter-related blood stream infections, drawing lessons from a remarkably successful Michigan initiative’. This 2-year programme, known as Matching Michigan, ran in England from April 2009 to the end of March 2011. It aimed to minimise CVC-BSI rates in adult and paediatric ICUs in England to at least the mean level (1.4 per 1000 CVC-patient days) seen in the Michigan-Keystone project. It involved three components: technical interventions, which sought to ensure consistent use of evidence-based measures for reducing risks of CVC-BSIs; non-technical interventions, which sought to intervene in culture and systems; and establishment of a standardised national reporting system for CVC-BSIs. All participating sites were invited to take part in two training sessions, the first focused on data collection and the second focused on the technical and non-technical interventions.
Matching Michigan followed, and took place during, heightened media interest and policy initiatives focused on healthcare-associated infections and BSIs (table 1) including the introduction by the Department of Health (DoH) in 2007 of best practice guidance on CVC insertion and management18 through its multicomponent ‘Saving Lives’ programme.19 Other improvement activities relevant to CVC-BSIs included the Health Foundation's Safer Patients Initiative, which ran in two phases from 2004 to 2008,20 and the Patient Safety First campaign, which began in 2008.21 However, in the absence of a national reporting system, it was not possible to assess the impact of any of these or any other efforts on CVC-BSI rates.
The context: national infection control initiatives in England before and during Matching Michigan
In this article, we report an analysis of the impact of Matching Michigan on rates of reported CVC-BSIs in adult and paediatric ICUs in England.
Methods
Design
This was a prospective, interventional, non-randomised, stepped, four-cluster, 2-year quality improvement project with continuous feedback of results to participating ICUs. The National Research Ethics Committee waived the requirement for informed patient consent on the basis that the intent was to improve uptake of established best practice care, and no patient-identifiable information would be collected centrally.
Delivery and recruitment
The NPSA established a national project team and an External Reference Group representing professional and governmental organisations. The scientific leads from the original Michigan-Keystone project acted as advisors and provided their improvement tools. Chief executive officers (CEOs) of all acute hospitals in England with ICUs were invited to participate in the programme. Participating hospitals agreed to appoint a local project team comprising an ICU physician, an ICU nurse, a microbiologist or infection control specialist and an executive or non-executive director.
Clusters
ICUs were grouped into four clusters with stepped implementation (table 2). Cluster 1 (North-Eastern Strategic Health Authority) allowed piloting of data collection, training and interventions. Clusters 2 and 3 comprised ICUs in southern and northern England respectively. Cluster 4 consisted of ICUs unable to join the project in the earlier phases.
ICU clusters, duration in project, training day attendance and reliability of submission of infection data
Definitions
Definitions of CVC, BSI, catheter-related (CRBSI) and catheter-associated BSI (CABSI) and measures of exposure are not straightforward. There is considerable evidence of variability in these definitions or a lack of clarity in their application in prior publications.22–25 The definitions we used, which were current in 2009, were from the Hospital In Europe Link for Infection Control through Surveillance programme,26 and the US National Nosocomial Infection Surveillance System from the Centre for Disease Control & Prevention,27 ,28 and were piloted and refined to ensure applicability and ease of understanding for an English context (see electronic supplementary material 1 (ESM 1)). The definitions distinguish between the surveillance definition of CRBSI and the clinical definition of CABSI. The key distinction between these definitions lies in the type of microbiological analysis undertaken to determine whether the source of any individual BSI can be attributed to a CVC.
ICUs were asked to submit data monthly to a specially created web-based system and to identify which definition they used for each infection at the time of reporting. Infections reported as either CRBSI or CABSI were summed to calculate infection rates. Measures of exposure were recorded through a daily census in each ICU involving a count of the number of CVCs in situ at a set time each day. ICUs were asked to complete a survey on generic infection control practices (table 3). Infection data could be submitted until 31 March 2011. However, to permit data cleaning before project closure, analysis was limited to the 20-month period from May 2009 to December 2010.
ICU infection control practices (127 respondents of 223 ICUs, response rate 57%)
Training and support
Each cluster was invited to attend two training days, the first on the data definitions developed for the programme (ESM 1) and the second some months later on the technical and non-technical interventions (table 4) adapted from the Michigan-Keystone project.14 Training was held in a centralised location and involved plenary and small group interactive sessions. ICUs started baseline data collection as soon as possible after the first training day.
Technical and non-technical interventions
Teleconference calls and internet-based teaching sessions were offered over the course of the programme. Guidance was provided by telephone and email and, if appropriate, on-site visits by two quality improvement facilitators (ICU nurses). The Patient Safety First website was used to host information on the interventions and on the programme more generally.21 The project clinical leads provided additional ad hoc support and guidance when required.
Data verification
Data limits and rules programmed into the software allowed erroneously entered data to be detected and corrected through the web-based tool. Extreme values were examined by clinical members of the project team, and discussed with local project leads. We also undertook verification of consistency between ICUs in identifying and reporting CVC-BSIs in a purposive sample of ICUs. To conduct the verification, we used on-site criterion-referenced case note review and contemporaneous telephone discussion with a second remote and blinded reviewer. Following institutional approval, each ICU in the verification sample provided a list of all blood cultures (BCs) performed over 3 months, and the case records of 5–20 patients with positive BCs. The number of BCs performed and the number of CVC-patient days were compared with the number of patient days to determine the frequency of sampling for BCs, and the CVC-utilisation ratio. Local adjudication and reporting of each CVC-BSI was compared with external review. Inter-observer agreement was determined using the κ statistic. ICUs were not asked to provide self-reported data on compliance or implementation of the technical and non-technical interventions because there was no method of assuring data reliability or completeness.
Statistical analysis
Random-effects Poisson regression modelling was used for the primary outcome, based on mean monthly CVC-BSIs related to CVC-patient days, anchored by time since the second training day for each cluster (zero pre-intervention, number of months from month of intervention onwards), and using as covariates the time trend (months from May 2009), teaching status, size of unit, random effect of unit, and cluster. This tests the hypothesis that the intervention (the second training day) will change the slope of an underlying secular trend. To explore whether changes in ICU infection rates were independent of, or potentially part of, a whole-hospital trend, and in the absence of a measure of pre-ICU exposure rates, we compared quarterly pre-ICU with ICU-acquired infection rates expressed as the proportion of all CVC-BSIs which were ICU acquired (ICU-acquired CVC-BSIs divided by the sum of ICU-acquired and pre-ICU CVC-BSIs). A stable ratio over time would suggest ICU trends were part of a wider whole-hospital effect. A χ2 test for trend was performed to evaluate changes in this ratio. All p values are two sided, with p≤0.05 considered statistically significant. Stata (V.9) was used for all analyses.
Results
Participant characteristics
Chief executives of all (139) acute hospitals in England with ICUs agreed that their organisations would participate. Of these, 32 (23%) were university hospitals. The study sample represented 223 ICUs, of which 176 (79%) were general adult ICUs, 21 (9%) paediatric, and 26 (11.6%) subspeciality. The mean (range) number of ICU beds per unit was 12 (3–43); the mean (range) annual admissions was 685 (166–2423). More than 80% of ICUs attended both training days (table 2), though the size of the team attending training ranged from single individuals (doctor or nurse) to large groups including executive leads.
Most (96.4%, 215) ICUs submitted at least some infection data to Matching Michigan. Responses (57%) to the survey of generic infection control practices demonstrated wide variation between ICUs (table 3).
Infection rates
Infection data were submitted on 2479 ICU-months of a maximum 2787, giving a reliability rate of 0.89. Complete data were submitted for every possible month by 147 (66%) ICUs (range between clusters 63–68%) (table 2). The first cluster of 19 ICUs (15 adult, 4 paediatric) provided baseline comparator infection data for subsequent clusters. Clusters 2 and 3 received their training a few weeks apart and their infection data were merged into a single cluster for analysis.
Of 1092 CVC-BSIs reported over 20 months, 884 (81%) were ICU acquired. A majority (66.7%) were diagnosed using the catheter-associated definition (table 5). Paediatric CVC-BSIs accounted for 14.6% of total declared infections, but only 7.89% of CVC-patient days. A total of 438 887 (404 252 adult and 34 635 paediatric) CVC-patient days were reported, giving a mean ICU-acquired infection rate for the entire project of 2.01 CVC-BSIs per 1000 CVC-patient days (adult ICUs 1.88, paediatric ICUs 3.58). Detailed monthly infection and CVC utilisation rates are given in ESM 2.
1092 CVC-BSIs by infection classification and location
Changes in infection rates
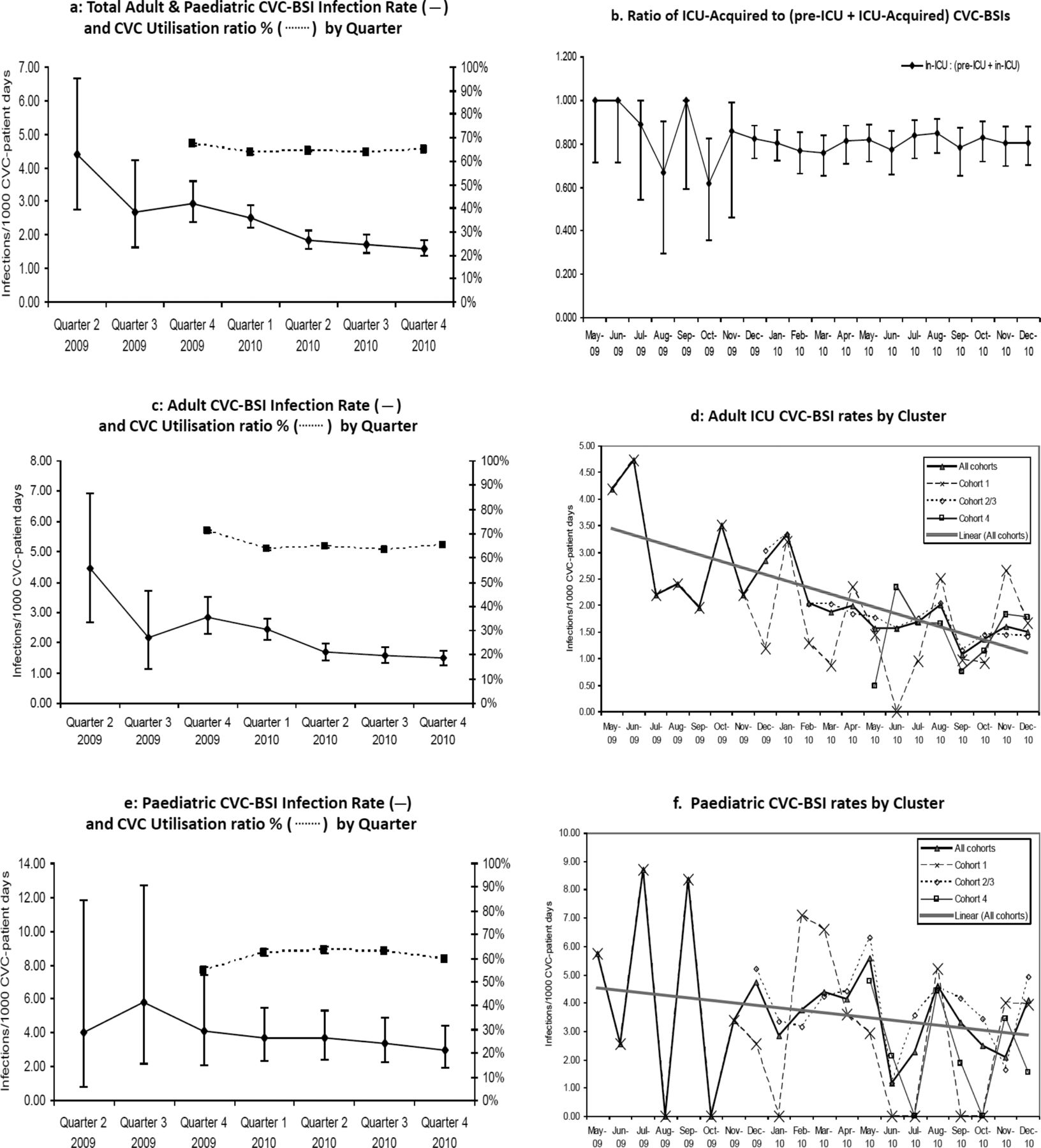
Aggregated adult and paediatric ICU infection rates diminished with time from a first month rate of 4.4 CVC-BSIs/1000 CVC-patient days for cluster 1, to 1.7 CVC-BSIs in December 2010 (all clusters) (ESM 2 monthly, figure 1A quarterly). The ratio between ICU-acquired CVC-BSIs and all CVC-BSIs remained stable during the project (test of homogeneity χ2=16.11, p=0.6497; test for trend of odds χ2=0.12, p=0.7237), suggesting a possible common cause for the reduction in infection rates in ICU and non-ICU locations (figure 1B).
{kind=link}
Central venous catheter (CVC)-blood stream infection (BSI) rates. (A) Total adult and paediatric CVC-BSI infection rate (——) and CVC utilisation ratio % (……) by quarter. (B) Ratio of intensive care unit (ICU)-acquired to (pre-ICU+ICU-acquired) CVC-BSIs. (C) Adult CVC-BSI infection rate (——) and CVC utilisation ratio % (……) by quarter. (D) Adult ICU CVC-BSI rates by cluster. (E) Paediatric CVC-BSI infection rate (——) and CVC utilisation ratio % (……) by quarter. (F) Paediatric CVC-BSI rates by cluster.
Mean adult ICU CVC-BSIs diminished from 3.7 CVC-BSIs/1000 CVC-patient days in the first quarter (inception of cluster 1), to 1.48 in the last quarter (figure 1C), and for paediatric ICUs from 5.65 (four paediatric ICUs) to 2.89 (18 paediatric ICUs) (figure 1E). The progressive reduction in infection rates was statistically highly significant for adult ICUs (Z statistic −4.45, χ2 p<0.0001), but not paediatric ICUs (Z statistic −0.79, χ2 p=0.625).
The rate of change in reduction in infection rates did not accelerate following the second training day. For adult ICUs, each successive cluster to join the project had an entry-level infection rate close to the post-intervention level of the preceding cluster (figure 1D) (Z statistic 1.29 and 0.87, χ2 probability 0.19 and 0.38 for clusters 2 and 3 and cluster 4 respectively). Late engagement (cluster 4) was not associated with poorer performance in any metric. Numbers were too small, and the variation in infection rates too great, to draw secure conclusions from the paediatric data (figure 1F).
Associations
The trend for reduction in infection rates was not associated with hospital type or the number of CVC-patient days for either adult or paediatric ICUs. CVC utilisation ratios could only be determined from December 2009; utilisation rates remained stable (66.3/100 patient days for December 2009–February 2010, 64.6/100 for October–December 2010) (ESM 2 and figure 1A,C,E), despite the continuing fall in pre-ICU and ICU-acquired CVC-BSI rates for this period.
Attendance at both training days was achieved by 179 ICUs (80.3%), 127 of which also provided 100% complete infection data (of 147 ICUs achieving this). Training day attendance was strongly associated with more reliable data submission (χ2 10.2187, p<0.005), but not with infection rates (Z statistic −0.29, p=0.773).
Data verification
Twenty-eight of 45 ICUs responded to an invitation to participate in data verification and 17 actually participated (one paediatric ICU, two university, 14 adult general). Reasons for non-participation included no response to further contacts (10), clinical workload (3), inadequate administrative support (4), absence of timely authority to access medical records (7), and inadequate project team resources (4).
The 17 ICUs participating in the verification sub-study performed 2357 BCs during 17 020 patient-days and 10 601 CVC-patient days, of which 328 (13.9%) BCs were positive (ICU range 5.7–23%). Frequency of sampling and CVC use varied widely: the BC:patient-days ratio was 2357/17 020=13.8 BCs/100 patient-days (range 4.8–39.6) and the CVC utilisation ratio was 0.62 (range 0.42–0.78).
Criterion-referenced case note review was conducted in 177 patients with 187 positive BCs; in 54 patients (30.5%) no CVC was in situ within 48 hours of the positive BC, which excluded potential CVC-BSIs. Of the 177 patients with positive BCs, 17 had been declared as CVC-BSIs and 160 as non-attributable. External adjudication agreed with local adjudication in 167 instances (seven reclassified as attributable, three as non-attributable, overall correct classification 94.3%). The kappa for agreement between local and external adjudicators was 0.706 (SE of kappa=0.088; 95% CI 0.534 to 0.877). The method did not permit determination of CVC infection in the absence of a blood culture.
Discussion
On initial examination, and using the metrics employed by the majority of studies in this area, Matching Michigan was a success. The programme demonstrated a 60% reduction in reported CVC-BSIs in adult ICUs in England, despite starting with less headroom for improvement than the original Keystone-Michigan project13 (baseline 4.4 CVC-BSIs per 1000 patient catheter days in the first Matching Michigan cluster compared with 7.7 at baseline in Michigan). For paediatric ICUs the 48% reduction did not achieve statistical significance; the difficulty of reducing CVC-BSIs in paediatric intensive care is well recognised.29–32 A conventional narrative might run thus: training in technical and non-technical interventions to improve patient safety combined with measurement and performance feedback stimulated a change in behaviour which resulted in a reduction in BSIs from CVCs.
Closer examination of the data reveals a more complex picture requiring a nuanced interpretation. Attributing the impressive reduction in adult ICU CVC-BSIs rates solely to programme participation is complicated by two novel insights. First, each successive cluster joined the project on the trend line for the post-intervention level of the preceding cluster, thus indicating a strong secular trend. Second, pre-ICU infections (which were not targeted by Matching Michigan) diminished in line with ICU-acquired infections, indicating that the secular trend was not limited to the ICU. These findings suggest the possibility that the reduction in infection rates could be attributable as much to concurrent and preceding improvement efforts and to the consciousness-raising effect of a nationwide programme as to any specific component of the Matching Michigan programme itself.
This study is an example of the challenges of conducting field evaluations of complex interventions to improve care in real time in rapidly moving fields. It illustrates in particular the challenges of identifying causal mechanisms during ‘rising tides’ when multiple policy pressures and the emergence of professional and scientific consensus combine to produce improvements across the board.33–35 Falling rates of CVC-BSIs have been reported in a number of studies worldwide36 ,37 and our study was undertaken during a period of intense national activity in England directed towards reducing hospital-acquired infections, including methicillin-resistant Staphylococcus aureus BSI rates (which fell by 22% between April 2009 and March 2011, and by 50% since 2008).38 For example, many hospitals had already introduced 2% alcoholic chlorhexidine skin disinfectant, full-barrier drapes were becoming more widely available, and alcohol hand rub had become universally available.
Our stepped before and after design reduces the risk of bias,39 and the analysis therefore emphasises the need for caution in attributing the reduction in infection rates to specific elements in the programme. Lack of a specific causative link between complex behavioural interventions and improved outcomes has been reported for end-of-life care,40 stroke care,33 coronary balloon angioplasty34 and multifaceted safety programmes,35 while others have reported strong secular trends for improvement in CVC-BSI rates in conjunction with national reporting but in the absence of specific targeted interventions.36 Financial penalties as a further stimulus for improvement do not appear to have had an additional impact on the adoption of self-reported CVC-BSI prevention measures in the USA.41
Study designs involving randomisation, which could help to determine quality improvement programme effects more precisely, are challenged by ethical considerations when best practice is already well established, and practical considerations of isolating intervention from controls. Cluster-randomised designs are particularly important for interventions involving behavioural change,40 ,42 since the component elements may be rooted in specific cultures, locations and periods, and require testing in the same way as a pharmaceutical intervention in a new population.43 ,44
A design such as that used in our study—involving clusters joining in a pre-determined sequence, with each successive cluster acting as a de facto control for the preceding cluster—although not formally randomised is one of the more robust approaches that can feasibly be deployed. However, it is subject to a number of threats to internal validity. The ‘waiting’ clusters were exposed to diffusion of treatment effects, as the interventions were widely publicised on the Patient Safety First website from the beginning of the study, and the original Michigan-Keystone project had received widespread attention. ICUs in ‘waiting’ clusters may also have engaged in ‘compensatory rivalry’,45 and increased their efforts to reduce CVC-BSIs while waiting to join the programme. It is also possible that the reduction in reported rates of infections may to some extent have been an artefact of reporting behaviours, since data were collected and reported by ICUs themselves and may have been influenced by perceptions of external scrutiny and performance management.46 How far any trend in reported infection rates may reflect changes in reporting behaviour over time is not easy to establish. A further limitation of our study was the absence of measures of adoption of the interventions and compliance with best practice. Several studies have reported an association between higher compliance and lower infection rates,47–49 but data completeness and the methods chosen for compliance monitoring are rarely described in detail, and the literature on hand hygiene demonstrates poor correlation between self-reported and observed compliance.50–52
The data verification sub-study provides some reassurance of validity in relation to reporting behaviours, but also demonstrates considerable variability in local practices in relation to CVC use and intensity of sampling blood for culture. Variability in surveillance techniques is well recognised and substantially alters reported infection rates.25 The survey of generic infection control practices (not compliance with the technical interventions) demonstrates wide variation, including the level of interaction between intensive care physicians and microbiologists. These factors make direct comparison between ICUs challenging. Harmonisation of practice would reduce the risk of confounding, and could bring additional benefits in reducing nosocomial infection rates.
Despite the difficulties of identifying specific programme effects, it is unlikely that the contribution of large-scale programmes such as Matching Michigan to the ‘rising tide’ is trivial. Such programmes may have a particular role in raising awareness, increasing the intensity of focus and stimulating managerial support for professional activities. Feedback of infection rates may have promoted more reliable provision of and adherence to the well known technical aspects of infection prevention for CVCs. Understanding more precisely how such programmes work remains an important task, since such understanding is likely to avoid inappropriate and ineffective interventions, optimise delivery and improve effectiveness.53 This is especially important when elements of programme design vary from the original: Matching Michigan was not exactly the same as the original Michigan-Keystone project. Differences included amendments to some of the programme materials to ensure contextual relevance; definitions of CVC-BSIs were specified more precisely; and the programme was directed by a government agency with advisory clinician input, not as a clinician-led collaborative. Contextual variability was also evident: Matching Michigan was, unlike Michigan-Keystone, implemented following extensive prior national efforts to improve practice, in a national health system in which intensive care specialists direct infection management with input from microbiology, as opposed to this being the domain of independent infection control practitioners.
It is encouraging that reported rates of pre-ICU and ICU-acquired CVC-BSIs showed reductions over the course of Matching Michigan. Reduced rates of infection will deliver health gains for patients and benefits for health systems. The apparent trend for a reduction in CVC-BSIs acquired before ICU admission should not encourage complacency, however,54 since in the absence of a denominator, conclusions cannot be drawn about rates of infection and quality of care. CVC use in non-ICU locations requires the same intensity of focus as it has received in the ICU.55–60 A national clinician-directed system for sustained continuous CVC-BSI benchmarking, such as those in Scotland61 and Wales,62 would ensure continued attention to CVC-BSIs, and could provide a platform for monitoring other healthcare-associated infections with linkage to patient outcomes.
This study adds to the science of improvement by using a quasi-experimental design that reveals the significance of underlying secular trends but does not rule out the possibility that the programme itself was implicated in that trend. Future studies should use robust mixed-methods research methodologies to clarify causal mechanisms underpinning quality improvement interventions, and to identify those most likely to promote more reliable delivery of best practice throughout the healthcare system, as well as promoting clinician ownership.63 To this end, a separate, independent ethnographic study of culture and behaviour in relation to CVC-BSIs in England was conducted at the same time as Matching Michigan and may provide insights that will promote such understanding.
Appendix
Core group: Peter Hibbert, Annette Richardson, Jeanette Beer, Sharon Jefferson, Sarah Goode, Catherine Ede, Tracy Abrusci, Gowri Sivakumaran, Bruce Warner, Julian Bion, Kevin Gunning, Geoff Bellingan, Mark Patten, Jane Cassidy, Ginny Edwards, Jane Eddleston, Adam Fraise, Keith Young.
Analytical, statistical and methodological support: Jill Altman, Martin McCutcheon, Sarah Leong, David Harrison, Peter Pronovost, Christine Goeschel.
External reference group: Helen Stirton (British Association of Critical Care Nurses), Brian Duerden (Department of Health), Andrew Pearson and Jennie Wilson (Health Protection Agency), Kathy Rowan (Intensive Care National Audit and Research Centre), Carl Waldmann (Intensive Care Society), Adam Fraise (Hospital Infection Society), Martin Kiernan (Infection Prevention Society), Steve Page and Emma Nunez (Strategic Health Authorities), Roddy O'Donnell (Paediatric Intensive Care Society), Barry Williams (Patient/User Representative), Stuart Stevenson (Patient Safety Champion), Sue Goulding (Patient Safety Action Team representative), Rachel Binks (Royal College of Nursing Critical Care Forum), Ravi Mahajan (Royal College of Anaesthetists), Simon Mackenzie (Scottish Intensive Care Society), Edward Kelley and Iciar Larizgoitia (World Health Organisation), Louise Teare (Director of Infection Prevention & Control, Bromfield Hospital), Chris Hancock (National Leadership and Innovation Agency for Healthcare).
Local project leads in each collaborating ICU: Addenbrooke's Hospital: Andrew Johnston, Rowan Burnstein, Samir Latifi, Ingrid Jackson, Pamela Bushen, Deborah White, Jumoke Sule, Nicholas Brown, Basil Matta. Airedale General Hospital: Alwyn Kotze, Karen Price, Alison Charlesworth, Bridget Fletcher. Alder Hey Children's Hospital: Steve Kerr, Andy Darbyshire, Pauline Bradshaw, Sian Snelling. Arrowe Park Hospital: Conor McGrath, Graham Ledgerton, Debbie Kretzer, Lesley Metcalfe. Ashford & St Peters Hospital: Melinda Brazier, Denise Hallett, Ingrid Johnson, Ian White, Valerie Howell, Tina Thomas. Barnet Hospital: Andy Cohen, Tony Wolff, Richard Harrison, Liz Stewart, Terina Riches. Barnsley Hospital: Jyothi Rao, Ken Inweregbu, Ye Myint, Tracey Smith. Basildon University Hospital: David Lowe, Yasser Shouman, Claire Winterflodd, Sian Morgan, Gayle Matthews, Maggie Rogers. Basingstoke & North Hampshire Hospital: David Niblett, Sandy Kirk, Fran Bertasius, Nicki Hutchinson. Birmingham Children's Hospital: Jeff Martin, Helen Winmill, Ursula Nusgen, Michelle McLoughlin. Blackpool Victoria Hospital: Nigel Randall, Palanikumar Saravanan, Lise Cross, Sue Howart, Liane Moorhouse, Paul Kelsey. Bristol Royal Hospital for Children: Peter Murphy, Tim Gould, Kathryn Hole, Katie Sweet, Louise Jenkins, Martin Williams, Jonathan Sheffield. Broomfield Hospital: Dilshan Arawwawala, Christine Mitchell-Inwang, Louise Teare, David Blainey. Calderdale Royal Hospital: Michael Howard, Johanna Turner, Helen Thomson. Castle Hill Hospital: J Elton, K Jessop, R Owen-Smith, L Hartley, E Henderson, C Hibbert. Central Middlesex Hospital: Jacek Borkowski, Nasia Ghani, Fiona Coogan, Elizabeth Robb. Charing Cross Hospital: Adrian Steele, Gary Mendoza, Clare Johnston, Alison Holmes. Chase Farm Hospital: Nicholas MaCartney. Chelsea & Westminster Hospital: Jason Tatlock, Jane Marie Hamil, Berge Azadian. Cheltenham General Hospital: Mark Haslam, Liz Bruce, Robert Jackson, Andrew Seaton. Chesterfield Royal Hospital: Charlie Cooper, Jayne Tague, Diane Simpson, Alfonzo Tramontano. City Hospital: Jonathan Hulme, Janka Webb, Beryl Oppenheim, Donal O'Donoghue. Colchester General Hospital: Mohamed Ramali Conquest District General Hospital: Kate Murray, Christa Wood, Barry Phillips, Harry Walmsley. Cumberland Infirmary: Simon Jones,Susan Brown, Manjula Meda, Sandy Brown. Darent Valley Hospital: Mike Protopapas, Tara Laybourne, Peter Orsman, Jenny Kay, Phillipa Wakefield, Helen Bradshaw. Darlington Memorial Hospital: Dominic Errington, Iain Veitch, Joanne Todd, Robert Aitken. Derriford Hospital: Andrew Tillyard, Peter Robbins, Carol Pollard, Judith Frame, Charlotte Kendall, Claire Haill, Alex Mayor. Dewsbury & District Hospital: Hugh Obeirne, Carol Wood, Wendy Smith, Tracey McErlain. Diana Princess of Wales Hospital: Annang Asumang, Mrs Amanda Holmes, Vivien Duncanson, Jane Partridge. Doncaster Royal Infirmary: David Wood, Louise Lowry, Christine Hoy, Lee Cutler. East Surrey Hospital: Mary Sexton. Eastbourne District General Hospital: Rhiana Edwards, Mandy Chequers, Barry Phillips, Harry Walmsley. Epsom Hospital: Stanislaw Jankowski, Sheila Obee, Amita Sharma. Evelina Children's Hospital: Ian Murdoch, Louise Dewsbury. Fairfield General Hospital: Ravi Marthi, Vivk Yadav, Linda Reynolds, Reeta Burman. Freeman Hospital: Jane Cassidy, Jon Walton, Kevin Brenan, Angela Johnson, Debbie Lawson, Lorna Charlton, Alistair Gascoigne, Kate Gould, Timothy Walls. Frenchay Hospital: Ian Thomas, Rachael Smith, Kim Jacobson, Christopher Burton. Friarage Hospital: Andrew Barrington, Krish Srikanth, Paul Buckley, Caroline Morley, Julie Barlow, Kolanu Prasad. Frimley Park Hospital: William Jewsbury, Justin Woods, Nupur Goel, Edward Palfrey. Furness General Hospital: David Highley, Lynne Wyre, Kim Wilson, Jackie Holt. George Eliot Hospital: Vivek Poongavanam, Marian Foster, James Clayton, Nigel Kee. Gloucestershire Royal Hospital: Chris Roberts, Jim Stone, Liz Bruce, Nicky Giles. Good Hope Hospital: Maung Kyi. Great Ormond Street Hospital, Central London: Ann Karimova, Christine Pierce, Annabel Linger, Clare Paley, Yvette Harding, James Soothill, Robert Evans. Guy's & St Thomas’ Hospitals: Duncan Wyncoll, Kath Daly, David Tucker, Eileen Sills. Hammersmith Hospital: Stephen Brett, Steve Thoresen. Harefield Hospital: Chris Meadows, Sunny Kaul, Peter Doyle, Pat Cattini, Robert Craig. Harrogate District Hospital: David Earl, Chris Gill, Kevin Kerr, Anne Lawson. Heartlands Hospital: Jock Melbeck, Sarah Quinton, Itisha Gupta, Roger Stedman. Hereford County Hospital: Anne Miles, Gillian Hill, Alison Budd. Hillingdon Hospital: Andrew Thorniley, Sohan Bissoonauth, Pippa Dorney-Kingdom, Arup Ghose, Marie Batey. Hinchingbrooke Hospital: Rizwan Hasan, Corin Prunty, Andreas Karas, Richard Dickenson. Homerton University Hospital: Robert Ghosh, Tina Stubbs, Alleyna Claxton, Pauline Brown. Horton General Hospital: Jillian Hewitt-Gray, Sharon Buchanan, Dayle Kinch. Huddersfield Royal Infirmary: Julie O'Riordan, Janice Carter. Hull Royal Infirmary: J Elton, I Smith, P Cole, C Turner, E Henderson, C Hibbert. James Paget Hospital: Katherine Kite, Lynn Everett, Linda Hawtin, Nick Coveney. John Radcliffe Hospital: Stuart McKechnie, Alison Shefler, Derrick Crook, Quentin Ainsworth, Shane George, Mhairi Speirs, Lorna Gale, Matthew Gasson, Jane Woollard, Jill Titchell, Sarah Malone, Rochelle Lay, Simon Wells, Lisa Butcher, Lily O'Connor. Kent & Sussex Hospitals: Lee Baldwin, Debbie Spinner. Kettering General Hospital: Phil Watt, June Thomas, Pam Howe, Liz Libiszewski. King's College Hospital, Denmark Hill: Stephanie Strachan, Jennifer Caguioa, Amanda Fife, Erika Grobler. King's Mill Hospital: Lisa Milligan, Valerie Whitaker, Win Maung, Andy Taylor. Leeds General Infirmary: Phil Jackson, Simon Whitely, Tim Palfreman, Sanjay Agrawal, Dorothy Kitching, Jennifer Asker, Juliette Cosgrove, Innes Reid, John Roche. Leicester Royal Infirmary and Leicester General: Kate Wilkins, Sue Davey, Moira Durbridge. Leighton Hospital: Susan Gilby, Sian Axon, Tracy Schiavone, Tracy Bullock. Lincoln County Hospital: Alan Liddle, Matthew Dolling, Sarah Southall, Charmian Hutson, Adam Wolverson. Queen Elizabeth II and Lister Hospitals: Pin Patel, Wendy Collier, Helen O'Connor, Sue Greenslade, Amanda Radford. Liverpool Heart & Chest Hospital: Nigel Scawn, Sandra Roberts, Nicola Best, Glenn Russell. Luton & Dunstable Hospital: Mark Patten, Karen Cairnduff, Rohinton Mulla, Elaine Hide. Macclesfield District General Hospital: John Hunter, Heather Cooper, Simon Cartiledge, John Wilbraham. Maidstone District General Hospital: Angus Turner, Wendy Lepke-Brown, Flo Panel-Coates. Manchester Royal Infirmary: Jane Eddleston, Niall O'Keeffe, Anne Tighe, John Logan, John Moore, Andrew Dodgson, Gill Heaton. Manor Hospital: Chris Newson, Katrina Hajdu, David Jones, Mike Browne. Medway Maritime Hospital: David Simpson, Ravi Singh, Kate Gray, Linda Dempster, Gulzar Mufti. Milton Keynes Hospital: Hamid Manji, Mali Bharamgoudar, Jane Adderley, Angela Legate, Robert Heavisides. Musgrove Park Hospital: Richard Innes, Carolyn Panton, Maggie Bradfield, Cecil Blumgart. New Cross Hospital: Simon Hester, Susan Rowlands, Joanne Ellison, David Loughton. Newcastle General Hospital: Barbara Fulton, Huw McConnell, Iain Johnstone, Catherine Coulter, Claire Riddell, Lesley Scott, Muhammad Raza. Norfolk & Norwich University Hospital: Tim Leary, Jill Roberts, Ngozi Elumogo, Judith Richards, Krishna Sethia. North Devon District Hospital: Andrew Walder, Lynsey Phillips, David Richards, Carolyn Mills. North Manchester General Hospital: Andrew MacKillop, Sally Murphy. North Middlesex Hospital: Mohan Sivarajaratnam, Vikki Howarth, Ian Hossain, Narayan Rao. North Tyneside General Hospital: Andrew McHutchon, Sue Ewart, Cathi Lang. Northampton General Hospital: Richard Marsh, Mary Burt, Anthony Bentley, William Duguid. Northern General Hospital: Steve Webber, Claire McEwan, Mike Heap, Des Breen. Northwick Park Hospital: Gary Wares, Irene Porter. Nottingham University Hospital: Julian Skoyles, Adam March, Asrar Rashid, Mallory Mercer, Helen Lushpenko-Brown, Sue Mager, Tim Boswell, Jill Wilson, Stephen Fowlie, Peter Homa, Dave Sperry, Anne Illsley. Papworth Hospital: Stephen Webb, Maura Screaton, Mari Ylivinkka, Josie Rudman. Peterborough District Hospital: Balraj Appadu, Lorna Clinton, David Enoch, Chris Wilkinson. Pilgrim Hospital: Andrew Norton, Karen Latham, Wendy Creasey, Paul Dunning. Poole General Hospital: Henrik Reschreiter, Kenneth Power, Amanda Saltmarsh, Susan Sutherland. Princess Alexandra Hospital: Rajnish Saha. Princess Royal Hospital: Ian Littlejohn, Russell Hedley, Owen Boyd, Angela Jenkinson, Clare Hebditch. Queen Alexandra Hospital: John Knighton, Matthew Richardson, Caroline Mitchell, Ursula Ward. Queen Elizabeth Hospital: Lyn Swanson, Martin Wood, Janet Thompson, Shirley Richardson. Queen Elizabeth Hospital, Birmingham: Brian Pouchet, Kaye England, Sandeep Walia, Tessa Oelofse, Tomasz Torlinski, Naomi Cole, John Fletcher, Nicki Dickson, Sam Wise, Adam Fraise, Pauline Jumaa, David Burbridge, Kevin Bolger, Kay Fawcett, Morag Jackson. Queen Elizabeth Hospital Woolwich: Peter Roberts, Sam Platt, Susan Bragman. Queen Mary's Hospital, Sidcup: Chris Palin, Sharon Paminter, Tracey Cooper. Queen Victoria Hospital, East Grinstead: Ken Sim, Nicola Heneghan, Amanda Parker, Alison Munday Queen's Hospital: Rajesh Jain, Jitendra Garg, Nicola Dearson, Corrine Cameron-Watson, Stephen Peter Burgess. Queen's Hospital Burton Upon Trent: Paul Stewart, Jackie Jones, Steve Harding, Jonathan Sheldon. Rochdale Infirmary: Anil Gupta, Helen Barrow, Claire Chadwick, Marian Carroll. Rotherham District General Hospital: Gerry Lynch, Derek Bainbridge, Sarah Cooper, Andrew Jackson, Chris Hughes. Royal Albert Edward Infirmary: Rafat Saad, Julie Barrett, Rob Nelson, Gill Harris. Royal Berkshire Hospital: Chris Danbury, Anne Savage, Linda Hosie, Nilangi Virgincar, Nigel Davies. Royal Blackburn Hospital: David Watson, Jeanette Ryde, Ade Rotowa, Catharina Schram. Royal Bolton Hospital: Ajmal Eusuf, Mel McNulty, Rizwan Khan, Maria Sinfield. Royal Bournemouth General Hospital: Martin Schuster-Bruce, Steve Morris, Bill Gransden, Tony Virgincar. Royal Brompton Hospital: Eva Zizkova. Royal Cornwall Hospital, Treliske: Cate Powell, Louise Dickinson, Joe Teape, Carol Richards. Royal Derby Hospital: Naresh Nandwani, Gill Ogden, Cathy Bratt, Em Wilkinson-Brice. Royal Hallamshire Hospital: Arthur Goldsmith, Jo Murray, Victoria West, Sue Dailly, Paula Shobbrook. Royal Lancaster Infirmary: David Highley, Lynne Wyre, Kim Wilson, Jackie Holt. Royal Manchester Children's Hospital: Peter-Marc Forune, Anne Stanton, Katie McCall. Royal Preston Hospital: Craig Spencer, Denise Brooks, Sharon Hallam, Tom Owen, David Orr, Claire Horsfield, Sue Reed, Ian Donaldson. Royal Shrewsbury Hospital: Alastair Windsor, Debbie Millington, Patricia O'Neill. Royal Surrey Country Hospital: Mike Carraretto, Margaret Eaton, Christopher Tibbs, Susan Lewis. Royal Sussex County Hospital: Andew Hill, Marco Maccario, Julie Lloyd, Jackie Portsmouth, Karen Wright, Matthew Fletcher. Royal Victoria Infirmary: Ian Clement, Lisa Squires, Manjusha Narayanan. Russells Hall Hospital: Michael Reay, Sarah Raybould, Denise McMahon. Salford Royal Hospital: Murad Ghrew, Angela Neumann, Samantha Westwell, Ann Trail, Steve Waldek. Sandwell Hospital: Jana Bellin. Scarborough General Hospital: Jo Jaidev, Sylvia Wrigglesworth, Sue Marquis, Mark Andrews. Scunthorpe General Hospital: Jerry Thomas. Sheffield Children's Hospital: Jeff Perring, Liz Murch, Derek Burke. South Tyneside District Hospital: Christopher Muench, Lorraine Spence, Carole Clark, David Shilton. Southampton General Hospital: Mike Grocott, Iain Macintosh, Laura Armstrong, Melanie Griffiths, Julie Brooks, Sarah Jeremiah, Judy Gillow. Southend Hospital: Blanca Boira, Teresa Sage, Stephen Barret, John Gilham. Southmead Hospital: Jasmeet Soar, Deborah Munro, Mariann Charlton. Southport & Formby District General Hospital: Sue Pieri-Davies, Michael Vangikar, Joyce Jordan, Martin Kiernan, Liz Yates. St George's Hospital, Tooting: Andrew Rhodes, Linda Murdoch, Deborah Dawson, Carol Kennelly, Peter Riley, Mike Bailey. St Helier Hospital: Larry Mulleague, Emma Conroy, Caroline Betts, Richard Varhegyi, Steve Hyer. St James's University Hospital: Stuart Murdoch, Karen Ledgard, Innes Reid, Juliette Cosgrove. St Mary's Hospital: Mehringise Cooper, Sonia Broadby. Stafford Hospital: John Hawkins, Christine Dooley, Debra Adams. Stepping Hill Hospital: Karen Szarfenberg, Sengottiyan Chandrasekaran. Sunderland Hospital: Alistair I Roy, Gillian Ferguson, Julie McHugh, Les Boobis. The Christie: Phil Haji-Michael, Angela Hayes, Oonagh McGugan. The Great Western Hospital: Chris Beeby, Liz Jaffray, Hilary Munube, Ruth McCarthy. The Ipswich Hospital: Andy Kong, Angela Statham, Tina Johnson, Peter Donaldson. The James Cook University Hospital: Fiona Hampton, Nicola Cree, Maria Jones, Chris Harper, Clare White, David McCaffrey, Mike Bramble, Tricia Hart. The Princess Royal Hospital: David Christmas, Stephanie Young, Carol Woods, Debbie Snooke, Steve Evans. The Queen Elizabeth Hospital: John Gibson, Katherine Wong, Lynne Liebowitz, Geoff Hunnam. The Royal London Hospital: Marie Healey, Suzanne Daniels, Michael Millar, Charles Gutteridge. The Royal Marsden Hospital: Dr Timothy Wigmore, Mr Rob Loveland, Ms Jennifer Watson, Ms Rebecca Martirani, Shelley Dolan. The Royal Oldham Hospital: Chithambaram Veerappan, Oliver Robinson. The Whittington Hospital: Andrew Badacsonyi, Breege Gilbride, Julie Andrews, Deborah Wheeler, Siobhan Harrington. Trafford General Hospital: John Barnes, Elaine Deay, Wayne Goddard, Shirley Smith. University College Hospital: Viki Mitchell, Deborah Smyth, Mary Azarcon, Geoff Bellingan. University Hospital, Coventry: Andrew Phillips, Julius Asante-Siaw, Elaine Clarke, Karen Bond, Tracey Fenwick, Kate Prevc, Ann-Marie Cannaby. University Hospital Aintree: Christopher Grant, Sharon Smith, Rick Catlin, Gary Francis. University Hospital Lewisham: Marthin Mostert, Sally Rowe, Debbie Flaxman, Claire Champion. University Hospital of Hartlepool: Sue Smith, Julie Olsen, Vijay Gupta, Louise Legg. University Hospital of North Tees: Vijay Gupta, Andrea Mockler, Julie Olsen, Sue Smith. Walton Centre: Chris Whitehead, Carole Scott, Phil Kane, Karen Dawber. Wansbeck Hospital: John Laurenson, Elizabeth Carr, Tamsin Oswald, David Evans. Warrington Hospital: Jerome McCann, Ellis Clarke, Andrew Sargent, Kathryn Holbourn. Warwick Hospital: Ian Purcell, Christine Georgeu, Steve Mather. Watford General Hospital: Thomas Stambach, Sarah Laferby, Frances Stratford, Russell Harrison. West Cumberland Hospital: Fiona Graham, Jackie Fox, Clive Graham. West Middlesex University Hospital: Amandeep Gupta, Jose Tomas, Elaine Danns. West Suffolk Hospital: Michael Palmer, James Whatling, Sue Partridge, Nichole Day. Wexham Park Hospital: Helen Challand, Lucy Everett. Whiston Hospital: Francis Andrews, Paul Jeanrenaud, Kim Sims, Josephine Keward, Mike Lynch. Worcestershire Royal Hospital: Gareth Sellors, Shelly Goodyear, Jane Stockley, Steve Graystone. Worthing Hospital: Ryck Albertyn, Janice Bates, Phillip Barnes. Wycombe and Stoke Mandeville Hospital: Richard Bunsell, Ann Ashworth, Jean O'Driscoll, Graziano Luzzi. Wythenshawe Hospital: Andrew Bentley, Gary Brear, Jane Clayton, Hayley Hardiman, AnneMarie Aziz, Meryl Graves, Amanda Bailey. Yeovil District Hospital: Jeremy Reid, Mark Robinson, Rachael Grey, Susan Jones. York Hospital: Rinus Pretorius, Anne Knaggs, Christine Cruise, Libby McManus.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors All collaborators are listed in the appendix. All authors contributed to the design and execution of the study, and all contributed to the interpretation of results.
-
Funding The Department of Health provided some analytical (data processing) assistance at the end of the study. The National Patient Safety Agency was responsible for directing the study. Statistical analysis was provided by the Intensive Care National Audit and Research Centre. Statement of independence of researchers from funders: the statistical analysis and clinical interpretation of results of the study was performed independently of the Department of Health.
-
Competing interests None.
-
Ethicas approval The National Research Ethics Committee waived the requirement for informed patient consent on the basis that the intent was to improve uptake of established best practice care, and no patient-identifiable information would be collected centrally.
-
Open Access This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/